
Abstract
The World Health Organization guidelines for treating pregnant HIV-positive women and preventing HIV transmission to infants now recommend lifelong antiretroviral treatment for pregnant and breastfeeding women. We applied quality improvement (QI) methods to support governments and facility staff to address service gaps in 5 countries under the Partnership for HIV-Free Survival (PHFS). We used 3 key strategies: break the complex problem of improving HIV-free survival into more easily implementable phases, support a national management team to oversee the project, and support facility-level staff to learn and apply QI methods to reducing mother-to-child transmission. The key results in each country were increases in data completeness and accuracy, increases in retention in care of mother–baby pairs (MBPs), increase in coverage of MBPs with appropriate services, and reduction in vertical transmission of HIV. The PHFS experience offers a model that other multicountry networks can adopt to improve service delivery and quality of care.
What Do We Already Know about This Topic?
Quality improvement (QI) has been shown to be effective in reorganizing care to improve services for HIV-positive women and their exposed infants and to reduce transmission from mother to infant.
How Does Your Research Contribute to The Field?
We applied the QI approach to address the same problems in five countries and documented what each country did to reorganize service delivery and improve clinic processes.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
The Partnership for HIV-Free Survival intervention changed practices in health facilities and contributed to changes made in national policy that were a direct result of what was shown to be effective in improving care for mothers and their infants.
Introduction
The World Health Organization (WHO) guidelines for treating pregnant HIV-positive women and preventing HIV infection in infants have evolved since 2010 to now endorse lifelong antiretroviral treatment (ART) regardless of clinical stage or CD4 count for pregnant and breastfeeding women. 1 This change required health-care providers to modify care delivery by initiating all HIV-positive pregnant women on ART; supporting treatment adherence during and after pregnancy; counseling women on breastfeeding and complementary feeding, weaning, and postweaning testing; providing prophylaxis for HIV-exposed infants (HEIs); and treating HEIs who become infected. Already overburdened, many providers struggled to effectively handle these changes, leaving significant service delivery gaps. 2
To address these challenges, the WHO, the United Nations Children’s Fund, and the US President’s Emergency Plan for AIDS Relief (PEPFAR) launched the Partnership for HIV-Free Survival (PHFS) in March 2013, supporting Kenya, Lesotho, Mozambique, South Africa, Tanzania, and Uganda. This article described the application of quality improvement (QI) methods in 5 of the 6 countries. Although the global initiative began in 2013, the various countries were on a staggered time line, according to their differing situational contexts. The PEPFAR funded 2 technical assistance teams: USAID Applying Science to Strengthen and Improve Systems Project (ASSIST) in Kenya, Lesotho, Tanzania, and Uganda, and the Institute for Healthcare Improvement (IHI) in South Africa to support governments and health facility staff in applying QI approaches to address service gaps (note 1). In every country, the Ministry of Health (MoH) took leadership of the initiative, and implementing partners provided inputs such as clinical training, supplies, and community referrals.
Problem
Without ART prophylaxis for mother–baby pairs (MBPs) and breastfeeding for 2 years or longer, mother-to-child transmission (MTCT) risk is approximately 40% for HEI. 3 Combined ART administered during pregnancy and continued while breastfeeding, along with appropriate care, can reduce MTCT to less than 5%. 4 But there are many challenges, and transmission rates remain unacceptably high in resource-limited countries. 5,6
An HIV-positive pregnant woman and her infant require multiple stages of coordinated care for their optimal health, from preconception until the infant is 2 years old. Many health systems fail to support MBPs to transfer among these different stages of care, creating multiple opportunities for a health facility to lose track of MBPs who simply do not return for care 7 or for a pair to receive only one category of services without being connected to other services they need. Retention is a problem across HIV care, but pregnant women are more likely to be lost to follow-up (LTFU) than nonpregnant adults. 8 Retention progressively decreases from predelivery into the postpartum period. 9
The PHFS promoted the use of QI methods to address many of these problems stemming from how care is organized. Quality improvement is a management science that empowers frontline health workers with skills and tools to function as a QI team to change systems and processes of care at health facility level. Quality improvement has been shown to improve PMTCT and other care processes in health facilities. 10,11
Ethical Approval and Informed Consent
No ethical approval or informed consent was required for this paper as no patient-level data were collected and used.
