
Abstract
Objective:
We examined patterns of contraceptive utilization by HIV status among women in Cameroon, hypothesizing that women living with HIV would utilize contraception at higher rates than their HIV-negative peers.
Methods:
Deidentified, clinical data from the Cameroon Baptist Convention Health Services (2007-2013) were analyzed (N = 8995). Frequencies compared outcomes between women living with HIV (15.1%) and uninfected women. Multivariate analyses examined associates of contraceptive utilization and desire to become pregnant.
Results:
Contraceptive utilization was associated with higher education, living with HIV, monogamy, and higher parity (P < .001). Women living with HIV had 66% higher odds of using contraceptives than their negative peers (odds ratio [OR]: 1.66, confidence interval [CI]: 1.45-1.91, P < .001). Polygamous women had 37% lower odds of using contraceptives compared to monogamous women (OR: 0.63, 95% CI: 0.52-0.75, P < .001).
Conclusion:
Increasing contraceptive utilization in resource-constrained settings should be a priority for clinicians and researchers. Doing so could improve population health by reducing HIV transmission between partners and from mother to child.
What Do We Already Know about This Topic?
Scientific and clinical communities are aware that modern contraception utilization in resource-constrained settings is below optimal levels; these low levels are associated with unintended pregnancies and HIV transmission.
How Does Your Research Contribute to the Field?
We examine associates of modern contraceptive utilization in Cameroon, a resource-constrained setting, and find that utilization is associated with demographics, cultural practices, and living with HIV.
What Are Your Research’s Implications toward Theory, Practice, or Policy?
The finding that women living with HIV had higher odds of using modern contraception alludes to the possible benefit of coordinated care in promoting modern contraceptive utilization; our finding that polygamy and contraception nonuse are associated highlights the need for culturally informed policies that promote contraception within the local cultural context.
Introduction
Appropriate and correct use of modern contraceptives reduces rates of maternal and neonatal mortality by preventing unplanned pregnancies, lowering risk of contracting or transmitting sexually transmitted infections (when barrier methods are used), and reducing the likelihood of contracting or transmitting HIV. 1 –5 Despite the recognized benefits of using modern contraceptives—defined by the World Health Organization as male condoms, female condoms, oral contraceptive pills, intrauterine devices, contraceptive implants, and injectable contraceptives—improving modern contraceptive utilization rates in resource-constrained settings continues to be challenging, due to sociocultural preferences and economic considerations that act as barriers to contraceptive utilization. 3 –10 These notable barriers negatively affect contraceptive utilization rates in sub-Saharan Africa, the poorest region of the world with the highest rates of HIV infections in women. 2,7 –9,11,12 Although epidemiological data on contraceptive utilization in global settings are informative to intervention work and policy development, these data are often unavailable or difficult to access due to sensitivity of this topic (reproduction and contraceptive utilization). 7 –9,13 –15 Considering the need to comprehensively understand associates of contraceptive utilization, specifically to inform better clinical care, shape health policies, and enhance the effectiveness of interventions designed to increase utilization of modern contraceptives, we examined patterns of contraceptive utilization across Cameroon by evaluating multi-regional clinical data from the Cameroon Baptist Convention Health Services (CBCHS), one of the largest providers of health care in the nation. 15
The CBCHS includes 5 hospitals, 24 health centers, and 43 primary health care centers; the CBCHS was established in 1936. The CBCHS has since grown into one of the largest providers of clinical and preventive services, including comprehensive women’s health care, in Cameroon. 15 –17 The CBCHS’ services include women’s health care programs at 8 urban, semi-urban, and rural sites (located in 6 of the 10 regions in Cameroon); these women’s health care programs offer cervical and breast cancer screening, treatment of reproductive tract infections, and contraceptive services including the provision of modern contraceptives. Additional information about the CBCHS, its work in Cameroon, and its nationwide infrastructure is described elsewhere. 18 –20
