
Abstract
Purpose:
To compare the number of antiretroviral-related clinically significant drug–drug interactions (CSDDIs) occurring in hospitalized patients that were intervened upon before and after Antiretroviral Stewardship Program (ARVSP) expansion and to classify the interventions made to prevent errors.
Methods:
A retrospective chart review of adult patients treated with antiretroviral therapy (ART) and who were hospitalized from September 2012 to February 2013. A CSDDI was defined as requiring an alternative therapy, dose adjustment, or schedule modification. Findings were compared to a prior study.
Results:
A total of 185 admissions were included and 76 CSDDIs were identified, 19 (25%) occurred after ART approval. The percentages of CSDDIs that occurred after ART approval and were intervened upon before and after ARVSP expansion were 43% and 95%, respectively (P < .001). An additional 80 other interventions were made by the ARVSP.
Conclusion:
An ARVSP is critical in the prevention of CSDDIs and errors to improve safety in HIV-infected patients.
Background
In the United States, over 1 million people are infected with HIV, and about 50 000 Americans are newly infected each year. 1,2 With the advent of antiretroviral therapy (ART), HIV-related morbidity and mortality have significantly decreased, requiring the management of other chronic comorbid conditions for this aging population. 3,4 Subsequently, HIV-infected individuals treated with ART are at a higher risk of polypharmacy, drug–drug interactions, and medication errors, especially when hospitalized. Incidence of antiretroviral-related errors in hospitalized patients have been reported as high as 70%. 5 –7 Most commonly reported errors include contraindicated combinations, incorrect doses, incomplete regimens, and lack of dosage adjustments based on renal and/or hepatic function. 5 –11 Such medication errors in HIV-infected individuals can increase the risk of resistance due to potential suboptimal ART as well as increase the risk of drug toxicity due to drug–drug interactions causing elevated drug concentrations.
At a 464-bed tertiary care facility located in Brooklyn, New York, all antiretroviral drugs are restricted and require approval by an infectious disease attending or a clinical pharmacist through the Antiretroviral Stewardship Program (ARVSP). The ARVSP, available 24 hours per day and 7 days per week, was established to ensure safe and timely continuation of ART. Upon hospital admission of an HIV-infected person, the medical team consults an infectious disease attending or the ARVSP for ART approval. The ARVSP consult entails direct patient interviewing by a clinical pharmacist to assess a patient’s antiretroviral regimen, compliance, and pertinent laboratory results. If the clinical pharmacist approves the ART, medication orders are screened for drug–drug interactions and necessary dosage adjustments are made before entering the ART into the computerized order entry system. Additionally, the clinical pharmacist evaluates the need for opportunistic infection prophylaxis. A credentialed HIV clinical pharmacist supervises all of the ARVSP’s consults. All consultations are documented in the hospital’s electronic medical record system and an internal clinical pharmacy database. The ARVSP receives approximately 400 consultations annually. This service eliminates many of the errors reported in the current literature, such as incomplete regimens, incorrect doses, and lack of dose and/or frequency adjustments.
An internal retrospective chart review was conducted on patient admissions between November 2010 and January 2012 to quantify the number of antiretroviral-related clinically significant drug–drug interactions (CSDDIs) occurring in hospitalized patients and to assess the ARVSP’s ability to identify and intervene upon drug interactions. The study by Bias et al revealed a 33% incidence of CSDDIs, where 73% occurred upon admission within the first 24 hours and 27% occurred during the remainder of hospitalization, after the initial 24 hours. The ARVSP identified and intervened upon 80% of the CSDDIs upon admission; however, 57% of the CSDDIs during the remainder of hospitalization were missed. 11 These findings prompted the ARVSP to expand its services by assigning a clinical pharmacist to conduct daily medication and laboratory reviews of HIV-infected patients after initial ART approval and until hospital discharge.
The primary objective of this study was to compare the number of antiretroviral-related CSDDIs occurring in hospitalized patients that were intervened upon before and after the assignment of an ARVSP clinical pharmacist to perform daily reviews. Secondly, this study was conducted to classify the interventions made by the ARVSP to prevent medication errors in HIV-infected patients.