Methods
Kenya, Lesotho, South Africa, Tanzania, and Uganda implemented PHFS-supported work based on 3 key strategies: (1) break the complex problem of improving HIV-free survival into more easily implementable phases, (2) support a national management team to oversee the project, and (3) support facility-level staff to learn and apply QI methods to reducing MTCT. During implementation, the 4 USAID ASSIST-supported countries (Kenya, Lesotho, Tanzania, and Uganda) collaborated by sharing results and learning among the 4 countries, while the South African team supported by IHI worked independently.
Break the Complex Problem of Improving HIV-Free Survival into More Easily Implementable Phases
Given the complexity of HIV care for women and their infected newborns, we deconstructed the problem into a set of smaller problems to be tackled by teams sequentially. We believed setting more manageable goals and achieving short-term, intermediate successes would motivate QI teams. In each country, the national management team designed the intervention to first understand service flow and data availability in a few clinics that would be supported under the PHFS. They learned that many patients and their data were lost between different service areas (eg, obstetrical care and HIV care) and that facilities were not able to link the records of mothers with their infants. They found that even during clinic visits, MBPs often did not receive all elements of required care. Staff from the 4 ASSIST-supported countries met to share their findings and plan how to phase the work. During this meeting, they agreed to break improvement efforts into 3 phases: Retain MBPs in care to avoid postpartum LTFU. Provide critical services at routine visits for MBPs. Provide critical services at special visits for MBPs.
The South African team began by sensitizing demonstration districts and province staff on the PHFS and conducting 12-month retrospective baseline assessments of services provided to HIV-positive mothers and their exposed infant in the 54 demonstration sites to identify gaps in PMTCT service delivery. They arrived at similar conclusions. After developing this phased approach, technical assistance teams worked with national management teams to develop implementation plans.
Keeping MBPs in care to avoid postpartum LTFU
One of the first implementation challenges to overcome for keeping MBPs in care was measurement. Teams needed to measure the number of MBPs retained in care (numerator) using the denominator of the total number of MBPs who should be attending the clinic every month. But there is no global standard for this indicator, given different country guidelines and data systems. All PHFS countries measured the numerator in the same way; the problem was how to calculate the number of MBPs who should be retained in care. We settled on 2 options for measuring this denominator with different strengths and weaknesses (Table 1). Each country team selected the option that worked best for them.
Retention Denominator Options, Strengths, and Weaknesses.

Abbreviations: ART, antiretroviral treatment; HEI, HIV-exposed infant; NA, not available.
A key challenge in understanding the problem’s scope was determining accurate measures for the number of MBPs who should be in care versus those actually in care. Each country team field-tested their selected indicator at one site before collecting baseline data for all sites. In Uganda, the baseline measure at 22 demonstration sites was 2.2% in care, translating to over 97% of HEI unaccounted for. Baseline was 0% to 18% in care at 30 Tanzania sites, 0.8% in care at 16 sites in Kenya, and 1% in care at 12 Lesotho sites.
Infants born at each site up to 18 months prior (24 months in Lesotho) were counted to create an estimated denominator. For example, to determine the total number of HEIs younger than 18 months expected to be in care monthly, Uganda used their early infant diagnosis register to identify all HEIs registered up to 18 months prior to the month of interest, then removed all infants who had died, been discharged, or transferred out of the facility, leaving only active HEIs and those LTFU. Monthly, sites adjusted the denominator by adding newly enrolled HEIs and transfers-in and deducting the dead, discharges, and transfers-out.
Providing critical services at routine and special visits
Retaining MBPs in care is necessary but not sufficient to improve HIV-free survival. When MBPs come to a health facility, they also need to receive the appropriate services. One of the challenges in providing care to MBPs is that the appropriate services change depending on the age of the child. This makes it confusing for health workers to remember what to provide on that specific visit. To address this problem, we divided elements of care into routine care—those elements of care that were required for any interaction with MBPs—and special care—those elements of care that would vary depending on the child’s age or the mother’s clinical status (Table 2). Countries measured routine care service provision differently. Lesotho and Uganda used a composite indicator; Kenya and Tanzania measured and tracked each service separately. The composite indicator numerator consisted of 7 items in Uganda listed in Table 2 under critical services; Lesotho tracked an eighth item, immunization. If all services on the list were provided, the MBP was counted in the numerator.
