
Abstract
Over half of mother-to-child HIV transmission (MTCT) occurs postdelivery. Keeping mother–infant pairs in care remains challenging. Health workers in 3 countries used quality improvement (QI) approaches to improve data systems, mother–infant retention, and facility-based care delivery. The number and proportion of infants with known HIV status at time of discharge from early infant diagnosis programs increased in Tanzania and Uganda. We analyzed data using statistical process control charts. Mother-to-child HIV transmission did not decrease in 15 Kenyan sites, decreased from 12.7% to 3.8% in 28 Tanzanian sites, and decreased from 17.2% to 1.5% in 10 Ugandan sites with baseline data. This improvement is likely due to the combination of option B+, service delivery improvements, and retention through QI approaches. Reaching the global MTCT elimination target and maximizing infant survival will require health systems to support mother–infant pairs to remain in care and support health workers to deliver care. Quality improvement approaches can support these changes.
Background
United Nations Programme on HIV/AIDS estimates that postbreastfeeding mother-to-child HIV transmission (MTCT) rates in 21 Global Plan countries have decreased from 22% in 2009 to 8.9% in 2015. More than half of the remaining infections now occur after delivery. 1 Reducing transmission rates further will require improvements in the care for mothers and infants during the postpartum period. To date, keeping mothers and infants in care after delivery has proven challenging. A recent review of lost to follow-up among HIV-exposed infants (HEIs) found that 34% of exposed infants were lost by 3 months and that 45% who had early infant diagnostic testing at 3 months were subsequently lost after testing. 2 Retention in care is a challenge in all HIV treatment programs, but pregnant 3 -6 and postpartum 7,8 women have worse retention in care than men or nonpregnant women. In addition, some 7 -11 but not all 12,13 studies find that retention is worse after delivery than before. Retention in care is a powerful predictor of HIV transmission. 11 It is also important for meeting the other health needs of HEI and their mothers, both of whom have higher mortality risks than their unexposed and uninfected counterparts. 14
What Do We Already Know about This Topic?
Over 50% of mother to child HIV transmission occurs after delivery. Retaining mothers and their exposed infants in care is important for reducing transmission but retention is generally poor.
How Does Your Research Contribute to the Field?
Health workers in Kenya, Tanzania and Uganda were supported to use quality improvement (QI) approaches to improve facility data systems, support mothers and babies to remain in care and ensure delivery of evidence based care. HIV transmission decreased substantially in Tanzania and Uganda but not Kenya. This is likely due to a combination of the availability of option B+ and improved retention in care and service delivery through QI approaches.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
Health workers can use QI approaches to reduce HIV transmission after delivery. Health systems should consider how to integrate these approaches into existing systems.
To address the challenges of retention and poor patient care in the postpartum period, the Partnership for HIV-Free Survival (PHFS) supported health facilities in Kenya, Lesotho, Mozambique, South Africa, Tanzania, and Uganda to use quality improvement (QI) approaches to identify and implement changes in how they delivered care. The goal was to reduce postnatal HIV transmission and mortality by helping staff in supported facilities to improve patient retention, HIV treatment and prophylaxis, and health and nutrition care for the mother–infant pairs attending their clinic. Staff in supported health facilities were encouraged to use QI approaches to (1) improve the data system so that health workers have complete patient information as mother–infant pairs moved among maternal, pediatric, HIV, health, and nutrition services; (2) improve mother–infant pair retention; and (3) ensure that mother–infant pairs receive appropriate care at clinic visits.
This article describes the postweaning HIV prevalence in facilities supported by the PHFS initiative in Kenya, Tanzania, and Uganda. These were the 3 countries that were able to make outcome data from their PHFS demonstration sites available at the time of data analysis and writing.
Methods
The United States Agency for International Development Applying Science to Strengthen and Improve Systems Project, working with President’s Emergency Plan for AIDS Relief clinical service partners, supported governments to implement the PHFS program in Kenya, Lesotho, Tanzania, and Uganda (the other countries were supported by other organizations). The program focused on supporting a limited number of facilities in each country to use QI approaches to improve data systems, help mother–infant pairs remain in care, and ensure that correct care was provided at clinic visits. Facilities were chosen by the national government of that country and the in-country partners based on various criteria including volume of patients and geographical HIV prevalence. The number of facilities supported per country was Kenya (16), Tanzania (30), and Uganda (22).
