
Abstract
Background:
There are few validated tools to measure stigma, particularly among children living with HIV and their families.
Methods:
This study was nested within a larger study that followed 240 child–caregiver dyads (children aged 10-15 years) at 8 clinics in western Kenya. The stigma instrument was administered to all child–caregiver dyads at 2 time points 6 months apart. The primary end point was to construct validity assessed by comparison to criterion constructs using generalized estimating equation models.
Results:
Mean age of child participants was 12.3 years and 52% were female. Generally, caregivers reported experiencing higher levels of HIV stigma compared to their children. Children (9%) and caregivers (14%) reported that HIV stigma made them feel stressed, anxious, and depressed. Child and caregiver stigma items showed high construct validity by emotional and behavioral outcomes.
Conclusions:
The stigma instrument showed high validity when compared to emotional and behavioral outcomes.
What Do We Already Know About This Topic?
HIV stigma is a major barrier to all aspects of HIV testing and treatment, but there are few validated tools to measure stigma among children living with HIV.
How Does Your Research Contribute to the Field?
Using a mixed-methods approach, we developed and tested a grounded stigma instrument among children living with HIV in western Kenya, which showed good construct validity with relevant emotional and behavioral outcomes.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Our research demonstrates that it is possible to develop a simple, low-cost questionnaire to identify children experiencing HIV-related stigma in a clinical setting who can be targeted for additional intervention or services.
Introduction
HIV-related stigma is an important barrier to all aspects of HIV prevention and treatment, including delayed HIV testing and enrollment in care, 1 –3 increased risk of not being retained in care, 4 –6 nonadherence to antiretroviral therapy (ART), 7 –10 and higher likelihood of nondisclosure to partners. 11,12 The negative impact of HIV stigma on psychosocial health, such as depression, anxiety, and decreased quality of life (QoL), has also been noted. 13 –16 Unfortunately, the literature on HIV stigma has been heavily skewed toward adults living with HIV and has not adequately considered the impact of stigma on children and adolescents living with HIV, most of whom reside in sub-Saharan Africa. 17
An estimated 1.8 million children younger than 15 years are living with HIV, with less than half accessing ART. 18 Children living with HIV may be at substantial risk of HIV stigma and its deleterious effects on HIV treatment and psychosocial health in ways both similar and distinct from adults. For example, perinatally infected children are at higher risk for stunted growth and delayed bodily development, and these differences in appearance may be a source of anxiety and internalized stigma or increase risks for social isolation and discrimination. Studies suggest that HIV stigma encountered from peers at school in the form of taunting, gossiping, or bullying, either because of the child’s own status or the status of a family member, are formative experiences for HIV-infected and affected youth 19 –22 and may lead to problems in school attendance or accessing peer support networks. 23 –25 Moreover, children may be affected by HIV stigma experienced at the caregiver level, which has been shown to negatively impact HIV-infected children, 26 –28 including caregivers delaying giving children medicines or taking them to clinical care. 29 –31 Generally, HIV stigma has been hypothesized to exacerbate poverty, malnutrition, and access to services for HIV-affected families. 32 –34
As more children access treatment, survive into adolescence, and transition into adult care settings, they must learn about their HIV status. Parents and caregivers of children with HIV often report that disclosure to children will improve ART adherence, 35 –44 increase the child’s long-term engagement in care, 35,38 –42,44 –46 and equip the child to protect himself or herself and others from HIV. 39,43,47 On the other hand, the potential negative impacts of HIV stigma weigh heavily in decisions about disclosure. Studies frequently cite parents’ and caregivers’ fears that the child will subsequently disclose his or her HIV status to others, 38 –41,44,46,48 –50 leading to potential stigma and social isolation for the child as well as the family. 38,40,41,44,45,49
A major barrier to investigating the prevalence and impacts of HIV stigma among children living with HIV and their families, as well as evaluating interventions to combat stigma, is the lack of reliable and valid stigma measures, particularly in resource-limited settings. 51 –53 Several authors of this paper (blinded) previously undertook a systematic review of measures of HIV stigma among HIV-infected and affected children. 54 Among 27 articles describing quantitative HIV stigma measures for HIV-infected and affected youth younger than 18 years, only a handful explicitly evaluated the validity of stigma measures using rigorous methods to ensure content validity, internal consistency, and construct validity, with most studies modifying existing measures such as the HIV Stigma Scale developed among adults in the United States. In this article, we report the results of the SAFI (Stigma in AIDS Family Inventory) validation study that aimed to systematically evaluate a culturally adapted, developmentally appropriate measure to assess HIV stigma experienced by children living with HIV and their caregivers in western Kenya.
