
Abstract
Aim:
To collect data pertaining to oral drug provocation testing (DPT) in hospitalized patients with antiretroviral (ARV)/antitubercular agent–induced rashes.
Methods:
Patients with cutaneous adverse drug reactions (ADRs) to ARV/antitubercular drugs and who underwent oral DPT during a 5-year period were included in this study.
Results:
Data were collected from the records of 21 patients. Of the 21, 19 had HIV infection. The most commonly implicated drug was nevirapine (NVP), followed by cotrimoxazole and antitubercular agents. Of the 11 ADRs that occurred on rechallenge, the ADR on rechallenge was similar in clinical presentation to the initial ADR in 6 patients, while a different rash was elicited in 5 patients.
Conclusion:
Oral DPT is a safe and effective tool to accurately diagnose ADRs, especially in patients on multiple drugs and in situations such as HIV infection and tuberculosis where second-line agents are expensive and/or not easily available through the national AIDS control/tuberculosis programs.
Introduction
Adverse drug reactions (ADRs) are commonly encountered clinical problems in dermatologic practice. In a hospital-based scenario, patients are often on multiple drug regimens, particularly in the setting of HIV infection and/or tuberculosis (TB). Multidrug regimens make the diagnosis of drug allergies complicated. Among the many forms of testing that can be used to identify the implicated drug in patients with cutaneous ADRs, oral drug provocation tests showed the highest sensitivity. 1 In addition, in the setting of underlying HIV/TB, it becomes vital to identify the culprit drug with some degree of certainty, since the second-line regimens tend to be expensive/unavailable in the developing world. Antitubercular and antiretroviral (ARV) drugs are notorious for producing a wide spectrum of cutaneous ADRs, ranging from simple urticaria to life-threatening Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). This makes it all the more difficult to perform oral drug provocation tests in these patients. 2 There are no clear guidelines for drug rechallenge in the setting of HIV/TB, and management often needs to be tailored to suit individual patient scenarios. We hereby present a series of cases of cutaneous ADRs predominantly in patients with HIV/TB, wherein the oral drug provocation tests were the only available means for reliably identifying the suspected drug in order to establish appropriate ARV and/or antitubercular treatment regimens in accordance with the national guidelines for HIV/TB.
Methods
During a period of 5 years (2010-2015), all cases of cutaneous ADRs to ARV/antitubercular drugs in whom oral drug rechallenge was performed were included in this retrospective study after ethical clearance from the institution ethics committee (IEC Study Ref. No. 21/2014). All patients with documented serious cutaneous ADRs (including intensely pruritic bright red maculopapular rashes) which warranted stoppage of the ongoing drug therapy were selected for oral DPT. In all these patients, rechallenge protocols had been formulated on an individual basis, since patients were on multiple drugs, with reactions to more than 1 drug in some cases. Rechallenge or challenge to the cross-reacting drug was always performed in the inpatient setting after a drug-free washout period lasting 5 elimination half-lives for the suspected drug. Suspected drugs were reintroduced one by one, starting at one-fourth of the recommended dose, with doubling of the dose every 2 days, until the full therapeutic dose was reached or an ADR occurred, whichever came first, except in the case of ARV drugs wherein full dose of the nonnucleoside reverse transcriptase inhibitor (NNRTI) and nucleoside reverse transcriptase inhibitor (NRTI) were given individually. Subsequent drugs were reintroduced once a patient tolerated full dose of the first drug with no adverse event. Inpatient and outpatient charts of these patients were reviewed retrospectively, and their demographic details and clinical data were recorded while maintaining confidentiality. Summary statistics such as mean/ average were performed on the data collected, and these are presented in the results section.
Results
Twenty-one patients, comprising 14 females and 7 males, were included in this study. Nineteen of these patients had HIV infection. In all 21 cases, the diagnosis of ADR was made based on clinical history and examination, with relevant blood tests along with causality assessment as determined by Naranjo score. 3 The incubation period for the rash ranged from 4 to 60 days, with an average incubation period of 21.4 days. The drug-free period between disappearance of rash and performance of rechallenge ranged from 2 weeks to 18 months. A total of 11 patients had positive results (reappearance of a rash) on oral rechallenge with the same/similar class of cross-reacting drugs (Table 1). For all HIV-infected patients with a suspected sensitivity to nevirapine (NVP), challenge was performed with efavirenz (EFV), except in 1 patient who was rechallenged with NVP itself, as we did not have access to any documentation that confirmed an initial rash to NVP. Of the 11 ADRs that occurred on rechallenge, the ADR on rechallenge was similar in clinical presentation to the initial ADR in 6 patients, while a rash of different morphology compared to the initial ADR was elicited in 5 patients. The most common suspected drugs implicated in the initial ADR were ARV drug (NVP), followed by cotrimoxazole, and antitubercular therapy, with agents from more than 1 category being tested in several patients. Seven patients had severe reactions such as erythema multiforme, erythroderma, SJS, and drug hypersensitivity syndrome (DHS), while 14 patients had a maculopapular rash, among whom 11 had systemic symptoms/ laboratory abnormalities. One patient had severe generalized pruritus with altered liver function tests, without any rash. Patients with suspected NVP sensitivity were challenged with EFV based on 30% cross-reactivity between the 2 drugs.