Detailed information on the support provided to the QI teams, and the changes that they made to deliver better care are provided in the JIAPAC-18-08-SA-1100 paper in this supplement, 15 and data on processes of care are described in the country papers (JIAPAC-18-08-SA-1103, 1104, and 1105). In summary, the type of support provided varied among countries, but in general, it consisted of (1) initial training on new prevention of MTCT (PMTCT) guidelines and the basic concepts of QI (5-day classroom training in Kenya and Tanzania, 1-day on-site training in Uganda) and (2) on-site support from trained QI coaches to help teams apply the QI skills they learned in the classroom to their setting. This involved helping them to work as multidisciplinary teams, pick specific improvement aims, to use simple analytical tools to identify causes for poor care, and to use iterative methods to test and adapt solutions to improve care. The frequency of on-site support varied from monthly (Kenya and Uganda) to quarterly (Tanzania), and (3) facilitated peer-to-peer learning sessions that allowed teams from different facilities to share progress and learn from each other. Learning sessions were 2 or 3 days in length and were held quarterly (Tanzania and Uganda) or annually (Kenya; see Table 1).
Description of PHFS Support.

Abbreviations: EID, early infant diagnosis; HEI, HIV-exposed infant; PHFS, Partnership for HIV-Free Survival; QI, quality improvement; PCR, polymerase chain reaction.
Each country’s data system was unique so each country used different methods to measure the proportion of HEI contracting HIV by the end of breastfeeding. Both Kenya and Tanzania used cohort approaches to measure transmission. All infants born to women with known HIV serostatus were admitted into the cohorts. Kenya tracked the outcomes of HEI born 24 months previously, while Tanzania tracked infants until 18 months of age. Uganda did not have a cohort system in place, and thus measured the proportion of HEI who were HIV positive when they were discharged from the early infant diagnosis (EID) system between 0 and 18 months. Data for the project were collected by facility-level staff from existing government monthly reporting registers and double-checked by the QI coaches. Data for Tanzania were collected again due to data quality concerns. Data were entered in Microsoft Excel and stored at the country level.
Because different countries used different measures and carried out the work over different time periods, data from each county were analyzed separately. Data on HIV transmission were analyzed using p-control charts that are used to analyze data with a binomial distribution 16 (eg, infants are either infected with HIV or not). We used an established rule for analyzing the control charts: a series of 8 consecutive points below the center line is categorized as a shift in the prevalence of HIV and will occur less than 0.4% of the time. 17 -19 Monthly data were used to create a time series graph. We then calculated the initial center line by calculating the mean of the monthly HIV transmission rate before the start of the QI intervention in Kenya and Tanzania. In Uganda, we only had data for 4 months prior to the start of the QI intervention, so we used the first 6 months (ie, we included the first 2 months of the QI intervention to set the initial mean). In all countries, if we detected a shift, we calculated the subsequent mean using the 8 data points that constituted the shift.
Ethical Approval and Informed Consent
Data for this project came from hospital records that are routinely collected and aggregated and contained no patient-level data or identifiers. No ethical clearance was required.
Results
Kenya
One facility enrolled no HEI; data from the remaining 15 facilities were analyzed. Between January and August 2013 (ie, before the initial QI training in September), the Kenya sites enrolled 228 HEI (mean: 28.5 per month). Of these, 15 (6.6%) were transferred to other facilities, 41 (18.0%) were lost, 6 (2.6%) died, and 157 (68.8%) had known HIV status at 24 months of age. Of this, 25 (15.9%) of the children tested were HIV positive. During the QI intervention (October 2013-September 2014), the sites enrolled 488 HEI (mean: 40.7 per month). Of these, 45 (9.2%) were transferred to other facilities, 90 (18.4%) were lost, 14 (2.9%) died, and 315 (64.5%) had known HIV status at 24 months of age. Twenty-three (7.3%) of those with known status were HIV positive (Table 2).
Number of HEI Enrolled in Care, Transferred Out, Lost, Died, and With Known HIV Status at Time of Discharge in Kenyan and Tanzanian Facilities.