Methods
Study Design
We conducted a multiphased validation study to develop and test a reliable, valid instrument to measure HIV stigma among children living with HIV and their families. In the first phase, we constructed a questionnaire for children and their caregivers. A potential set of questionnaire items were identified through a systematic review of existing questionnaires and other methods used for pediatric HIV stigma measurement. 54 We utilized a conceptual framework that assumes people living with HIV (or caring for those living with HIV) may experience 4 types of HIV stigma that operate in subtle but in distinctive ways. Perceived and enacted stigma are characterized by the fear that HIV stigma and discrimination may occur and the belief that it has occurred, while internalized stigma captures negative beliefs among oneself because of their HIV status. 55,56 A fourth type of stigma, courtesy stigma, describes stigma and discrimination directed at an individual who is associated with or attending to someone who is living with HIV (but not necessarily infected themselves), which has important consequences for families caring for infected children. 57 We incorporated these various dimensions of stigma into the stigma questionnaire.
Adaptation of stigma questionnaire items in the literature and the conceptual framework to the local setting and population were informed by focus groups with children living with HIV and caregivers of HIV-infected children (results published elsewhere), as well as cognitive interviews with children and caregivers to test and maximize face validity of items. The final set of stigma questionnaire items was translated from English to Kiswahili by a trained translator and then back-translated into English, repeating this process until items were consistent. Following recommendations for cross-cultural test adaptation, 58 a team of multicultural and multilingual experts reviewed the translations and assessed items for cultural sensitivity and intercultural communication. This team has extensive qualitative research methods and instrument validation and cross-cultural adaptation expertise in this setting, particularly related to pediatric adherence to treatment and disclosure of HIV status in which issues of stigma are prominent. 31,44,59 –64
The resultant questionnaire, known as the SAFI Stigma questionnaire, asks a series of questions regarding the stigma and discrimination that an individual experiences because of his/her own or someone in their families’ HIV status. Participants were instructed to respond to an experience as having “never happened” or “ever happened.” If “ever happened” was selected, the participant was then prompted to describe the time frame in which the experience happened, categorized as either in the “past 6 months” or “longer than 6 months ago.” Many of the question prompts are led by the statement, “Because I have HIV or someone else in my family has HIV…”
In the second phase, which are reported here, we tested the reliability and validity of the HIV stigma questionnaire items (child and/or caregiver stigma questionnaires provided on request). Reliability and validity testing was nested within a cluster, randomized, prospective cohort study to evaluate a disclosure counseling intervention. The study followed 240 families with HIV-infected children aged 10 to 15 years for 2 years at 8 clinics (∼35 children per clinic), who are part of the Academic Model Providing Access to Healthcare (AMPATH) in western Kenya, one of the largest HIV care providers in sub-Saharan Africa. 65,66 Informed consent was required from all of the child participants’ parents or guardians, and assent was also required from all child participants. Study assessments were conducted at baseline and every 6 months thereafter, which included clinical characteristics (WHO disease stage, CD4 counts, and viral load) and various questionnaires administered by research assistants assessing disclosure status, adherence to treatment, behavioral and mental health, and QoL. Child participants were also issued Medication Event Monitoring Systems (MEMS® Cap, WestRock, Atlanta, USA) caps for electronic dose monitoring. Baseline characteristics of this cohort and study methods, including the various assessments and how they were interpreted, are published elsewhere. 67 The stigma questionnaire was administered (in English or Kiswahili, depending on participant preference) to all children and their caregivers at the final 2 routine study evaluations (month 18 and 24) alongside the other assessments. Due to the fact that the stigma questionnaire specifically references HIV, only children who were disclosed and knew their HIV status were administered the stigma questionnaire (all caregivers were administered the questionnaire). At month 18 and 24, 126 and 155 children were administered the stigma questionnaire, respectively. Data were collected from October 2014 to June 2015.