Spectrum of Rash on Rechallenge or Challenge to Cross-Reacting Drugs.

Abbreviations: ATT, antitubercular therapy (consists of 4 drugs—isoniazid, rifampicin, pyrazinamide, and ethambutol); DHS, drug hypersensitivity syndrome; ART, antiretroviral therapy; ZLN, zidovudine + lamivudine + nevirapine; TLE, tenofovir + lamivudine + efavirenz; M, male; F, female.
Discussion
An ADR consists of “a response to a drug that is noxious and unintended and occurs at doses normally used in man for the prophylaxis, diagnosis, or therapy of disease.” 4 The ADRs range in severity from minor reactions such as pruritus/urticaria to severe life-threatening reactions including anaphylaxis, SJS/TEN, and DHSs. Many ADRs are immunologically mediated mostly through type 1 (immediate) or type 4 (delayed) hypersensitivity reactions. The type 4 hypersensitivity reactions (mediated by T cells) are usually more difficult to diagnose due to the long/variable time period between drug administration and appearance of the ADR. Also, the intercurrent infections such as respiratory or urinary infections are known to precipitate or worsen ADRs through nonspecific viral stimulation of cytotoxicity. 5 Patients experiencing ADRs are faced with clinical, emotional, and financial costs, not to mention the inevitable undermining of the doctor–patient relationship in some instances.
Virtually every drug known to man is capable of producing a cutaneous ADR, at least in theory, although some drugs are higher on the list. In this study, we dealt mainly with immunologically mediated delayed reactions to antitubercular and ARV drugs. According to previous studies, the incidence of ADRs to antitubercular agents ranges from 7% to 45%, with pyrizinamide being responsible for the majority of reactions, followed by isoniazid. 6 -10 In our current series, the most common culprit drug was isoniazid. Patients with HIV infection are at a significantly higher risk of ADRs, the reasons being multifactorial, including changes in drug metabolism, oxidative stress, cytokine profiles, and immune hyperactivation. 5,11 Many of the drugs used for the treatment of HIV infection and the associated opportunistic infections also cause hypersensitivity reactions, through a combination of genetic, immunologic, and viral/host factors. All the NNRTIs, including NVP, EFV, delavirdine (DLV), and etravirine, are capable of causing a rash, with the incidence of NVP rash ranging from 17% to 32% of patients. 12 In majority (12/21) of our patients, the suspected drug was NVP, which was indirectly established by a negative result on challenge to EFV (10/21 patients). The conclusion that patients who did not react to rechallenge with EFV probably had an NVP rash initially was reached based on the assumption that the most likely culprit drug in the zidovudine + lamivudine + nevirapine regimen is NVP and the fact that these patients subsequently tolerated EFV-based regimens (ZLE) without any rash. Risk factors for ADRs to NVP include higher CD4 count, female gender, opportunistic infections, immune reconstitution, hepatitis B coinfection, and several genetic polymorphisms, which are still being looked at in various studies. 12 In our series, 8 of 19 HIV-infected patients had CD4 counts ≤200 cells/mL, with majority (11/19) being females. None of these patients had coexisting hepatitis B infection or fulfilled the criteria for immune reconstitution inflammatory syndrome (IRIS).