Methods
Setting and Patients
This study was a single-center, retrospective chart review conducted on patient admissions between September 2012 and February 2013. Patients were included in the study if they were 18 years of age and older, diagnosed with HIV or AIDS, and receiving ART while hospitalized. Patients were excluded if an infectious disease attending approved ART and the ARVSP was not consulted. This study received approval by the institutional review board.
Definitions
A CSDDI was defined as an interaction between an antiretroviral agent and a concomitant medication requiring an alternative therapy, a dose adjustment, or a schedule modification. Upon admission was defined as occurring at the time of computerized order entry of ART, typically within the first 24 hours of hospitalization. During the remainder of hospitalization was defined as occurring after the time of initial order entry of ART, typically after 24 hours, and until patient discharge. The CSDDIs were considered intervened upon by the ARVSP if the electronic medical record or internal clinical pharmacy database had documentation of the recommendation and medication orders were changed accordingly.
Data Collection
Medication profiles were screened and cross-referenced for CSDDIs using 3 different sources: (1) the Department of Health and Human Services Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents, (2) the Liverpool HIV drug reference, and (3) the Micromedex drug database. These resources are frequently updated and serve as comprehensive tools to identify medication errors with ART. The following data were collected for each CSDDI: timing (upon admission or during the remainder of hospitalization), type (alternative therapy, dose modification, or frequency adjustment), interacting antiretroviral and concomitant agent, and whether or not the ARVSP intervened. Multiple hospital admissions for a single patient during the study period and multiple CSDDIs for a single inpatient admission were included in the analysis.
Statistical Analysis
The primary end point of this study was the difference in the number of antiretroviral-related CSDDIs that occurred during the hospitalization and were intervened upon before and after ARVSP expansion of monitoring HIV-infected patients daily. Secondary end points included the quantity and classification of all antiretroviral-related CSDDIs, the difference in the number of antiretroviral-related CSDDIs that occurred upon admission and were intervened upon before and after ARVSP expansion, and the quantity and classification of interventions in addition to antiretroviral-related CSDDIs made by the ARVSP. The findings of a prior internal study, from before ARVSP expansion, were used as the comparative cohort. Categorical data were expressed as frequencies and percentages according to descriptive statistics, and continuous data were expressed as means with standard deviations. The Fisher exact test was used to compare categorical data and the student t test was used to analyze continuous data to the findings of the comparative cohort. Differences were considered statistically significant if the P value was less than .05.
Results
A total of 185 admissions met the inclusion criteria. Hospitalized patients were 51 ± 11.9 years old and the majority were females who had an undetectable viral load, versus the comparative cohort that had a majority of males who had a detectable viral load (Table 1). There were 76 CSDDIs identified, 57 upon admission and 19 during the remainder of hospitalization. This indicates a CSDDI incidence rate of 2 in every 5 patient admissions and 1 out of 4 occurring during hospitalization, similar to the comparative cohort (Figure 1). Of the interactions that occurred upon admission, 56 (98%) were intervened upon by the ARVSP and of those that occurred during the remainder of hospitalization, 18 (95%) were intervened upon. In relation to the percentage of CSDDIs that occurred during the remainder of hospitalization and were intervened upon in the comparative cohort, there was an absolute difference of 52% with a P value of <.001. Comparing the percentage of CSDDIs that occurred upon admission and were intervened on, there was an absolute difference of 18% with a P value of <.001 (Figure 2).

Incidence and timing of antiretroviral-related clinically significant drug–drug interactions (CSDDIs). The percentages of antiretroviral related CSDDIs that occurred during the remainder of hospitalization in the November 2010 to January 2012 and September 2012 to February 2013 cohorts were 27% and 25%, respectively (P = .86).

Difference in antiretroviral-related clinically significant drug–drug interactions (CSDDIs) identified and intervened upon. The percentages of missed antiretroviral-related CSDDIs that occurred during the remainder of hospitalization in the November 2010 to January 2012 and September 2012 to February 2013 cohorts were 57% and 5%, respectively (P < .001). The percentages missed upon admission were 20% and 2%, respectively (P < .01).
Patient Characteristics.