Ethical Statement
The study was approved by the institutional review board of Indiana University School of Medicine (Protocol #1206009036) in Indianapolis, Indiana, and the Moi University/Moi Teaching and Referral Hospital Institutional Research and Ethics Committee (Approval #000872) in Eldoret, Kenya. All study participants aged 18 years and older provided informed consent prior to enrollment. For children younger than 18 years, we obtained assent as well as informed consent from their guardian according to local laws and guidelines. Research participants were provided with a small stipend (about US$3) per study assessment to compensate them for their travel and time. To reduce the risk of accidental disclosure of HIV status to children, research assistants underwent additional training before consenting and assessing study participants, which included modules on disclosure assessment protocols, confidentiality, and privacy. Additionally, research assistants were trained to refer any participants whom they deemed to be demonstrating significant psychiatric distress. A specific mental health study referral form was created to document and refer participants for mental health services.
Analysis
Descriptive statistics and item analysis of the participants’ responses to stigma measurement items were conducted, including item response distribution, item discrimination indices, and item-scale correlation. Test–retest reliability was assessed for individual stigma items at the 2 time points for stigma items administered to children and separately for stigma items administered to caregivers. We also examined the agreement between child and caregiver responses to individual stigma items that were sufficiently similar (a total of 8 items), which was assessed using κ statistics. The primary end point of the validation study was construct validity, which was assessed by comparison to primary criterion constructs using generalized estimating equation (GEE) models. These GEE models allowed for the modeling of repeated measures across visits, gave the ability to accurately model the covariance structure to ensure the best fit, and allowed for the use of distributions within the exponential family, to model nonlinear data. Primary criterion constructs were adherence to treatment, QoL, behavioral health, depression, and clinical characteristics. Adherence was assessed using a previously validated questionnaire in this setting that asks about missed and late doses as well as barriers to adherence. 59,60 In addition, participants were issued electronic dose monitors (MEMS) that recorded a time and date stamp each time the bottle was opened. Quality of life was assessed using the multidomain Pediatric AIDS Clinical Trials Group General Health Assessment for Children (GHAC) QoL questionnaire developed by the Pediatric AIDS Clinical Trial Group. The GHAC was constructed through previously validated measures with good internal consistency, reliability, and validity. The modular, age-specific GHAC instrument for children measured the QoL on the following 5 domains: general health, physical functioning, symptoms, psychological well-being, and social and role functioning. Each domain of the GHAC is scored separately on a Likert scale, with scaled scores ranging from 0 to 100, with higher scores indicating better QoL. 68 –70 Behavioral health was assessed using the 25-item Strengths and Difficulties Questionnaire (SDQ)–Youth Version, 71,72 which consists of 5 scales that measure difficulties in 5 psychological domains: emotional symptoms, conduct problems, hyperactive-inattention, peer relationship, and prosocial behavior. Participants are asked to rank their behaviors as “not true,” “somewhat true,” or “certainly true.” Depression was assessed using the Patient Health Questionnaire–9-item (PHQ-9) depression instrument, 73 a 9-item module adapted from the full PHQ assessment and provides diagnosis of probable depression and assesses severity of symptoms. Participants are asked to report how often they have experienced depressive symptoms over the last 2 weeks, on a scale of 0 (not at all) to 3 (nearly every day). The PHQ-9 has demonstrated high internal reliability. Patient responses to the GHAC, 69,74,75 SDQ, 71,72 and PHQ-9 76 were scored and transformed consistent with the published literature. Linear (for continuous outcome variables) and logistic (for dichotomized variables) regression models were used for validating stigma items against criterion constructs, while accounting for key demographic variables. Demographic and clinical characteristics were extracted from the participants’ medical chart using a standardized clinical data extraction tool.
Results
Participants’ Characteristics
At study baseline, mean age of child participants was 12.3 years and 147 were female (52%), with the majority of caregiver participants being the biological mother of the child (54%), as well as a number of aunts/uncles (19%), biological fathers (17%), and grandparents (11%; Table 1). About half of children were total orphans (ie, both their mother and father were deceased) and a fifth has a sibling who was also living with HIV. Adherence monitoring using MEMS revealed only 28% of children were able to sustain >90% of doses taken over the follow-up period, with median adherence of 70% of disease taken.
Participants’ Characteristics.

Abbreviations: IQR, interquartile region; MEMS, Medication Event Monitoring Systems; SD, standard deviation.
