
Abstract
Background:
Concomitant use of several drugs for a patient is often imposing increased risk of drug–drug interactions. Drug–drug interactions are a major cause for concern in patients with cardiovascular disorders due to multiple co-existing conditions and the wide class of drugs they receive. This study is aimed to assess the prevalence of potential drug–drug interactions and associated factors among hospitalized cardiac patients at medical wards of Jimma University Medical Center, Southwest Ethiopia.
Methods:
A hospital-based prospective observational study was conducted among hospitalized cardiac adult patients based on the inclusion criteria. Patient-specific data were collected using structured data collection tool. Potential drug–drug interaction was analyzed using Micromedex 3.0 DRUG-REAX® System. Data were analyzed using statistical software package, version 20.0. To identify the independent predictors of potential drug–drug interaction, multiple stepwise backward logistic regression analysis was done. Statistical significance was considered at a p-value < 0.05. Written informed consent from patients was obtained and the patients were informed about confidentiality of the information obtained.
Results:
Of the total 200 patients, majority were male (52.50%) and with a mean(±standard deviation) age of 42.54(±7.89) years. Out of 673 patients’ prescriptions analyzed, 521 prescriptions comprised potential drug interactions and it was found that 967 drug interactions were present. The prevalence rate of potential drug–drug interactions among the study unit was 4.83 per patient and 1.44 per prescription regardless of the severity during their hospital stay. Overall the prevalence rate of potential drug interactions was 74.41%. Older age (adjusted odds ratio (95% confidence interval): 1.067 (2.33–27.12), p = 0.049), long hospital stay (⩾7 days) (adjusted odds ratio (95% confidence interval): 2.80 (1.71–4.61), p = 0.024), and polypharmacy (adjusted odds ratio (95% confidence interval): 1.64 (0.66–4.11), p = 0.041) were independent predictors for the occurrence of potential drug–drug interactions.
Conclusion:
This study demonstrated a high prevalence of potential DIs among hospitalized cardiac patients in medical wards due to the complexity of pharmacotherapy. The prevalence rate is directly related to age, number of prescribed drugs, and length of hospital stay. Pharmacodynamic drug–drug interaction was the common mechanism of drug–drug interactions. Therefore, close monitoring of hospitalized patients is highly recommended.
Background
Adverse drug events (ADEs) have been one of the major public health concerns to patients and health care professionals. Hospital adverse events are an important source of morbidity and mortality in different countries and settings and represent an important item of expenditure for health care systems and their prevention could be associated with a relevant cost saving. 1 One of the specific types of ADE is drug–drug interaction (DDI). 2 It is defined as pharmacological or clinical response to the administration of a drug combination which is different from that expected from the known effects of the two agents when given alone. The clinical result of a DDI may manifest as antagonism, synergism, or idiosyncratic. 3 It can be divided into pharmacodynamic (PD) and pharmacokinetic (PK) interactions. PD interactions occur when the combination of medications causes additive or antagonistic pharmacological effects and influence efficacy. PK interactions occur when there are changes in absorption, distribution, metabolism, and elimination. 4 They are often predictable and, therefore, avoidable or manageable.5,6
DDIs are more frequent in patients who are elder, hospitalized for a longer period of time, and/or receive more drugs per day.7–9 Maybe due to comorbid conditions, chronic therapeutic regimens, polypharmacy, and frequent modification in therapy, hospitalized patients are more likely affected by potential drug–drug interactions (pDDIs). The prevalence of pDDIs is close to 40% in patients taking five medications and exceeds 80% in patients taking seven or more medications.10,11
The incidence of cardiovascular diseases has significantly increased in the recent decades and considered as a leading cause of deaths worldwide. 12 Various studies suggest that cardiovascular patients are more often reported with pDDIs as compared to patients with other diseases. The possible reasons behind include older age, multiple drug regimens, PK or PD nature of drugs used in cardiology, and the influence of heart disease on drug metabolism.13,14 The pDDIs for a particular cardiovascular drug vary with the individual, the disease being treated, and the extent of exposure to other drugs.15,16
Different practice models and experience showed that the clinical pharmacists have a major role in preventing DDIs; especially by evaluating physicians’ prescriptions for possible DDI.17,18 Therefore, integrated professional interaction should be encouraged between health care professionals in order to optimize drug safety. Vigilance by health care workers, such as clinicians, pharmacists, and nurses in detecting, diagnosing, and reporting DDIs, particularly in at-risk individuals such as cardiac patients, is also vital for continued drug safety monitoring.