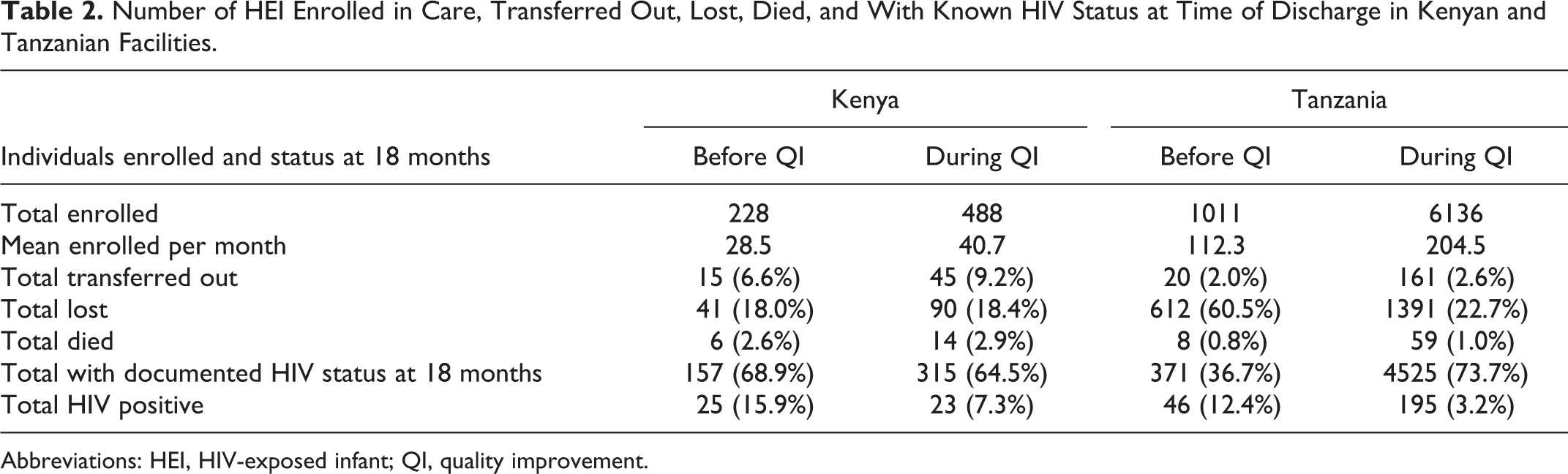
Abbreviations: HEI, HIV-exposed infant; QI, quality improvement.
On the control chart, the mean of the proportion of children with a known HIV status at discharge who were HIV positive each month during the first 24 months was 14.2%. No shift below this mean was detected (Figure 1).
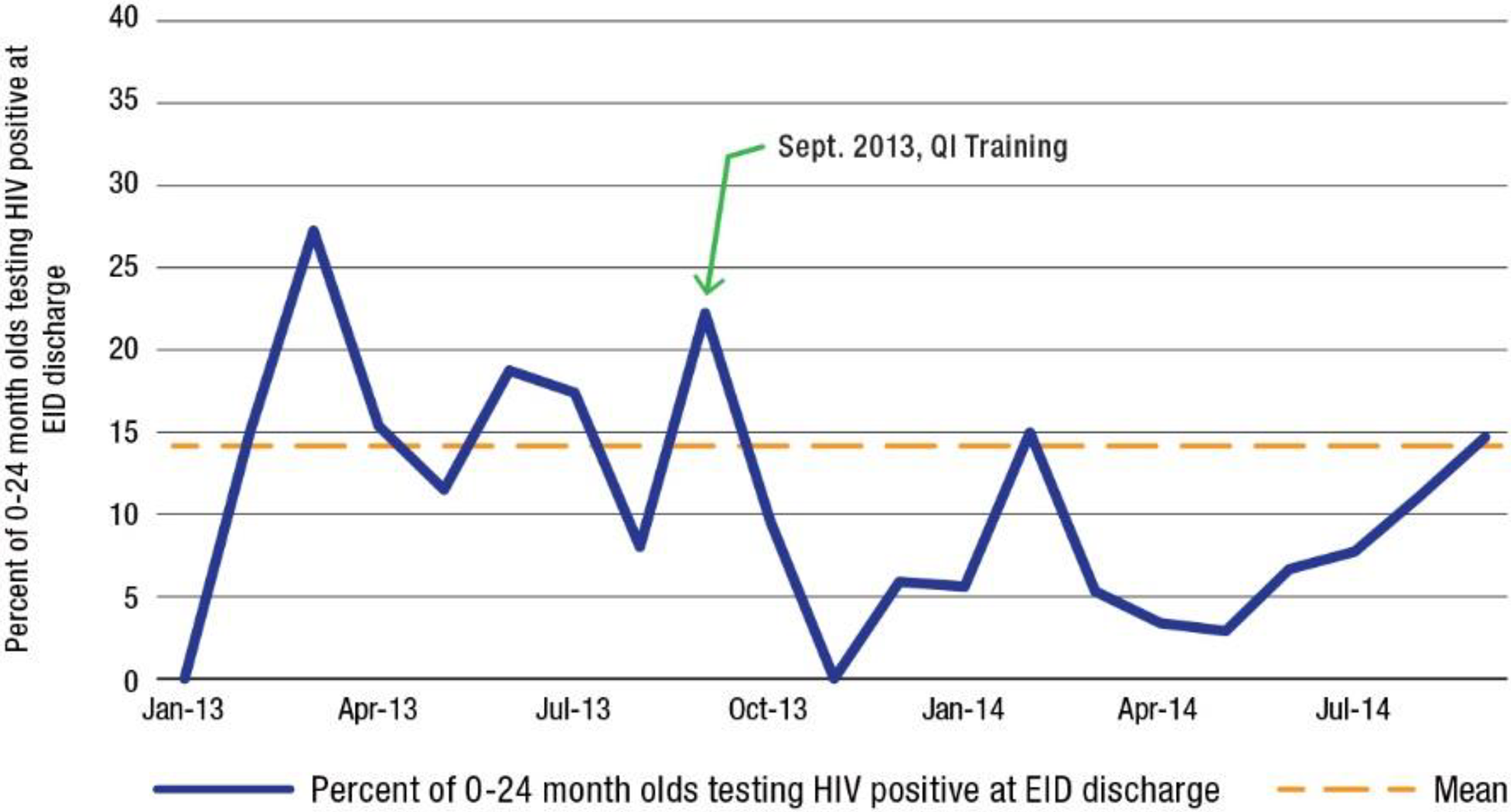
Percent of 0- to 24-month olds testing HIV positive at early infant diagnosis (EID) discharge, Kenya.
Tanzania
Data were available from 28 of the 30 sites. One facility enrolled no HEI; one facility’s data had could not be validated and were therefore excluded. Between January and September 2013 (ie, before the initial QI training in October), the facilities enrolled 1011 HEI (mean: 112.3 per month). Of these, 20 (2%) were transferred to another facility, 612 (60.5%) were lost, 8 (0.8%) died, and 371 (36.7%) had a known HIV status at 18 months. Forty-six (12.4%) of those with known status were HIV positive. During the QI intervention (November 2013-May 2016), 6136 HEI were enrolled (mean: 204.5 per month). Of these, 161 (2.6%) were transferred to other facilities, 1391 (22.7%) were lost, 59 (1.0%) died, and 4525 (73.7%) had a known HIV status at 18 months. One hundred ninety-five (3.2%) of those with known status were HIV positive (Table 2).
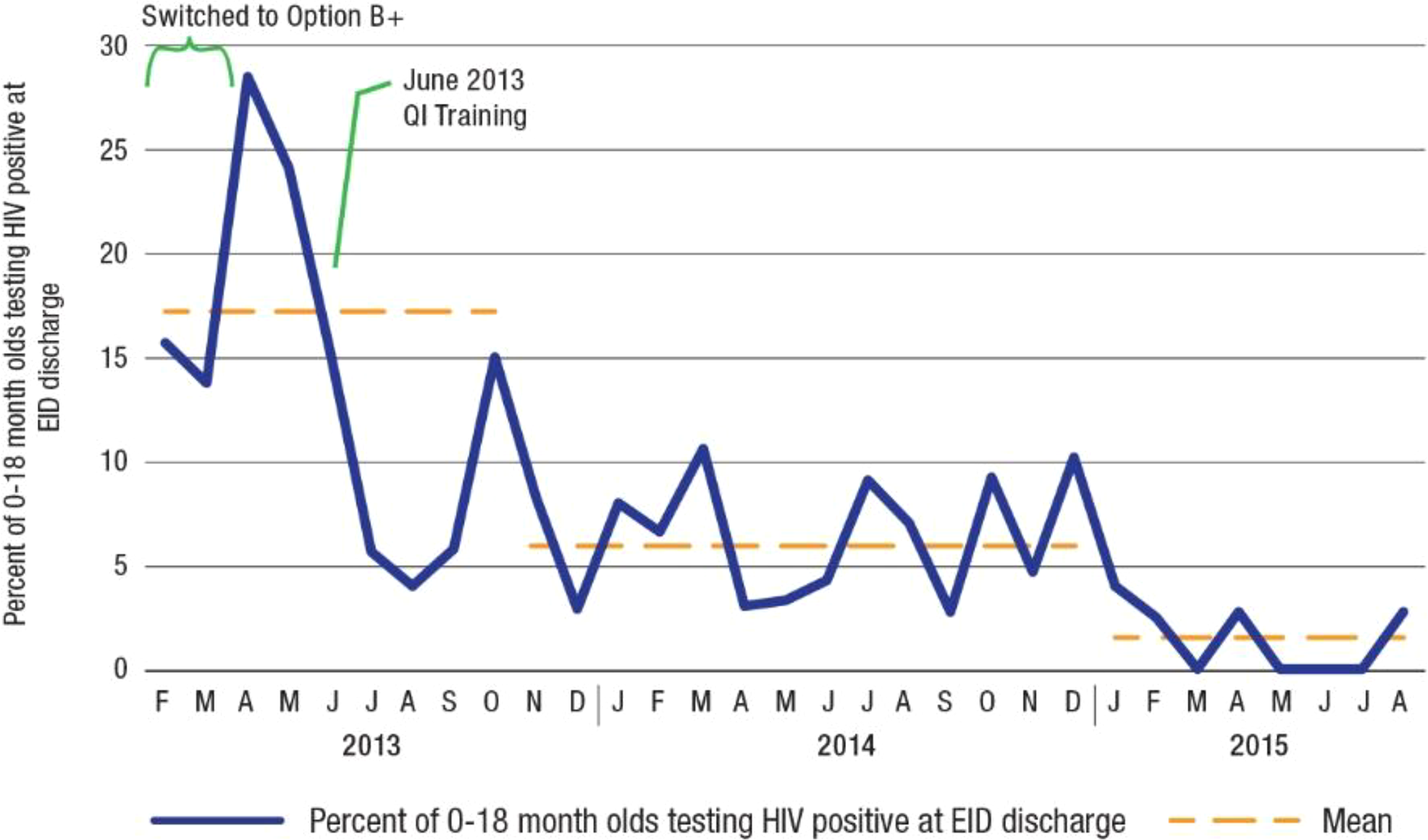