Responses to the Stigma Questionnaire
Child and caregiver participants’ responses to stigma items are provided in Table 2. A small proportion of children (ie, less than 10%) responded that they had lost friends due to their HIV status, had been bullied or insulted, experienced HIV-related discrimination, and had lost social support. More children, although still a minority, reported that their HIV status had made them feel stressed or anxious (9% at month 24) or depressed or sad (9% at month 24). Almost half of the children (45%) reported that it was important to keep their HIV status a secret (45%), but only 11% reported that they delayed taking their HIV medications so others would not see them. Caregivers reported slightly higher levels of stress or anxiety (13% at month 24) and depression or sadness (14% at month 24) due to their child’s HIV status. Moreover, caregivers were more likely to report other forms of stigma and discrimination that they experienced. For example, while 11% of caregivers reported being called names or bullied due to the child’s HIV status, only 3% of children reported these experiences, and 10% of caregivers reported experiencing discrimination in the neighborhood compared with only 2% of children. Caregivers were also much more likely to report thinking that people in the community think HIV is a dirty or immoral disease, with 21% reporting a few people think that and 19% reporting most people think that.
Responses to Stigma Items.

Reliability and Construct Validity
Test–retest reliability was high; responses by both children and caregivers on individual stigma items were highly consistent from month 18 to month 24 (agreement was >90% for the majority of stigma items). Child and caregiver stigma items showed high construct validity, with the SDQ and caregiver stigma items showed high construct validity with the GHAC General Health (Table 3). Several caregiver stigma items also showed construct validity with MEMS adherence and viral load. No child or caregiver stigma items were significantly associated with child- or caregiver-reported adherence using the CAMP Adherence Questionnaire, depression using the PHQ-9 questionnaire, or any GHAC domains outside of General Health (ie, no items correlated with physical functioning, psychological functioning, social and role, HIV, and health care).
Association of Stigma Questionnaire Items with Relevant Constructs.a

Abbreviations: GHAC, General Health Assessment for Children; MEMS, Medication Event Monitoring Systems; PHQ-9, Patient Health Questionnaire–9 item; SDQ, 25-item Strengths and Difficulties Questionnaire.
a± indicates direction of the slope for stigma items significantly associated with construct (P < .05). No stigma items were significantly associated with child- or caregiver-reported adherence using the CAMP Adherence Questionnaire or depression using the PHQ-9 questionnaire. Several stigma items were associated with the GHAC but only within the General Health subdomain (ie, no significant association with the other domains—physical functioning, psychological functioning, social and role, HIV, and health care).
On the child questionnaire, stigma items that showed high construct validity with the SDQ included experiencing discrimination at home due to HIV, losing social support, feeling stressed/anxious due to HIV stigma, feeling depressed/sad due to HIV stigma, and hopes for the future changing in a negative way due to HIV. Similar but not identical stigma items on the caregiver questionnaire showed high construct validity with the SDQ, including being called names/insulted due to the child’s HIV status, losing financial support/work due to the child’s HIV status, feeling depressed/sad due to HIV stigma, and that the child’s future hopes had changed in a negative way. All child and caregiver stigma items showed high construct validity in the same “direction”—that is, child and caregiver reports of stigma/discrimination or its negative effects on the stigma questionnaire were associated with poorer total difficulties scores on the SDQ (poorer emotional and behavioral health). Five caregiver stigma items showed high construct validity, with the GHAC General Health domain in the same direction as the results above. These items were related to feeling depressed/sad due to HIV stigma (which also showed validity with the SDQ), the child being isolated due to their HIV status, the child experiencing discrimination at home or at school, and HIV discrimination affecting the child’s education.
Agreement Between Child and Caregiver Responses
There were 8 items on the child and caregiver questionnaires that asked about HIV stigma that the child had experienced with the items being sufficiently similar to compare child and caregiver responses. Agreement was fairly high (between 84% and 100%), but not all κ statistics were statistically significant (Table 4). Overall, caregivers were slightly more likely to report that their child had experienced stigma when compared to child self-reports. For example, at month 18, only 3% of children reported being called names or bullied due to their HIV status but 9% of caregivers reported their child was called names or bullied.
Agreement Between Child- and Caregiver-Reported Individual Stigma Items.