Although there is no universally accepted method for causality assessment in ADRs, the diagnosis of ADRs is invariably based on the physician’s judgment, in combination with a number of causality assessment algorithms, the most widely used ones being the Naranjo probability scale and the World Health Organization - Uppsala Monitoring Centre (WHO-UMC) causality system. 3,13 We used the Naranjo scale to assess our patients with ADR at the time of initial presentation, with majority of the patients obtaining scores in the range of 7 to 9, implying “probable” ADRs. Skin tests for ADRs, including prick tests, patch tests, and intradermal tests, can be used to pick up immunoglobulin E-mediated immediate hypersensitivity reactions and occasionally specific types of delayed reactions, particularly exanthematous reactions. However, their usefulness in the clinical setting is limited, as they are not available in standardized forms for most drugs, and in many cases the specific antigenic determinant/drug metabolite responsible for a particular reaction is unknown. 5 In vitro tests such as the lymphocyte transformation test are essentially research tools, and the results cannot be reliably extrapolated to the clinical setting. In the light of all these constraints related to in vivo and in vitro testing, DPT is widely regarded as the “gold standard” to establish or exclude drug hypersensitivity, since it accurately clinically reproduces the suspected ADR while overcoming the drawbacks of all the methods described earlier. 14 The DPTs should be considered only after weighing the risk–benefit ratio in an individual patient and should be undertaken with extreme caution only in a hospital setting, especially in cases where the initial reaction was severe. Indications for DPT are to (1) exclude hypersensitivity when the history is nonsuggestive, (2) prove hypersensitivity when the history is suggestive and allergologic tests are negative/inconclusive/unavailable, (3) provide safe drugs in proven hypersensitivity, and (4) exclude cross-reactivity in proven hypersensitivity. 14 Although DPT is not recommended in severe drug hypersensitivity reactions, we weighed the risks and undertook DPT with caution in a few cases of DHS, erythroderma, and SJS/EMF, when no alternative drug was available or when the alternative was expensive/toxic/costly/unavailable. In some cases, the DPT results were surprising, for example, in 1 case of HIV infection with suspected DHS to NVP, we were able to prove tolerance to NVP/EFV and instead found the offending agent to be lamivudine (3TC) (case no. 5 in Table 1). The 3TC is generally considered to be one of the safer ARV drugs, although a recent case series indicates that 3TC rashes may be more common than we think. 15
The time interval between resolution of rash and performance of DPT should ideally consist of at least 5 elimination half-lives for the drug in question. Generally, DPT is not recommended earlier than 4 weeks after resolution of the ADR, which was the protocol followed by us, except in extenuating circumstances such as one case of tuberculoma of the brain, in whom therapy could not be delayed, or in situations where patients were lost to follow-up after experiencing an ADR, only to reappear for treatment after a prolonged gap, the longest being 18 months. The abovementioned patient reacted to both isoniazid and ethambutol on DPT (which was performed after a 2-week interval) and was subsequently put on an alternative regimen consisting of rifampicin and levofloxacin, which the patient successfully completed with no further ADR. The DPT is not without its drawbacks, as evidenced by our HIV-infected patient (case no. 9 in Table 1) with a suspected SJS to NVP, who had a positive rechallenge to EFV (different rash), was referred to a regional center (national AIDS control organization) for protease inhibitor (PI)-based regimens but subsequently returned to an EFV-based regimen, which the patient tolerated for at least 2 years after initiation. Hence, both false positive and false negative results may be obtained by DPT, and in rare instances, a patient may inadvertently undergo spontaneous desensitization/ tolerance induction to the drug being tested for, as evidenced in the abovementioned case.
In certain situations patients require both antitubercular therapy (ATT) and ART, and as treatment of the opportunistic infection (TB) takes precedence according to guidelines, ATT is initiated first and ART added after the patient tolerates ATT for at least 2 weeks. However, we do still encounter patients who require both ATT and ART simultaneously, and when ADRs develop in such instances, all the drugs need to be stopped, followed by rechallenge. At our center, we perform rechallenge to ATT drugs first (in the order of least likely culprit drug to most likely, ie, ethambutol first, followed by rifampicin, isoniazid, and pyrazinamide last), stabilize the patient on standard/modified ATT according to the outcome of rechallenge, and wait for at least a couple of weeks (or longer if the CD4 count is favorable) before introducing zidovudine (ZDV) and 3TC first, followed by a suitable NNRTI (EFV) or PI, as the situation demands.
There are no clear protocols/guidelines for performing DPT, and interpretation of results is widely variable due to a number of reasons, one of which is called the “protopathic bias” implying that rash could be a sign of the disease process itself (eg, viral exanthem) and/or treatment of the disease could precipitate a rash in some instances (eg, ampicillin-induced rash in infectious mononucleosis). 16 Broadly, DPTs can be interpreted as follows: positive, suggestive, and negative. Similar to patch testing, the “results” of DPT need to be distinguished from the actual clinical “interpretation.” Rechallenge can be considered to be “positive” when the observed reaction is identical to the initial one, “suggestive” when the observed reaction is different/ milder than the initial one (can be considered to be a prodrome of the initial reaction), and “negative” when there is no reaction. 16 In our study also, this phenomenon was observed, wherein rechallenge produced either only pruritus or a rash of different/milder morphology than the initial event.