Routine and Special Visits.
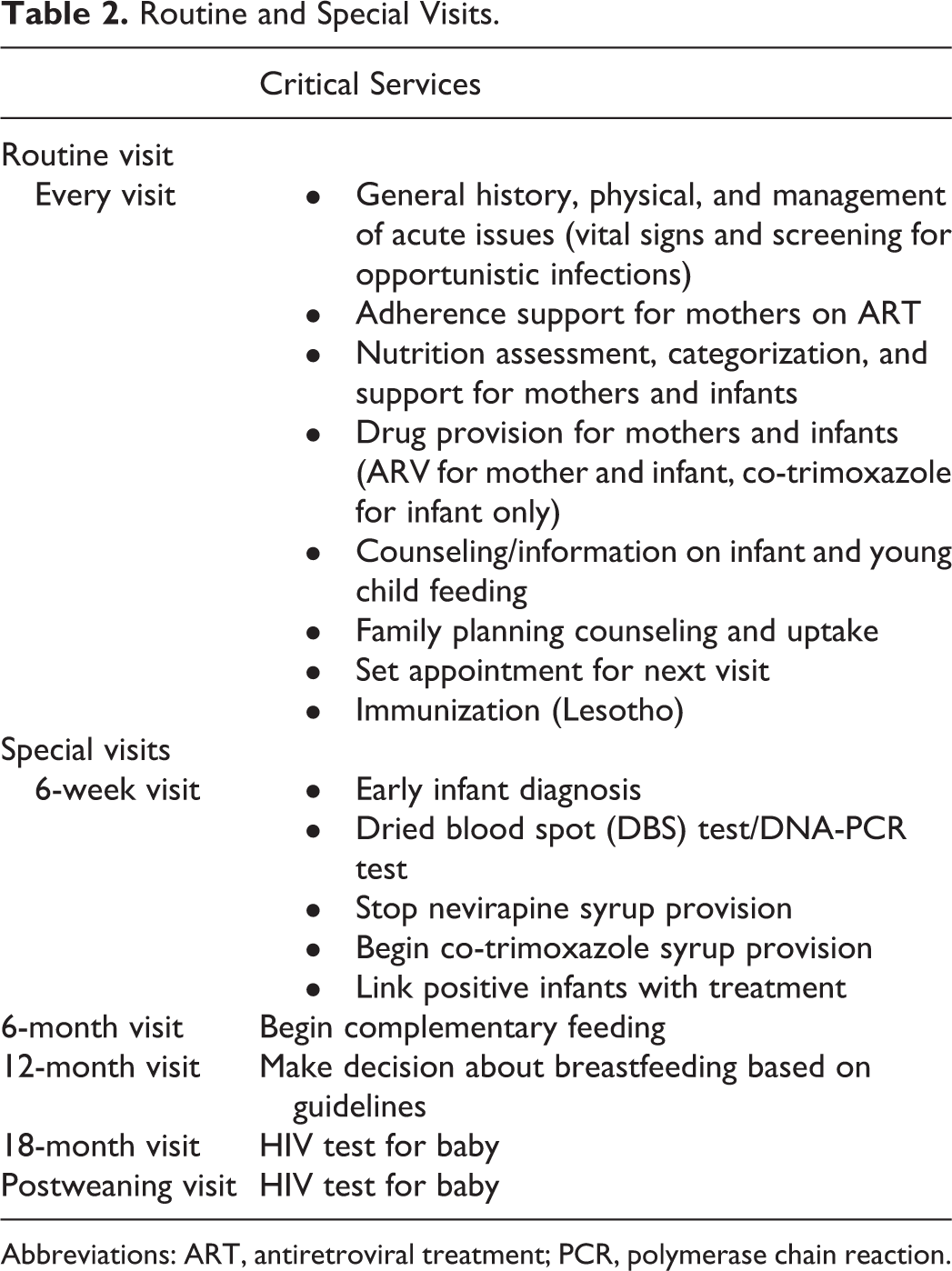
Abbreviations: ART, antiretroviral treatment; PCR, polymerase chain reaction.