On the control chart, the mean of the proportion of children with a known HIV status at discharge who were HIV positive each month during the first 8 months was 12.7%. A shift below the mean started in August 2013, which was 2 months before the start of the QI intervention and 5 to 7 months after the switch to option B+. The new mean after the shift was 6.3% (Figure 2). A subsequent shift occurred in September 2014, which was 12 months after the QI training and 17 to 19 months after the switch to option B+. The new mean was 3.8%.

Percent of 0- to 18-month olds testing HIV positive at early infant diagnosis (EID) discharge, Tanzania.
Uganda
Data on the number of children discharged from the EID program with a known HIV status and the number who were HIV positive were not being collected at 12 of the 22 facilities at the start of the QI intervention. One of the first tasks of the QI teams was to develop these systems. All facilities had these data by December 2013. Because of the lack of data prior to QI teams starting in these facilities, we analyzed the data from Uganda in 2 separate groups: those 10 facilities that had data prior to the QI training and the 12 facilities that did not have data prior to the QI training.
Among the 10 facilities that did have data available between February and June 2013 (the initial QI training started in June 2013), an average of 29 children were discharged each month from the EID with a known HIV status (note: because Uganda did not have cohort data, we do not know how many were lost prior to that point). Of this, 17.2% of these children were HIV positive. During the QI intervention (July 2013-August 2015), an average of 39 children were discharged from the EID with a known HIV status. On the control chart, a first shift below the center line started in November 2013 (5 months after initiation of the QI intervention and 8-10 months after the switch to option B+). This shift had a new mean of 5.9%. A second shift occurred in August 2014 (16 months after the initiation of the QI intervention and 19-21 months after the switch to option B+). This shift had a new mean of 1.5% (Figure 3).
Percent of 0- to 18-month olds testing HIV positive at early infant diagnosis (EID) discharge, Uganda (10 facilities).
In the 12 Ugandan facilities without data prior to the QI training, complete data were available from December 2013. We therefore constructed a control chart from this point on. We calculated the initial mean using the first 8 months of the program. During the first 8 months (December 2013 and August 2014), an average of 32 children were discharged from the EID with a known HIV status. Of this, 9.9% of these children were HIV positive. Between September 2014 and August 2015, an average of 41 children were discharged from the EID with a known HIV status. On the control chart, a shift below the center line started in September 2014 (17 months after initiation of the QI intervention and 20-22 months after the switch to option B+). This shift had a new mean of 2.1% (Figure 4).