Cameroon’s HIV prevalence is 4.5%, with a 7.8% HIV prevalence rate in pregnant women; yet, only 23% of adults living with HIV received antiretroviral therapy and only 16% of women of childbearing age used modern contraception. 21 –25 Data from the Cameroon Demographic and Health Surveys show wider variability in contraceptive utilization across method type and age-group. 25 Younger Cameroonian women were more likely to use male condoms as compared to older Cameroonian women, while older Cameroonian women utilized injectable contraceptives at higher rates than their younger peers. 25 Recent smaller studies in Cameroon found that although progress has been made to assess and meet contraceptive needs, economic and sociocultural barriers to contraceptive access and use persist as strong barriers. 26 –29 Other examples of known barriers to contraceptive usage include access to health care (and modern contraceptives), individual-level educational attainment, health knowledge about fertility and contraception, parity (number of children a woman has given birth to), age, employment status, and whether or not using contraceptives is acceptable to the woman’s male partners. 24 –31 Employment status and acceptability to male partners reflect a woman’s level of autonomy, empowerment, and/or social status, all of which have been found to be associated with a range of women’s health behaviors in resource-constrained settings. 31 –33
Since women living with HIV should be engaged in routine health care, and there has been a global movement to couple HIV treatment services with ancillary health care services (eg, cervical cancer screening, access to contraceptives, etc), we hypothesize that Cameroonian women living with HIV will have a higher rate of modern contraceptive utilization, even after controlling for personal characteristics. Conversely, considering polygamy (having co-wives) is a relatively common cultural practice in Cameroon with up to a quarter of Cameroonian women having co-wives, 34 we hypothesize that women in polygamous relationships will have lower odds of using modern contraceptives. Considering the multifaceted decision-making process around contraceptive utilization, we tested the aforementioned hypotheses using multivariate analyses.
Methods
Study Design and Participants
Data were drawn from the CBCHS Women’s Health Program (WHP, established in 2007). Our study is cross-sectional; we analyzed data from the CBCHS WHP collected during a 6-year period, from the WHP’s inception in 2007 to 2013. The sample of 8995 included women of reproductive age (16-45 years) who were screened for cervical cancer. We excluded women who had a hysterectomy (n = 303) and women who did not know their HIV status (n = 296).
Outcome Measures
Two outcome variables representing fertility preferences were included: (1) current use of modern contraception and (2) desire to become pregnant soon. Contraception utilization was defined as currently using any contraceptive method. The measure was then refined by categorizing methods of contraception reported by patients. These included sterilization, intrauterine device, contraceptive implants, injectable contraceptives, oral contraceptive pills, and/or condoms (both male and female condoms), lactation amenorrhea method (LAM) - commonly referred to as breastfeeding, withdrawal calendar method, and traditional (country) method. Women reporting current use of sterilization, intrauterine device, contraceptive implants, injectable contraceptives, oral contraceptive pills, and/or condoms (both male and female condoms) were coded as 1, “Using a modern method.” The remainder was coded as 0, “Not using a modern method.” Fertility desires were defined as hoping to become pregnant in the next few months. Women hoping to become pregnant in the next few months were scored as 1 and all others were coded as 0.
Independent Measures
We included 3 health variables: self-reported HIV serostatus (HIV-infected or positive and HIV-uninfected or negative), parity, and number of children desired. HIV serostatus was defined as those reporting their HIV status as negative or positive. Parity was specified by a categorical variable: 0 children (referent), 1 to 2 children, 3 to 4 children, and 5 or more children. Likewise, the number of children desired was measured as a categorical variable: 0 children (referent), 1 to 2 children, 3 to 4 children, and 5 or more children.
We included 5 sociodemographic variables previously found to be associated with contraceptive utilization or potentially relevant to contraceptive utilization in Cameroon: age, education, employment status, marital status, and polygamy (presence of co-wives). Age was specified as a categorical variable with the following groups: 16 to 24 years old (referent), 25 to 34 years old, and older than 35. Cutoffs were chosen based on a population median age of 18 years, female life expectancy of 59 years, and average age at first birth of 19 to 20 years. 35,36 Education was measured with a categorical variable: no formal education (referent), primary education (grades 1-6), secondary education (grades 7-12), and postsecondary education. Employment was measured by a categorical variable: not employed (referent), employed, and student. Likewise, marital status consisted a categorical variable: not married (referent), married, and widowed/divorced. Finally, polygamy was measured with a single binary variable: 1 = has co-wives, 0 = no co-wives.