After addressing retention, QI teams within facilities focused on improving care during routine visits and then moved on to improving special visits. The idea behind this phased approach was to avoid overwhelming QI teams with too many improvements areas at once.
Supporting a National Management Team to Oversee the Project
For the second element of the PHFS strategy, each country established a PHFS steering group and/or used their existing national PMTCT working group to (1) designate demonstration sites for piloting this approach, (2) identify improvement priorities and measures, (3) coordinate the roles and responsibilities of each partner, and (4) plan and oversee implementation. Groups convened monthly and were chaired by an MoH PMTCT lead and, in some countries, co-chaired by the nutrition lead. The initial step was to identify demonstration sites (Table 3) and to plan how to use the learning from these sites to develop a strategy to scale up the approach nationally if it was found to be effective.
PHFS Demonstration Sites by Country and Facility Type.
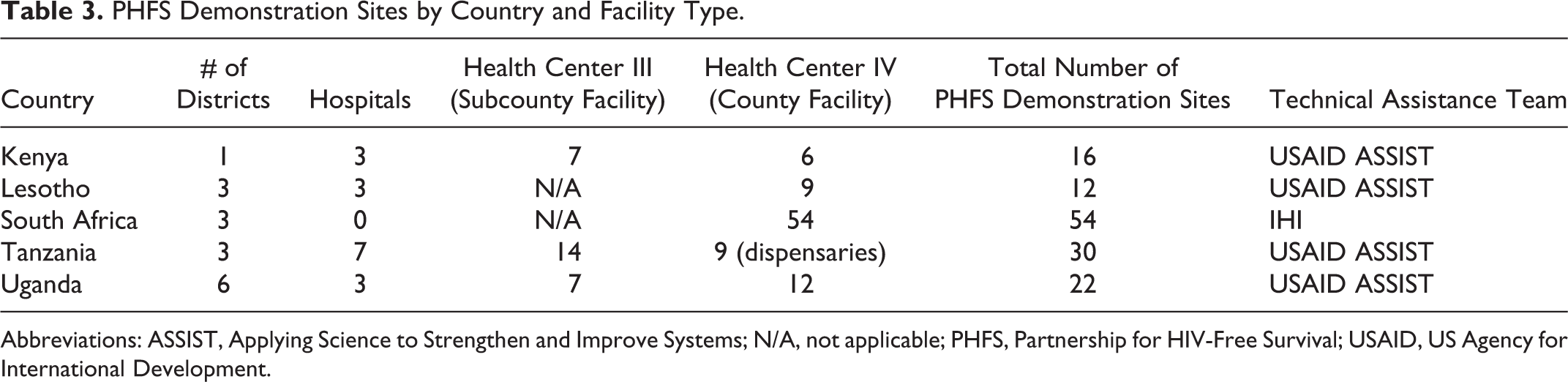
Abbreviations: ASSIST, Applying Science to Strengthen and Improve Systems; N/A, not applicable; PHFS, Partnership for HIV-Free Survival; USAID, US Agency for International Development.
Support Facility-Level Staff to Learn and Apply QI Methods
The heart of the PHFS work was changing how care was delivered at facilities. We used 3 approaches to support facility staff to use QI methods to improve care for HIV-positive mothers and their babies: initial training in QI methods, on-site QI coaching, and peer-to-peer learning.