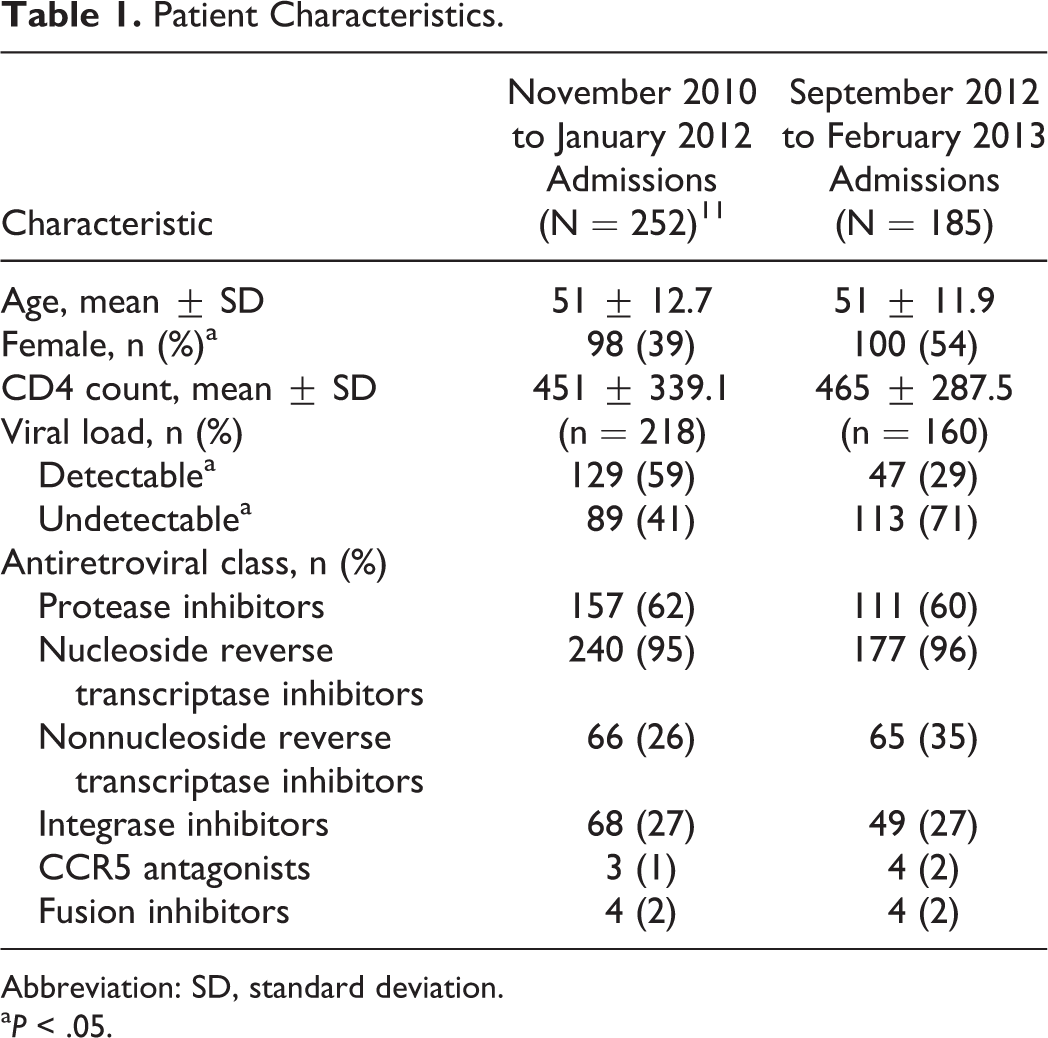
Abbreviation: SD, standard deviation.
a P < .05.
The leading type of CSDDIs was requirement of alternative therapy (76%) followed by dose adjustment (13%) and drug schedule modification (11%). Protease inhibitors were associated with a majority of the CSDDIs (79%) identified and the remaining were associated with nonnucleoside reverse transcriptase inhibitors. Acid-suppressive therapy (eg, proton pump inhibitors, histamine-2 receptor antagonists, and antacids) was the causative agent in 53% of the CSDDIs, followed by 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase inhibitors or statins (30%).
In addition to antiretroviral-related CSDDI interventions, there were 80 other interventions made by the ARVSP. Interventions included calculating and expediting zidovudine (ZDV) dosing for pregnant females in labor, renal dose adjustments of medications including antiretroviral drugs, initiation or discontinuation of opportunistic infection prophylaxis and treatment, and recommendations for alternative therapy or to discontinue therapy (Figure 3).