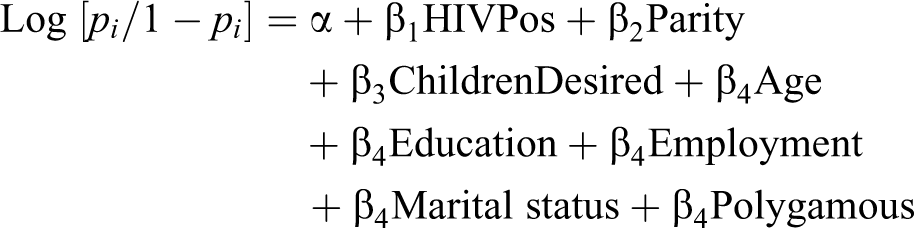
Statistical Analyses
All analyses were conducted using Stata version 15. Univariate statistics were computed, stratifying by HIV serostatus in order to compare characteristics of women living with HIV to their HIV-negative peers in our sample. Logistic regression models were used to examine associations between fertility preferences (modern contraceptive utilization and desire to become pregnant soon), fertility/health measures, and sociodemographic characteristics. Minimal statistical significance was reported at P < .05. The model predicting modern contraceptive utilization and desire to become pregnant soon is specified as:
Ethical Approval and Informed Consent
Ethical approval to conduct the overall study was obtained from the local, CBCHS institutional review board (IRB, #IRB2015-21). Ethical approval to analyze CBCHS’ deidentified data for this particular study was obtained at the University of Alabama at Birmingham IRB, federal-wide assurance FWA00005960 for protocol number #E160405005. Since this specific study evaluated existing programmatic, medical record data, informed consent was not obtained for individual records.
Results
Sample Characteristics
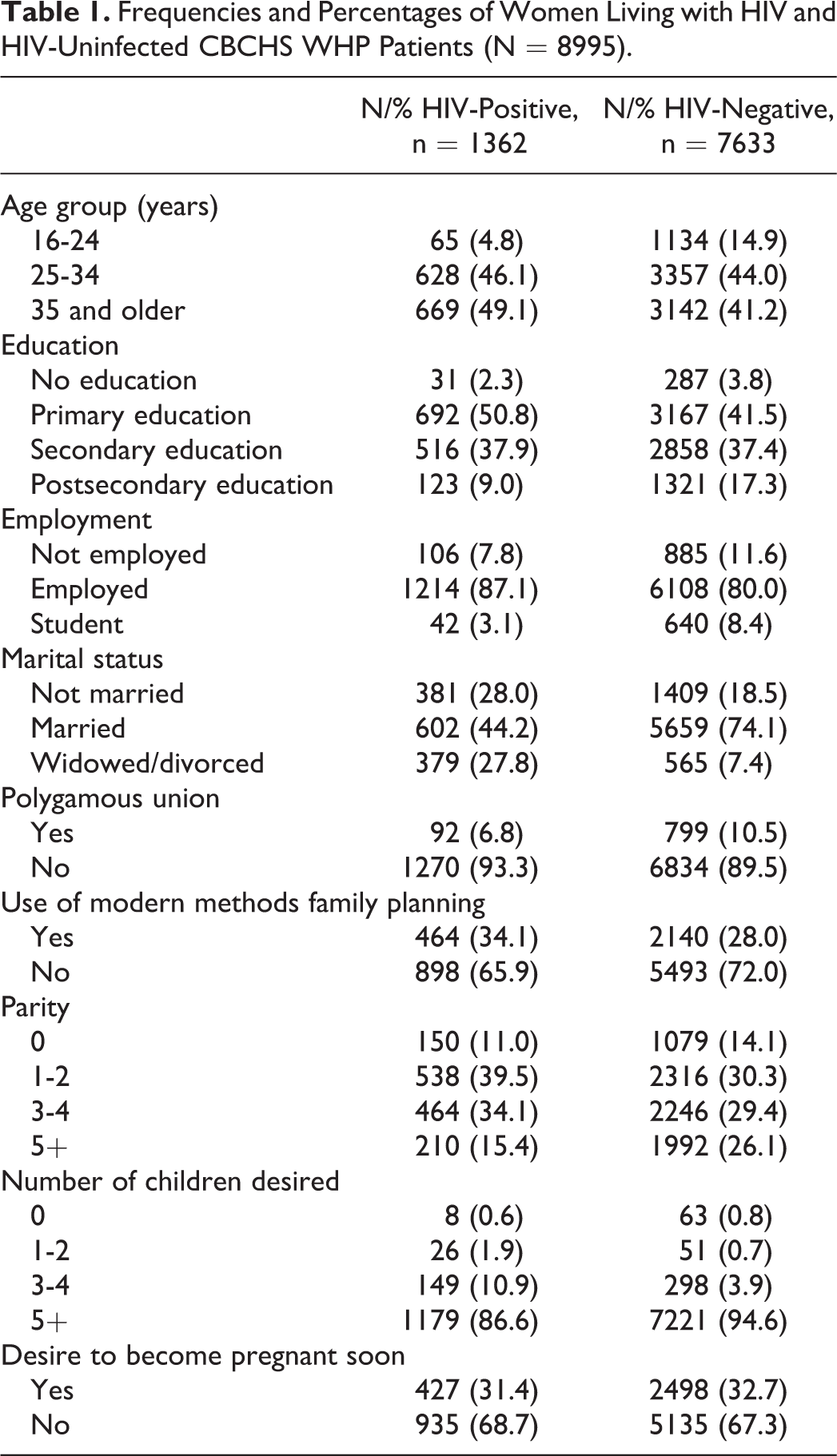