With our protocol (Figures 1 and 2), we were able to manage several patients who eventually tolerated the relevant combination regimen with avoidance of the culprit drug(s) and were hence able to avoid costly/toxic second-line treatments. Although our protocols were tailored to the needs of the individual patient, in the future we hope to establish protocol-based guidelines for the management of ADRs in patients on multiple drug regimens. Generation of this kind of data, although heterogeneous, is sorely needed if these relatively unexplored areas are to be further researched.

Suggested protocol for mild rash.
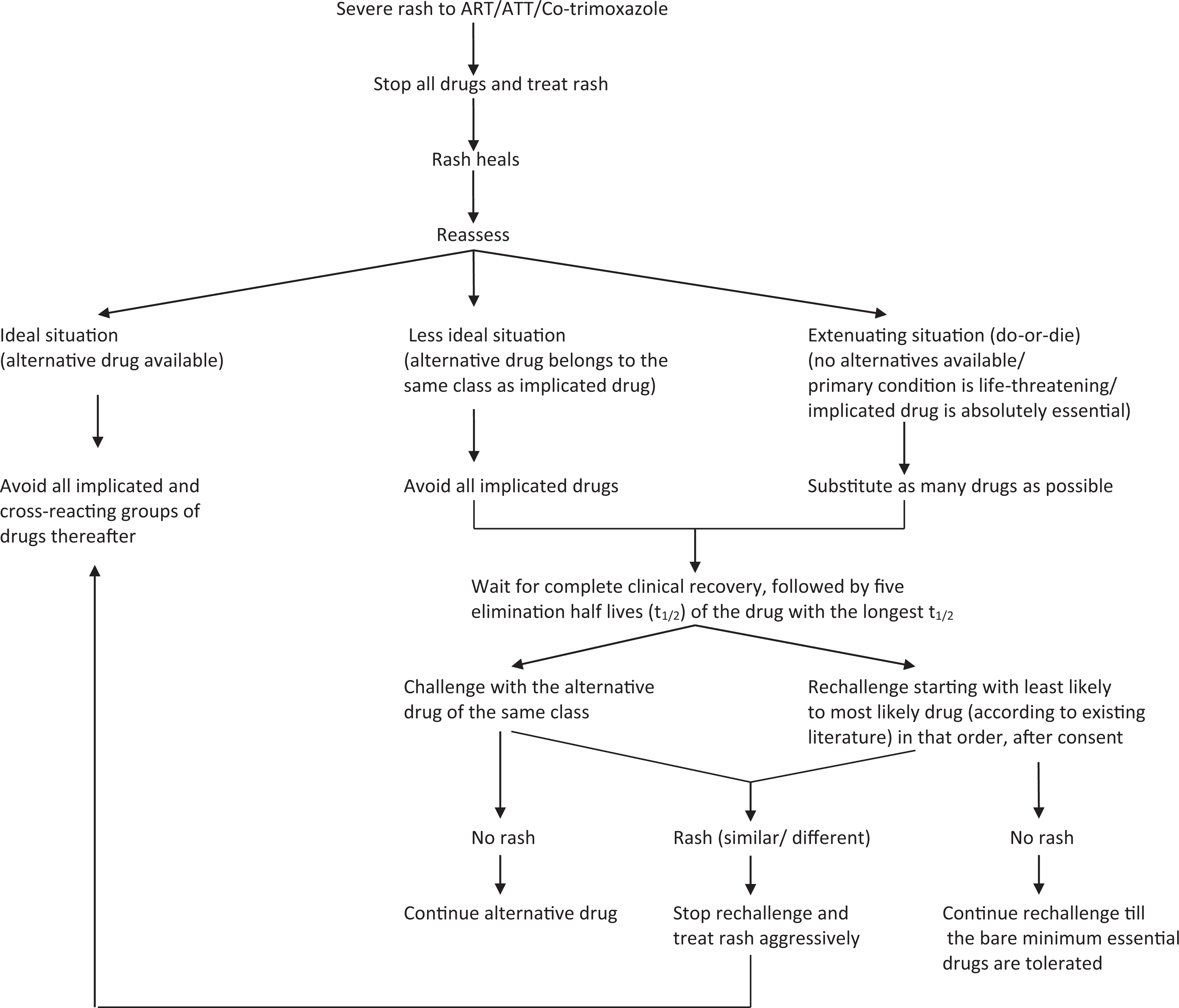
Suggested protocol for severe rash.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.