Initial training
Two- or 3-day QI trainings 12,13 were conducted by advisors with at least 5 years’ experience applying QI methods to different clinical areas, except for Lesotho staff who were newer to the QI approach. Topics included how to form QI teams at the facility, developing improvement aims (clear and quantifiable objectives), analyzing clinic processes to identify gaps, choosing changes and testing them using the Plan-Do Study-Act (PDSA) cycle, and analyzing data to determine whether a change resulted in improvement to a predetermined process indicator. During the QI training, advisors introduced health workers to tools that guided teams through implementation. Teams in Kenya, Lesotho, Tanzania, and Uganda used QI documentation journals, 14 while teams in South Africa used QI trackers, hardcover books, and PDSA templates. 15 Teams used these tools to document progress, record data, and plot time series charts; these tools were reviewed during coaching visits. Country teams’ application of QI was guided by the Model for Improvement. 16
Coaching
The teams received regular coaching led by MoH district health officers competent in QI, as well as advisors from the technical assistance teams. The MoH officers attended the initial QI training and received ongoing guidance from QI advisors where needed, essentially a “coaching for coaches.” Coaches supported the facility staff to learn how to work effectively as a QI team, identify the root causes of barriers to improving care, develop possible solutions for those barriers, use iterative testing to identify which solutions work and modify them to work optimally in that context, and continually measure and use data as feedback on whether care was improving.
In Kenya, Uganda, and South Africa, sites received monthly coaching. Due to the distances between the 3 Tanzanian districts (Mufindi, Nzega, and Mbeya), sites received quarterly coaching. Visits in Lesotho occurred every quarter from March 2014, then monthly beginning in August 2016. Coaches in Kenya, Lesotho, Tanzania, and Uganda used a coaches’ guide, 17 and in South Africa, an improvement tracker, 18 to organize their visits by documenting improvement aims, change ideas that were being currently tested, results from previous coaching visits, and areas to discuss during the next visit. Coaches also collected data from facilities on paper before transferring them to Excel databases for aggregation and analysis.
Peer-to-peer learning
The QI collaborative model (Figure 1), developed by IHI, was applied in each country. This is a method for testing and implementing evidence-based changes quickly across a group of facilities.

The Institute for Healthcare Improvement quality improvement collaborative model.
Two to 3 individuals from each demonstration site were convened for 2-day district-level learning sessions every quarter. The technical assistance team led the development of learning session agendas, created graphs depicting site performance, identified roles for district management coaches and implementing partners at the sessions, and prepared materials (flip charts, markers, notebooks, etc). Learning sessions begin with presentations of site-level performance data, which often ignited friendly competition among teams. These gatherings also often included small group discussions to identify good practices, technical or QI method refresher training, and development of action plans by each team. After each session, participants shared what they learned with their colleagues. Team members rotated their attendance at the next session so that most, if not all QI team members, participated in at least 1 learning session. The PHFS learning session participation ranged from 25 to 50 people, depending on the number of demonstration sites in the district.
Results
The key results of PHFS activities in each country were increases in data completeness and accuracy, increases in retention in care of MBPs, increase in coverage of MBPs with appropriate services, and reduction in vertical transmission of HIV. This article presents the first 2 types of results; service coverage and MTCT results are presented in other articles in this supplement.
Improving Data Completeness and Accuracy
In Kenya and Tanzania, data quality audits were conducted during coaching visits, and data cleaning exercises were undertaken to address gaps. In South Africa, teams conducted file audits and cross-checked tally sheets, facility input forms, registers, and DHIS data monthly to ensure accuracy and to identify and address inconsistencies in the data.
In Uganda, data accuracy and completion was a QI aim. At baseline in Uganda, only 2.9% of HEI clinical charts were found to be complete and accurate. Quality improvement teams improved the completeness and accuracy of records to over 90% within 9 months and maintained that level of performance for the subsequent 9 months before they ceased regularly tracking this indicator (Figure 2).

Improving data completeness and accuracy in Uganda.
The Ugandan teams first discussed how they would measure improvement in data completeness and accuracy. They agreed to tally the number of records with complete and accurate data and the total number of records at the end of each day, determining accuracy by cross-checking patient records against registers. A QI team member was assigned to perform this task, and teams met briefly each day to review the results. After a root cause analysis, they learned that many health workers were unclear about how to complete the registers and records and required refresher training or orientation on proper documentation of services. Training only resulted in slight improvements since the problem was both due to lack of understanding how to document and failure to do it. The QI teams agreed that clinical records needed to be completed before patients left the clinic, and they assigned a nurse with the task of checking each record.