As a result, pDDIs have become a common concern and an important concept in terms of an appropriate prescription process.16,19,20 Hence, robust and accurate information regarding the potential adverse impacts of co-administration of drugs is critical for reducing the health impacts and costs of adverse events. 9 Different studies have been conducted to develop practical decision, support tools, and improve clinicians’ knowledge of prevalent and clinically important pDDIs encountered in their daily practice. In Ethiopia, inappropriate prescription of drugs with potential interactions causing serious risks to patient health has not been adequately studied among cardiac patients. Hence, this study sought to determine the type, prevalence, and characteristics of pDDIs and associated factors among inpatients receiving cardiovascular medications at medical wards of Jimma University Medical Center (JUMC).
Methods
Study design and setting
A hospital-based prospective observational study design was conducted during February to March 2017 at the internal medicine wards of JUMC among adults hospitalized with cardiac disorder who fulfill the inclusion criteria. JUMC is the only teaching and referral hospital in the southwestern part of Ethiopia with a bed capacity of 600. Geographically, it is located in the Jimma town 352 km southwest of Addis Ababa, the capital. It provides services for approximately 9000 inpatient and 80,000 outpatient clients per year with a catchment population of about 15 million people.
Study population
Hospitalized cardiac patients aged 18 years or older admitted to the internal medicine wards with a hospital stay of at least 24 h and those prescribed least two medications of any type were enrolled for the study. Patients visiting on an outpatient basis, unwilling to give consent, and those who died during hospital stay were excluded from the study. No sample size calculation and sampling technique were used. All patients admitted to medical wards with a diagnosis of cardiovascular disorder were included in the study. A total of 236 cardiac patients were admitted to medical wards of JUMC; from these, 200 patients who fulfilled the inclusion criteria were included for the final analysis.
Data collection, procedure, and quality control
A semi-structured questionnaire was developed by researchers from relevant literatures. Patient chart review and self-report were used to determine various variables. All medications that were prescribed during patient hospital stay (starting from admission to discharge) and administered to the patients were screened for pDDIs. Micromedex 3.0 DRUG-REAX® System (Thomson Reuters Healthcare Inc., Greenwood Village, CO, USA) was used to screen and classify pDDIs. Two trained data collectors interviewed the study participants. Patient charts and medical records were reviewed for the respective information. We used a pill count method as well as medication administration charts for the assessment of drug adherence. If the patient has not received or not administered for less than 95% of his or her prescriptions for unjustified reasons, it will be recorded as “non-adherent.”21,22 Before entry to the Statistical Package for Social Sciences (SPSS) for analysis, data were cleared, categorized, compiled, and coded and also checked for completeness and accuracy. Any erroneous, ambiguous, and incomplete data were excluded. The data on DDIs identified were documented. pDDIs were categorized into different levels as follows.
Onset
Rapid. The effect of interaction occurs within 24 h of administration.
Delayed. The effect occurs if the interacting combination is administered for more than 24 h, that is, days to week(s).
Unspecified. The occurrence of the effect of interaction is not specified.
Severity
Major. There is risk of death and/or medical intervention is required to prevent or minimize serious negative outcomes.
Moderate. The effect of interaction can deteriorate patient’s condition and may require alteration of therapy.
Minor. Slight effects are produced that do not impair the therapeutic outcome.
Data processing and analysis
Data were entered into a computer using EpiData version 3.1 and exported to SPSS version 20.0 for analysis. Logistic regression analyses were used to assess the crude and adjusted effects of seemingly significant predictors of the target outcome. Variables that had a p-value ⩽ 0.25 on univariate analysis were eligible for multivariate logistic regression. All crude odds ratios (CORs) were reported through univariate logistic regression output and adjusted odds ratio (AOR) through multivariate logistic regression. Categorical and continuous data were expressed as percentages and mean ± standard deviations (SDs), respectively. Descriptive statistics were applied for the analysis of patient characteristics, including means, SDs, medians, and percentiles, and categorical variables were analyzed using the chi-square test. A p-value < 0.05 was considered to be statistically significant.
Ethical consideration
Ethical clearance and approval was obtained from the institutional review board (IRB) of Jimma University. The data collected from the JUMC medical wards were preceded by a formal request letter from Jimma University. Written informed consent was obtained from each study participant after clear orientation of the study objective. The raw data were not made available to anyone and not used as the determinant of the participant. All steps in data collection and compilation were conducted and supervised by the researchers. Strict confidentiality was assured through anonymous recording and coding of questionnaires and placed in a safe place. The patient had full right not to participate as well as leave the study at any time during the study.