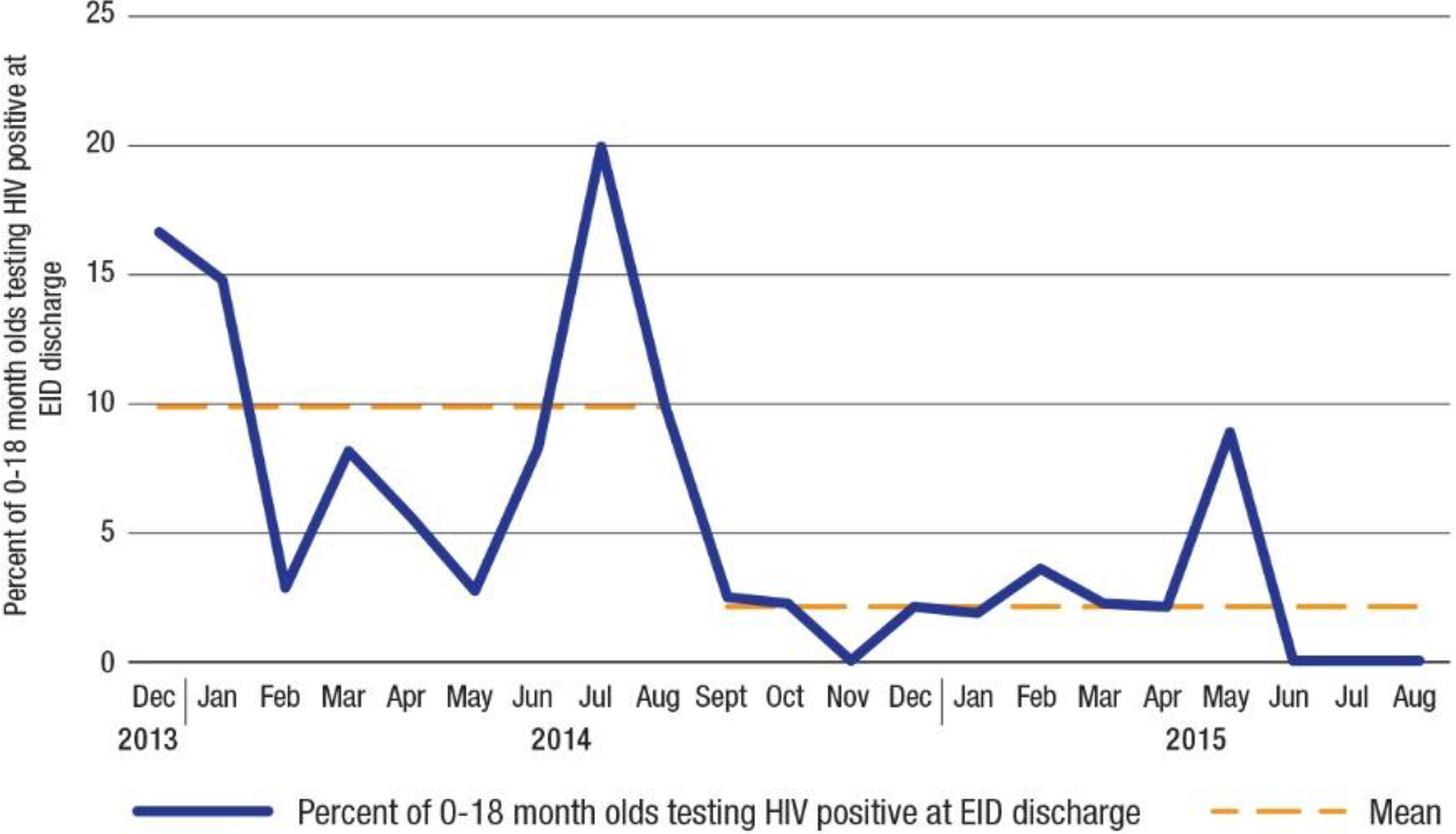
Percent of 0- to 18-month olds testing HIV positive at early infant diagnosis (EID) discharge, Uganda (12 facilities).