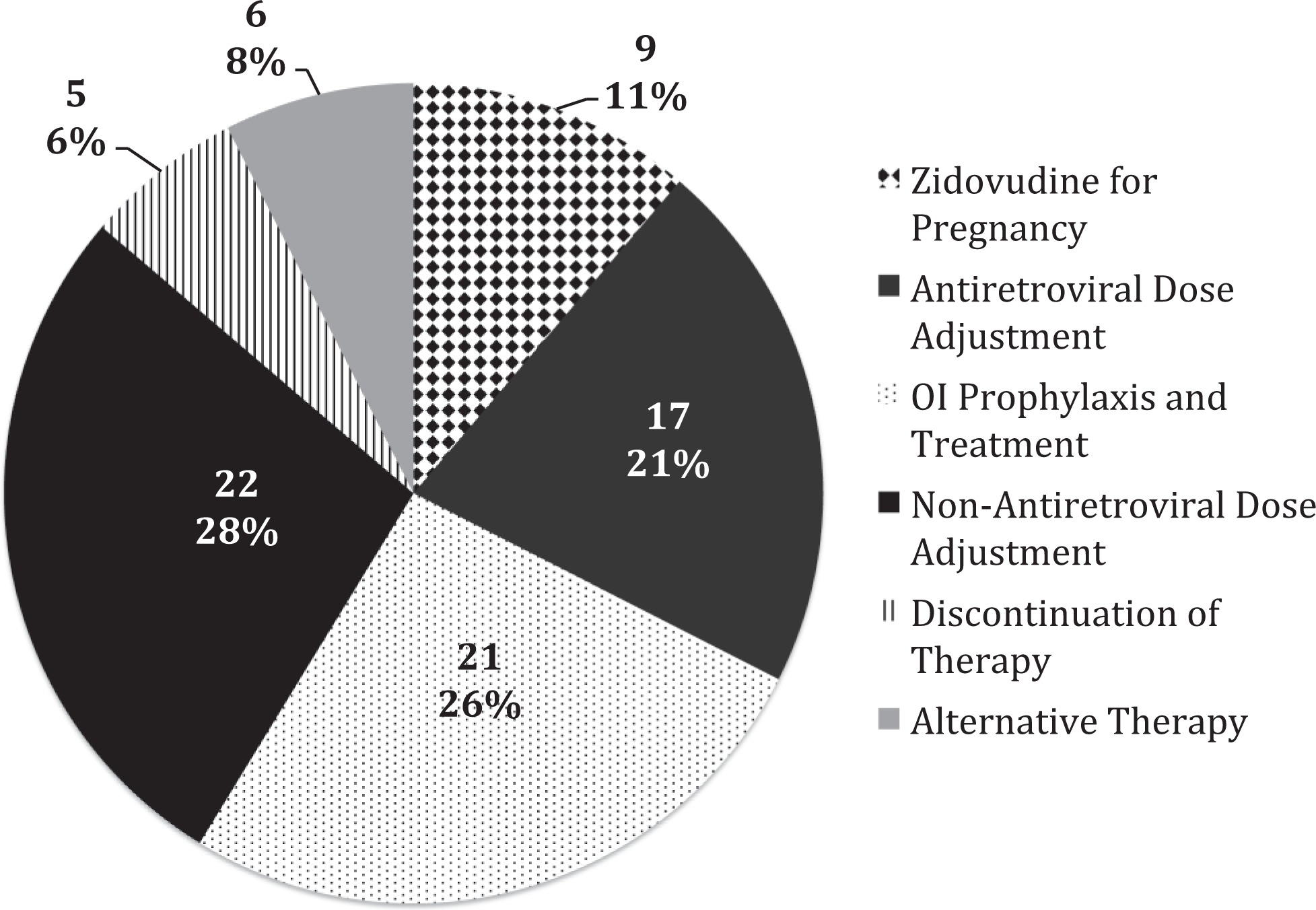
Additional interventions by the Antiretroviral Stewardship Program (ARVSP). ARVSP clinical pharmacists made an additional 80 interventions that were documented between September 2012 and February 2013. Nonantiretroviral and antiretroviral dose adjustments accounted for 28% and 21% of these interventions, respectively. These dose adjustments included changes needed for renal function. Opportunistic infection (OI) prophylaxis and treatment intervention included the initiation or discontinuation of either prophylaxis (n = 19) or treatment (n = 2) for HIV-infected patients. Zidovudine (ZDV) for pregnancy included calculating doses and expediting orders for initial bolus and subsequent continuous infusion of ZDV for HIV-infected women in labor. Discontinuation of therapy included duplicate therapy (n = 3) and therapy without an indication (n = 2). Alternative therapy interventions included those not due to antiretroviral-related CSDDIs.