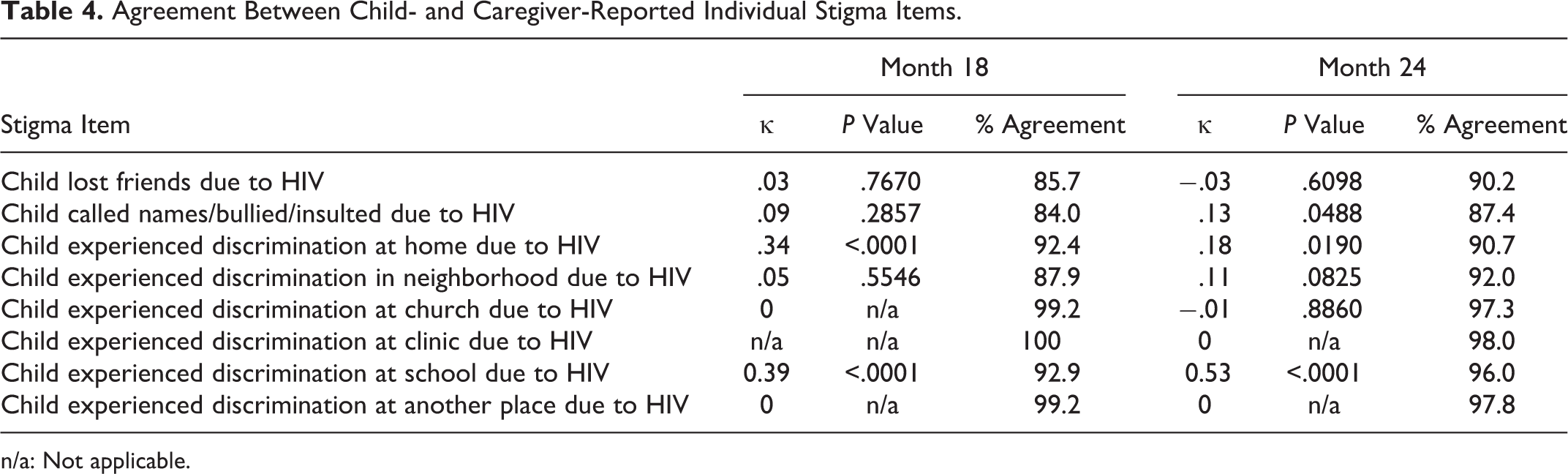
n/a: Not applicable.
Discussion
A minority but not insignificant proportion of children and caregivers reported fearing or experiencing HIV stigma among this cohort of families in western Kenya. Generally, caregivers tended to report high levels of both child-level and caregiver-level stigma. Our results support that the phenomenon of courtesy stigma, whereby caregivers may fear or directly experience stigma due to the status of their child (rather than their own status), is an important characteristic of HIV stigma in this setting, which can affect child outcomes both clinically and psychosocially. 77 Up to 1 in 10 caregivers in our cohort reported being negatively judged or isolated/avoided due to the child’s HIV status. In their qualitative study of HIV-related sigma in the United States, Bogart and colleagues referred to this phenomenon as the “interconnectedness of stigma experiences in families living with HIV.” 78 Our study supports the need for instruments to be attentive to the ways in which HIV stigma can impact families caring for children living with HIV.
The lower levels of stigma reports from children versus their caregivers deserve further investigation in this setting. Given many of the children’s younger age—average age was 12 years—it is possible that many children, even though they knew about their HIV status, were too young to recognize or connect their feelings and experiences to HIV-related stigma. It is also possible that because only children who were disclosed to were administered the questionnaire but all caregivers responded, the children who were yet to be disclosed to were more at risk of HIV stigma. Studies report a close association between caregivers’ fears of HIV stigma and nondisclosure to children, 62 which we also found in our own focus groups with caregivers in this setting. Finally, children in this setting may be reluctant to report their own internal or external experiences of HIV stigma; about half of children reported that they felt it was important to keep their HIV status a secret. This may extend to keeping their own feelings and experiences related to HIV stigma private. Among adolescents in high-income settings, staying silent and keeping secrets about their experiences of living with HIV in different social contexts (of which the clinic or research study is one) is an important adolescent practice as both a protective and self-care strategy. 79 How these silences may operate in the context of children and adolescents living with HIV in Kenya need to be further explored.