Keeping MBPs in Care to Avoid Postpartum LTFU
Providers worked to reorganize and integrate care delivery by merging service points for MBPs, which ensured they could link the files of mothers and their babies and give pairs a joint appointment date. Improving retention also included ensuring that MBPs accessing other services at the facility (like for fever) were identified and given HIV/MNCH appointments. Several tools and job aids were created and used to track pairs.
The proportion of MBPs retained in care every month was extremely low at baseline, but the 4 country teams (Figure 3) were able to significantly improve retention by the end of their respective intervention periods. This supplement includes individual country papers describing the QI work in Kenya, Lesotho, Tanzania, and Uganda, respectively; those papers provide in-depth process results using time series charts. Uganda collected data from 3 non-PHFS sites for comparison; those sites did not register any change in the processes that were being improved at demonstration sites.

Improving retention of mother–baby pairs in 4 countries.
The South African technical assistance team faced challenges combining MBP files. Joint appointments were given, but files ultimately remained separate. The team identified HIV-positive pregnant women at antenatal care and used postnatal care (PNC) registers to identify HEIs. Pairs were documented in another book. This exercise proved helpful; HEIs were easily identified at the 6-week PNC visit and received care. However, follow-up visits were challenging because up to 60% of mothers resumed working and their HEIs were brought to facilities by guardians. Despite numerous appointment reminders, most mothers did not return. For PHFS, South African teams only counted mothers and babies who received care as pairs in their numerator and total number of MBPs in their denominator. Results from South Africa were not provided for this manuscript.
Providing Critical Services at Routine and Special Visits
All countries improved services at routine and special visits, including nutrition services and HIV testing for HEIs at various stages. Detailed results are available in the country-specific papers within this supplement.
Countries inserted checklists into medical records and posted them on examination room walls to ensure that MBPs received all required services when they came for care.
Specifying Changes to Service Delivery That Were Tested and Found Effective
In addition to the quantitative results, PHFS activities in the 5 countries generated important learning about how to improve PMTCT in these settings. Tables 4 to 7 list the changes tested and adopted in the 4 main areas that QI teams focused on: data completeness and accuracy, retention of MBPs, increasing coverage of routine services, and increasing coverage of special services. (The article titled “Using a multi-country learning network to harvest and rapidly spread implementation knowledge across programs aimed to reduce mother-to-child transmission of HIV and improve nutrition: perspectives and lessons learned for similar large-scale initiatives” in this supplement describes how this learning was generated.)