In our study sample, modern contraceptive utilization was low, with 34.1% of the women living with HIV reporting using a modern contraceptive method and 28.0% of HIV-negative women reporting modern contraceptive utilization (Table 1). About half of the women living with HIV in our sample (49.1%) and 41.2% of the HIV-negative women were aged 35 or older. Forty-seven percent of the women living with HIV (46.9%) and 54.8% of the HIV-negative women had higher than a primary level of education. The majority of our sample were employed (87.1% of women living with HIV and 80.0% of uninfected women). Less than half of the women living with HIV were married (44.2%), whereas almost three-fourths of the HIV-uninfected women were married (74.1%). Eleven percent (10.5%) of the HIV-negative women were in a polygamous union, compared to 6.8% of women living with HIV. Approximately half of the sample had 3 or more children (49.5% of women living with HIV and 55.5% of their HIV-uninfected peers). The desire to have 5 or more children was high, with 86.6% of women living with HIV desiring 5 or more children and 94.6% of the HIV-negative women desiring 5 or more children. Finally, the desire to become pregnant in the next few months was similar irrespective of HIV serostatus (HIV positive: 31.4%; HIV negative: 32.7%).
Frequencies and Percentages of Women Living with HIV and HIV-Uninfected CBCHS WHP Patients (N = 8995).