Discussion
The expanded ARVSP, which included assignment of clinical pharmacists to monitor HIV-infected patients daily throughout hospitalization, significantly decreased the incidence of antiretroviral-related CSDDIs. Only 2 CSDDIs were missed throughout this entire study, a single interaction upon admission and a single interaction during the remainder of hospitalization. The CSDDI missed upon admission was a simvastatin order for a patient treated with protease inhibitors; however, the patient was not discharged with a prescription for simvastatin. The CSDDI missed during the remainder of hospitalization was for an intranasal fluticasone order for a patient treated with protease inhibitors. The order for fluticasone was placed in the evening and the patient was discharged the next morning prior to the clinical pharmacist’s daily review.
In the comparative cohort, a majority of the CSDDIs missed during the remainder of hospitalization were due to an order set including acid-suppressive therapy for HIV-infected patients admitted to the detoxification service. 11 As a result of these findings, the ARVSP pharmacists ensured that orders for atazanavir (ATV) and rilpivirine with concomitant acid-suppressive therapy were appropriately spaced apart, which contributed to the 52% reduction in missed CSDDIs.
Many of the CSDDIs identified in this study were due to statins and acid-suppressive therapy, which is consistent with the current literature. 5,9 –11 At our institution, the preferred statin is simvastatin followed by rosuvastatin, which is restricted except for patients concomitantly treated with cytochrome 3A4 inhibitors or inducers and for cardiac order sets. When a physician orders a nonformulary statin for a patient, the order entry automatically prompts conversion to simvastatin. Since all antiretroviral drugs are restricted and require approval, medical teams tend to order statin therapy prior to ART approval and enter simvastatin. Educating the medical team to postpone order entry of statin therapy for an HIV-infected patient until after ARVSP consultation may help prevent the incidence of this type of CSDDI. As for acid-suppressive therapy, education on appropriate administration of stress ulcer prophylaxis for inpatients may help prevent the continued occurrence of this type of CSDDI.
The difference in baseline characteristics of sex and viral load between this study and the comparative cohort is not expected to impact the number of antiretroviral-related CSDDIs identified. Sex and viral load do not affect the use of acid-suppressive therapy or statins, the main causative agents for the antiretroviral-related CSDDIs identified. Besides intervening upon antiretroviral-related CSDDIs, clinical pharmacists were able to make several other types of interventions to decrease overall medication errors and increase patient safety through the ARVSP.
Limitations
Different clinical pharmacists were conducting the ARVSP service between this study and the comparative cohort, which could potentially account for some of the difference in the number of CSDDIs intervened upon throughout patient hospitalizations. Additionally, this study did not include ART approvals made by an infectious disease attending, which could have unaccounted CSDDIs. Another limitation is the unknown actual patient harm and/or clinical benefit of these CSDDIs and interventions. This study was conducted at a single-center hospital that has an in-house clinical pharmacotherapist-on-call service available 24 hours per day and 7 days per week that tertiary hospitals may not be able to replicate.
Conclusion
Clinically significant drug-drug interactions are common among hospitalized HIV-infected patients, and clinical pharmacists evidently play a significant role in decreasing the number of CSDDIs missed throughout patient hospitalization. Antiretroviral Stewardship Programs, including antiretroviral restriction and continued daily monitoring by clinical pharmacists, are critical for the prevention of not only drug interactions but also other medication errors to improve safety in HIV-infected patients.
Footnotes
Acknowledgments
The authors sincerely thank the clinical pharmacists of the 24-hour on-call program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.