One of the most routinely reported outcomes by both children and caregivers related to HIV stigma was experiencing anxiety, stress, depression, and a negative outlook for the future. This is consistent with other studies that showed that HIV stigma is associated with increased risks for mental health issues in adults 80 –82 and adolescents. 83,84 Stigma items related to experiencing anxiety, depression, and negative outlook showed high construct validity with the SDQ, an instrument designed to measure emotional and behavioral symptoms. Surprisingly, no child or caregiver stigma items showed significant construct validity with the PHQ-9, a common depression screening instrument. Anecdotal evidence from the research team in Kenya that administered the questionnaires to children and their caregivers reported in debrief meetings their particular dissatisfaction with the PHQ-9 instrument and that participants were more likely to have difficulty understanding and responding to these items during study assessments.
The finding that caregiver stigma items showed high construct validity by the GHAC General Health domain but not child stigma items is interesting. The GHAC General Health domain asks about the child’s overall health, physical health, emotional health, and daily activities on a 10-point scale from very worst to very best. This finding may also be related to children’s unwillingness to disclose physical and mental problems related to their HIV status or to the lack of sensitivity of the particular measure. We did not find strong construct validity on stigma items by adherence to treatment in this study. Quantitative adherence monitoring using the gold standard of electronic dose monitoring (MEMS) revealed significant levels of missed doses (eg, only 28% of children achieved >90% doses taken during follow-up). Interesting, a study among Thai youths living with HIV found while stigma reported using the HIV Stigma Scale was not associated with adherence by quantitative assessment (visual analog scale), stigma was associated with poorer adherence and missed doses by qualitative assessment (in-depth interviews). 85 In qualitative work in this setting, we have also documented a strong association between HIV stigma and child adherence to HIV medication.
There are a number of important limitations of this study to consider. First, as noted earlier, one major difficulty of validating HIV stigma by its connection to mental and behavioral health outcomes is the lack of validated instruments for children and adolescents in sub-Saharan Africa. 86 We could not find any research that rigorously evaluated the validity of the PHQ-9 in East Africa among children or adolescents, although the PHQ-9 was evaluated among adults living with HIV in western Kenya and showed good validity and reliability in assessing Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) depressive disorders. 87 A study in Zambia found high rates of emotional problems among adolescents living with HIV, 88 but a study evaluating the validity of the SDQ among HIV orphaned children in South Africa showed valid clinical cutoffs for caregivers but not for children. 89 Second, while both the SDQ and PHQ-9 have been translated into more than 60 languages, validation of the instruments into many languages (eg, Kiswahili) has not been investigated. 90 This validation study was tested in only one country in sub-Saharan Africa, and there may be additional language and cultural content challenges if using it in another setting. Nonetheless, the Academic Model Providing Access to Healthcare program in Kenya is clinically representative of many in sub-Saharan Africa, 91,92 and the study sites included urban, peri-urban, and rural clinical sites. Moreover, while participants had the choice to have the questionnaire administered in English or Kiswahili, almost all participants chose Kiswahili, which prevented us from comparing the validity of the questionnaire when it was administered in English versus Kiswahili. Additional work adapting and retesting this stigma instrument is ongoing. Third, enrollment in this study was done via convenience sampling. It is possible that children or their caregivers who were experiencing higher levels of HIV stigma would have been less inclined to enroll in the study, which required participation in study assessments and keeping medication in MEMS bottles. Additionally, the instrument was only tested in disclosed children, as the questionnaire directly asks about HIV. Finally, the stigma instrument was delivered by 8 research assistants (1 per clinic). To improve standardization of instrument administration, extensive training sessions and bimonthly meetings with the senior research team to discuss study assessments were conducted.
Conclusion
We provide evidence for the reliability and validity of a culturally tailored and patient-informed instrument to measure HIV-related stigma among Kenyan children and families. The stigma instrument showed good reliability and construct validity was high on child- and caregiver-reported emotional and behavioral health, with higher levels of reported HIV stigma associated with poorer mental health. While additional testing of this instrument is required, our study provides an important contribution to the limited literature on instruments to measure stigma among HIV-infected children and their families in resource-limited settings.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the view of Icahn School of Medicine at Mount Sinai, Indiana University School of Medicine, University of Massachusetts Boston, or the Moi University School of Medicine. The primary author had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Acknowledgments
First and foremost, the authors acknowledge the invaluable contribution of time from the cohort of families who participated in this study and the health-care workers involved in their routine care. The authors also acknowledge the diligent work by the study’s counselors and research assistants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant “Stigma in AIDS Family Inventory” (3R01MH099747-01S1) to Dr Rachel Vreeman from the National Institute for Mental Health, Bethesda, MD, USA.