Contraceptive Utilization
Table 2 presents the multivariate results related to modern contraceptive utilization and fertility desires. Women between the ages of 25 and 34 had approximately 20% lower odds of modern contraceptive utilization relative to younger women 16 to 24 years old (odds ratio [OR]: 0.81, 95% confidence interval [CI]: 0.69-0.96, P < .05). Likewise, women in our sample who were 35 years old or older had almost 50% lower odds of using modern contraception relative to younger women aged 16 to 24 years old (OR: 0.51, 95% CI: 0.42-0.61, P < .001). Women with postsecondary educational attainment had over 4 times higher odds of contraceptive utilization relative to women with no education (OR: 4.31, 95% CI: 3.01-6.16, P < .001). Women with primary and secondary education had 2.5 and 3 times higher odds of modern contraceptive utilization relative to women with no education (OR: 2.49, 95% CI: 1.77-3.50, P < .001, OR: 3.00, 95% CI: 2.13-4.23, P < .001, respectively). Students had higher odds of using modern contraception relative to unemployed women (OR: 1.72, 95% CI: 1.36-2.17, P < .001). Being married was associated with 26% lower odds of modern contraceptive utilization compared to unmarried women (OR: 0.74, 95% CI: 0.64-0.85, P < .001), and being widowed or divorced was associated with 48% lower odds of modern contraction use compared to unmarried women (OR: 0.52, 95% CI: 0.42-0.63, P < 0.001). The presence of co-wives (being in a polygamous relationship) was negatively associated with modern contraceptive utilization; women in polygamous relationships had approximately 40% lower odds of using modern contraceptives (OR: 0.63, 95% CI: 0.52-0.75, P < .001) compared to their nonpolygamous peers. Women living with HIV had 66% higher odds of using modern contraceptives compared to HIV-negative women (OR: 1.66, 95% CI: 1.45-1.91, P < .001). Likewise, women with higher parity had higher odds of using modern contraception compared to women with no children (OR: 1.74, 95% CI: 1.45-2.08, P < .001; OR: 4.01, 95% CI: 3.28-4.91, P < .001; OR: 5.32, 95% CI: 4.26-6.63, P < .001 for 1 to 2, 3 to 4, and 5 or more, respectively).
Logistic Regression Odds Ratios of the Associates of Modern Contraceptive Utilization and Desired Pregnancy.a

aN = 8995.
b P < .05.
c P < .001.
d P < .01.
Intent to Become Pregnant
Compared to women aged 16 to 24, women aged 25 to 34 years had 2.1 times higher odds of desire to become pregnant soon (OR: 2.1, 95% CI: 1.80-2.47, P < .001), and women aged 35 years old or older had 2.7 times higher odds of desire to become pregnant soon (OR: 2.69, 95% CI: 2.25-3.21, P < .001). Women with a postsecondary education had 33% lower odds of desiring to become pregnant soon relative to women with no formal education (OR: 0.67, 95% CI: 0.49-0.92, P < .05), and women who were currently students had 44% lower odds of desire to become pregnant soon (OR: 0.56, 95% CI: 0.44-0.72, P < .001). Relative to unmarried women, married women had 2.9 times higher odds of desire to become pregnant soon (OR: 2.91, 95% CI: 2.51-3.70, P < .001), and the presence of co-wives was associated with higher odds of desire to become pregnant soon (OR: 1.32, 95% CI: 1.11-1.56, P < .001). Finally, women with higher parity had lower odds of desire to become pregnant soon relative to women with no children (OR: 0.39, 95% CI: 0.33-0.46, P < .001; OR: 0.09, 95% CI: 0.08-0.11, P < .001; OR: 0.03, 95% CI: 0.03-0.04, P < .001 with increasing parity).
Discussion
We hypothesized that Cameroonian women living with HIV would have a higher rate of contraceptive utilization and higher odds of using contraceptives than their HIV-negative peers. We also hypothesized that Cameroonian women in polygamous relationships (women with co-wives) would have lower odds of using modern contraceptives as compared to their nonpolygamous peers. We found strong statistical support for both hypotheses. Multivariate analysis showed that women who reported living with HIV had higher odds of utilizing modern contraception, even after controlling for personal characteristics.
Women living with HIV theoretically should have ongoing contact with their health care system, and this routine engagement may improve access to contraception counseling and services, resulting in increased contraceptive utilization. 37,38 Previous studies (as well as this study) have found evidence in support of coupling HIV treatment services and contraception counseling 37,38 ; however, the benefits and challenges of comprehensive women’s health care in global settings are not fully understood and warrant further examination. For example, a recent study from South Africa found women living with HIV (these are women who are likely to be engaged in health care) were more likely to have an unplanned pregnancy than their uninfected peers, which is both surprising and worrisome. 39 Having said this, it is critical to note that South Africa is a unique setting with a generalized HIV epidemic wherein pregnancy outcomes may be influenced by cultural indicators, similar to the way in which polygamy was associated with modern contraceptive utilization in our study in Cameroon.