Discussion
Staff in facilities at Tanzania and Uganda successfully reduced HIV transmission during the time that they used QI approaches to help mother–infant pairs remain in care and to ensure that appropriate services were delivered during clinic visits. The baseline levels of transmission were very high in these facilities and were not much lower than transmission rates that occur in the absence of antiretroviral therapy. 20 Teams in all countries were able to successfully use QI approaches to improve retention in care of mother–infant pairs and improve processes of care during clinic visits. 15 The number of HEI retained in care and whose status was known at the time of discharge from the EID program increased dramatically in Tanzania and Uganda over the course of the QI intervention.
This analysis has a number of limitations. The PHFS was designed as an implementation effort to support health workers to use QI approaches to change how they delivered care following the 2010 World Health Organization (WHO) Guidelines on HIV and infant feeding 21 and the 2012 WHO programmatic update for PMTCT. 22 Since control groups were not included within the PHFS, it is therefore possible that factors other than the QI intervention per se led to part or even all of the decrease in HIV transmission. One obvious factor that probably contributed to the decrease in HIV prevalence is the switch to using option B+. The first reduction in Tanzania occurred 2 months before the start of the QI intervention and 5 to 7 months after the switch to option B+. It therefore seems likely that the change to more effective treatment was a main contributor to the reduction in transmission in these countries. On the other hand, option B+ was launched in Uganda in January to March 2013, while the reductions in transmission occurred in November 2013 and August 2014 in the sites with baseline data. The second reduction was 16 months after the introduction of QI approaches in these facilities and these were likely a key contributor. The process indicators reported in the Uganda country paper within this supplement 23 improved in the final quarter of 2013 and could therefore account for all or much of the reduction in transmission seen in August 2014. The sites in Tanzania and Uganda saw a dramatic increase in the number of infants who were retained in care until their HIV status was known at the time of discharge from the EID program. Retention was a key aim of the QI teams in these facilities and this likely contributed to more infants benefiting from the new treatment. Specific changes that these sites implemented to improve retention are described in JIAPAC-18-08-SA-1100.
The PHFS was designed to build on existing QI approaches in each country. The design did not include a controlled study to assess the effectiveness of different components of the approaches. We believe that our general approach of (1) building health worker skills to use QI to change how care is delivered and supporting them to apply these skills through (2) on-site coaching, and (3) peer-to-peer learning opportunities are generalizable, but the details of how these 3 elements are applied need to vary based on local context.
Other limitations pertain to the data used in this study. Each country had existing PMTCT strategies and data systems. The project worked within these existing systems rather than developing parallel, project-centered data systems. This fostered country ownership and was helpful for generating lessons about how to spread learning to new facilities within each country; but as a result, we had to use a different definition of HIV transmission in each country, making project-level analysis of data challenging. Because of this, we can only report data by country rather than aggregated across all countries. Additional limitations include data quality issues related to the use of facility registers and the short duration of data collection in Kenya, which may explain why no shift in HIV prevalence was found. In addition, complete data were not available for all facilities. This was particularly an issue in Uganda, where less than half of the sites had data before the QI intervention.
This is one of very few PMTCT program evaluations that have measured HIV transmission through the end of breastfeeding. A recent systematic review of interventions to improve PMTCT programs identified only 2 studies that measured vertical transmission at 12 months or longer. 24 Aluisio found that 18.0% of HEI seen between 1999 and 2005 were infected at 12 months in Nairobi, Kenya. 25 Kalembo et al found that 10.8% of HEI seen between 2004 and 2006 were infected at 18 months in Mwanza, Malawi. 26 Now that there are global targets to reduce HIV transmission through weaning to below 5%, it is imperative that implementers and researchers measure this on a routine basis for all breastfed infants (not just EID). Quality improvement approaches can be used to support more mothers and infants to remain in care and to reduce HIV transmission.
Footnotes
Authors’ Note
These contents in this document are those of the authors and do not necessarily represent the views of PEPFAR, USAID, or the U.S. Government. WHO, IHI, UNICEF, and USAID came together to design and initiate the PHFS. The success of the partnership was ensured by the combined efforts of Ministries of Heath, national and district health teams, health facility staff, and community workers/volunteers.
Acknowledgment
The authors would like to acknowledge Lani Marquez and Simon Hiltebeitel for their knowledge management support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was provided by the US President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development (USAID) and its Applying Science to Strengthen and Improve Systems (ASSIST) Project, implemented by University Research Co., LLC (URC) through Cooperative Agreement Number AID-OAA-A-12-00101. This was supported by USAID and PEPFAR.