List of Changes Tested and Adopted to Improve data Completeness and Accuracy.

Abbreviation: MBP, mother–baby pair.
List of Changes Tested and Found Effective to Increase Retention of MBPs.

Abbreviation: MBP, mother–baby pair.
List of Changes Tested and Adopted to Increase Coverage of Routine Services.
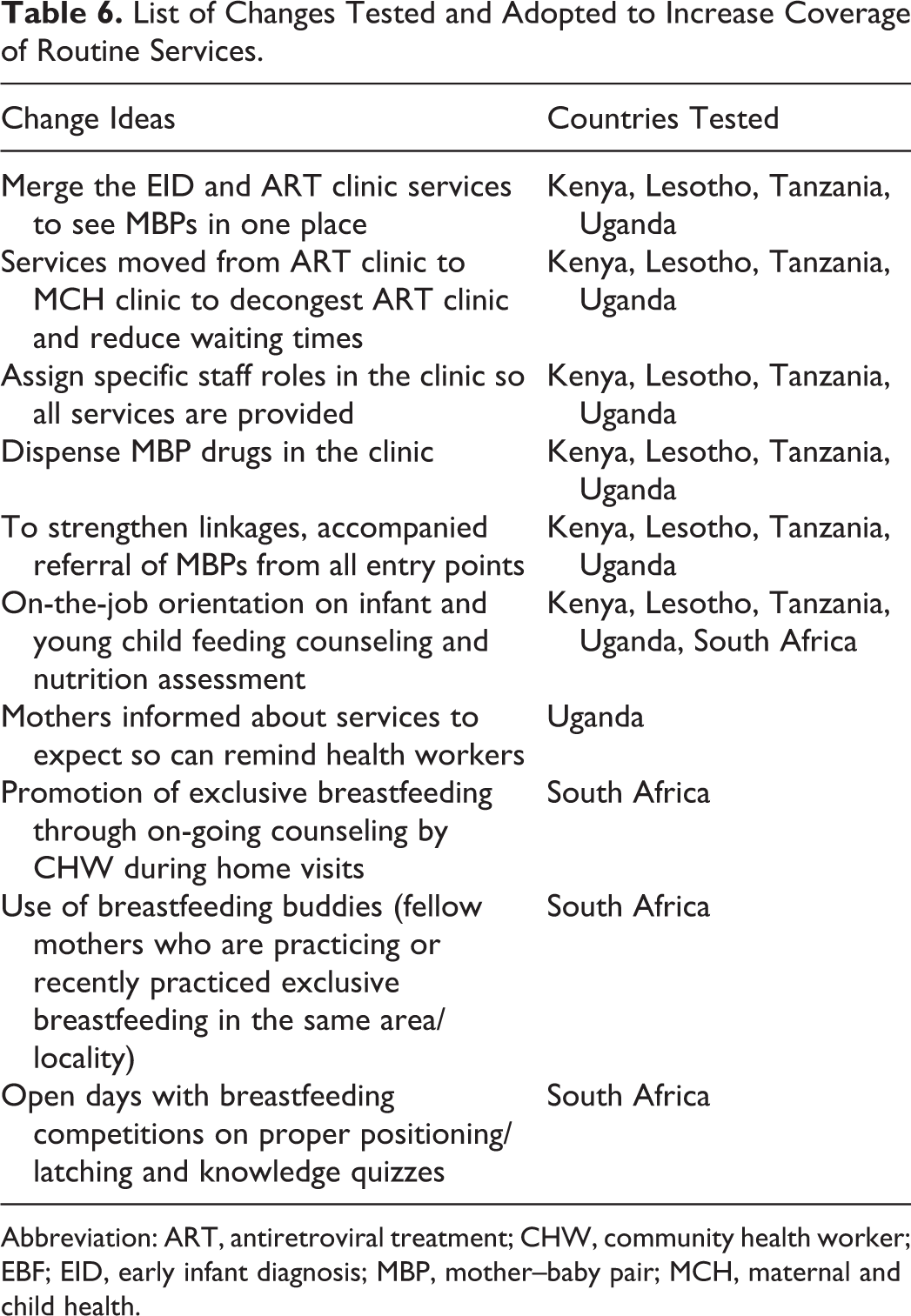
Abbreviation: ART, antiretroviral treatment; CHW, community health worker; EBF; EID, early infant diagnosis; MBP, mother–baby pair; MCH, maternal and child health.
List of Changes Tested and Adopted to Increase Coverage of Special Services.

Abbreviation: ART, antiretroviral treatment; CHW, community health worker; EID, early infant diagnosis; HEI, HIV-exposed infant; MBP, mother–baby pair; PCR, polymerase chain reaction.
The country papers included in this supplement (Kenya, Lesotho, Tanzania, and Uganda) describe in detail the changes they tested. Each country and even each facility team discussed how best to improve processes and decided on which changes to test at a microlevel. For that reason, not every country tested every change, because a given change may not be relevant in certain health-care settings. In fact, only a handful of changes that resulted in improvement were tested in every country. A change idea may not have been relevant because it was addressing an issue that was not a problem in that particular context, or because it was not a good solution for that particular country/facility. Each country’s experiences with the various changes tested were shared through biweekly calls and multicountry learning network channels.
Discussion
Retaining MBPs in care to reduce vertical transmission requires making the service delivery system easier for patients to remain in care and reliably providing the right care to patients at each visit. Both present challenges to a health-care system. First, health-care service delivery is typically an individual activity (eg, the nurse is responsible for one set of tasks, while the doctor has another set). Retention does not fit this paradigm—no one individual is responsible for ensuring people stay in care. Second, relying on individuals’ memory about which services should be provided at each visit is fraught with the possibility of error. Quality improvement is a collective management approach that can give health workers better skills and tools for fixing problems like retention—areas that are not easily assignable to any one person—and for changing service delivery, making it less dependent on individual initiative or memory.