Thus, modern contraceptive utilization is not exclusively determined by general health care access but may be enhanced by increasing individual-level health care knowledge about contraceptive options and efficacy of each type of contraceptive available in that setting, thoughtfully addressing cultural barriers and beliefs to modern contractive use and bolstering access to comprehensive, multifaceted health care that couples key services in an effort to improve overall population health. These individual and structural interventions could then lead to reductions in HIV transmission between sexual partners and from mothers to newborns.
Limitations
Limitations should be considered when applying study findings. First, women enrolled in the CBCHS WHP were self-selected, potentially leading to bias. Women in our sample, those enrolled in the CBCHS WHP, utilized modern contraception at a rate of 29.0% as compared to the national rate of about 16%. 20,29 Although this provides some support for the benefit of coupling contraceptive services with other health care services (eg, HIV services, cervical cancer screening, etc), these sample characteristics illustrate that (even though relatively large) our study sample may not align with the sociodemographic profile of all Cameroonian women of childbearing age, reducing generalizability. Since this study was a secondary analysis of existing data, we were unable to address this potential bias. Second, medical and enrollment records were originally collected and stored in hard copy on paper; thus, misclassification from reading and manually keying records could have occurred, even with auditing and multiple entry techniques applied. Third, because these data were self-reported and were not triangulated from a secondary source such as pharmacy or laboratory records, a desirability bias may have skewed the results. Namely, self-reported HIV serostatus is particularly prone to reporting bias toward reporting HIV-negative status among women who know they are infected. Lastly, cross-sectional data cannot provide information on causality; thus, we are unable to say certain behaviors or participant characteristics lead to higher or lower contraceptive utilization. Future studies should address these limitations by conducting longitudinal trials of health care utilization that not only monitor behavior over time but also seek to address the educational and structural deficiencies, along with cultural roadblocks that are associated with lack of modern contraceptive utilization.
Conclusion
Our study makes 3 significant contributions to the scientific literature. First, we found evidence that utilization of modern contraception in Cameroon is alarmingly low. This low utilization could lead to unplanned pregnancies and transmission of HIV from mother to infant. Second, we found a statistical relationship between modern contraceptive utilization and polygamy, an understudied cultural practice that appears to have implications for health. Third, our study provides some support for the potential benefit of pairing contraceptive services with HIV counseling, testing, and treatment services.
Considering the limited availability of national data sets that include HIV serostatus and behaviors related to contraception, epidemiological and intervention trials that engage local partners, such as the CBCHS, have the potential of uncovering new knowledge that is pertinent to ongoing global efforts to address unmet contraception needs in both women living with HIV and HIV-negative women, ultimately leading to improved population health and reductions in maternal and child mortality.
Footnotes
Authors’ Note
H.B. was lead author and contributed to the conceptualization and writing of this manuscript. K.R.H. developed and conducted the statistical analyses and wrote the methods and results sections. J.D.O. provided conceptual guidance and contributed to the writing. S.M. and R. conducted the data collection and produced the data set. M.K. contributed to the writing. T.W. and E.W. provided background information on the CBCHS and edited the manuscript. A.T. was the senior author, clinically validated the results, and is the liaison between the CBCHS and the University of Alabama at Birmingham. Data are available from S.M. or K.N. in an Excel workbook. The authors provide their consent for publication of this manuscript.
Acknowledgements
The authors would like to acknowledge the good work and partnership of the CBCHS, especially the outstanding work done by the WHP nurses, without which this study could not have occurred. The authors would also like to acknowledge the UAB Sparkman Center for Global Health for its long-term commitment to supporting capacity building and action research in resource-constrained global settings.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.