Breaking addressing problems down into 3 stages, a focus on country ownership, and a collaborative country-level steering group allowed countries and QI teams to quickly get started.
From the very first meeting, we agreed to a deliberate focus on learning and documenting what health workers were learning in real time. The ASSIST technical support teams in particular held biweekly phone learning meetings to discuss progress, successes, and challenges. Throughout the 3-year implementation period, this deliberate focus reminded us to continuously analyze, document, and share what we were learning about improving care within each country and across countries, using various formats from one-on-one to multicountry sharing.
There were several challenges in implementation. The international partners charged with facilitating the PHFS in the various countries needed to understand how to work under the leadership of the MoH to integrate this work into existing national PMTCT strategies. If the PHFS was perceived as a new or parallel intervention, the MoH was rightfully reluctant to engage or assume ownership.
In some cases, we struggled to engage all critical MoH departments (HIV, MNCH, and nutrition) from the start. It was also challenging for us to keep the focus on learning. Several steering committees were in favor of implementing the PHFS in many sites straightaway, and we held dialogues to convince the countries to keep the total number of demonstration sites small in order to facilitate learning, documentation, and validation of effective strategies for eventual spread.
Country Variation in QI Application
Quality improvement applications are contextual; health-care workers learn to constantly modify and adapt when using QI approaches. Countries agreed on priorities, but their implementation approach varied. Teams varied in how they measured MBP retention as described above and in the provision of their routine visit services. For example, Lesotho and Uganda tracked the delivery of their respective standard care package of services using a composite indicator. Kenya, South Africa, and Tanzania tracked provision of individual routine services rather than a standard package, such as ART initiation for mothers or nutrition assessment and categorization.
Teams tested change ideas according to country contexts, but we found parallels. For example, Kenya used mentor mothers to track mothers who missed appointments; Tanzania used community health workers and home-based care providers; while Uganda used expert patients, linkage facilitators, mentor mothers, or community health workers.
The nuances of coaching and peer-to-peer learning also varied. South Africa, Tanzania, and Uganda had learning sessions quarterly; Kenya had yearly sessions; and Lesotho convened 3 over an 18-month period. South Africa faced challenges as monthly coaching visit dates were preplanned; teams were not able to adapt if the subdistrict had another priority that week. This meant missed opportunities for MoH program coordinators to be part of some site visits.
The various country/facility management teams had divergent abilities and preferences, which led to divergent approaches in the application of QI and the variation in the strength of the results.
Across the 5 countries, PHFS supported 134 facilities to use QI approaches to improve PMTCT, MCH, and nutrition care for MBPs. We believe the PHFS experience offers a model that other multicountry networks can adopt and build on to improve service delivery and quality of care. The key elements of success were: (1) breaking down problems into smaller, more specific problems; (2) addressing those problems with data-driven QI led by individual facility teams; (3) multistakeholder, in-country leadership; (4) on-site QI coaching; and (5) inter- and intracountry shared learning and support. Particular challenges were related to shifting the focus away from excessive planning and data collection at the early stages and keeping the focus on getting started quickly and learning from the QI processes that each facility was applying to its clinical flow. The application of QI in this context led to greater efficiencies and effectiveness in service delivery.
Footnotes
Acknowledgments
This initiative was the brainchild of WHO, IHI, UNICEF, and USAID. It was led by the Ministries of Heath, driven by national and district health teams, and operationalized by health facility staff and community workers/volunteers. The authors would like to acknowledge Timothy Quick for his critical contributions to this initiative and his continued support, encouragement, and guidance. The authors also thank Lani Marquez for her technical support and her key knowledge management role for this initiative including editing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the US President’s Emergency Plan for AIDS Relief (PEPFAR) through the US Agency for International Development (USAID) and its Applying Science to Strengthen and Improve Systems (ASSIST) Project, implemented by University Research Co, LLC (URC) through Cooperative Agreement Number AID-OAA-A-12-00101.