Results
Medical and medication profiles of 200 hospitalized cardiac patients were evaluated during the study period in terms of pDDIs. Majority of the study participants were male 105 (52.50%), were at the age of ⩾56 years (77; 38.50%), were married (91; 45.50%), live and come from the urban area (107; 53.50%), and were unemployed (104; 52%) (Table 1).
Baseline sociodemographic characteristics of the study participants at medical wards of JUMC 2017.

JUMC: Jimma University Medical Center; SD: standard deviation; ETB: Ethiopian Birr.
Concerning the study participants’ behavioral habit, majority were non-smokers (122; 61%). About 94 (47%) were khat chewer and 58 (29%) were alcoholic. With regard to adherence to prescribed medications, among the study participants, about 89 (45.50%) patients were not fully adherent to their medication (Table 2).
Behavioral measures of study participants at medical wards of JUMC 2017.
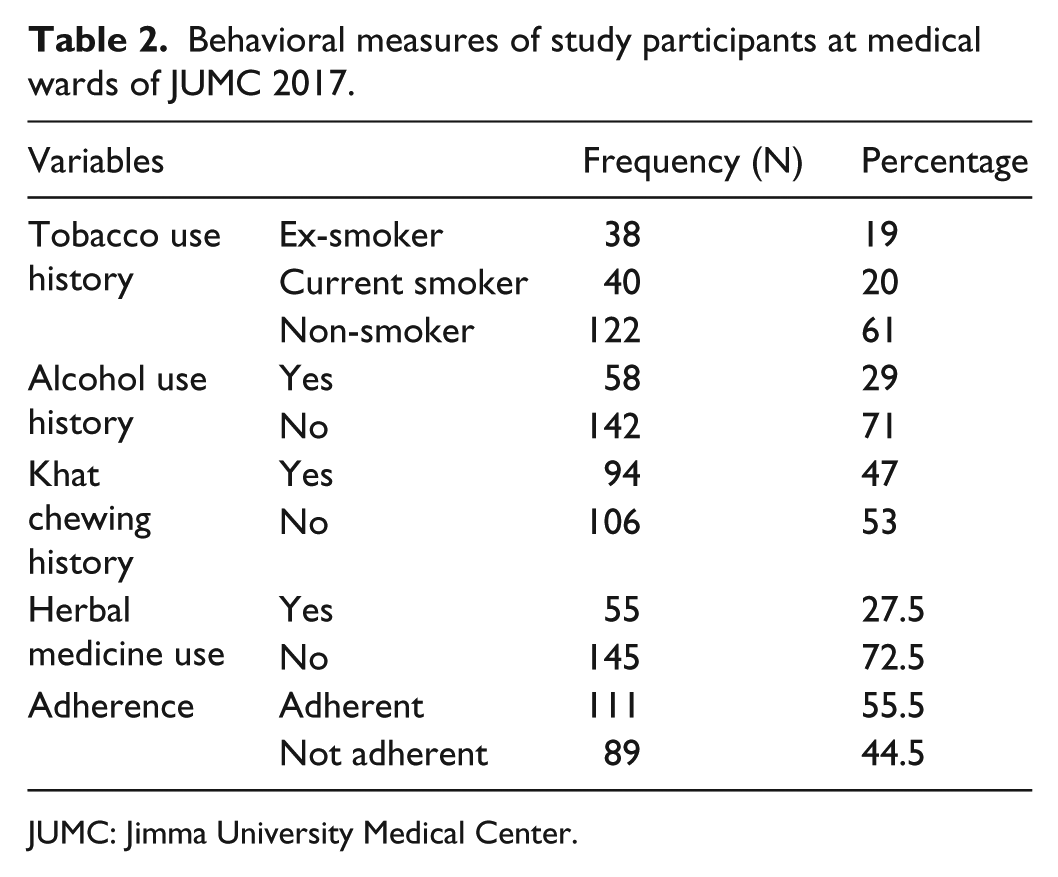
JUMC: Jimma University Medical Center.
In about 130 (43.92%) patients, comorbidities originated from infections, followed by hypertension (70; 23.65%) and atrial fibrillation (32; 10.81%). Around 53 (26.50%) study participants were diagnosed with one comorbid condition. The main causes of heart failure were ischemic heart disease accounting for 38.5%, followed by hypertensive heart disease (32.5%) and valvular heart disease (12.5%). The mean number of drugs prescribed per patient in the study population was 7.43 ± 3.86 (range 2–15). The mean duration of hospital stay of patients was 7.63 ± 4.66 (range 5–36) days (Table 3).
Baseline clinical characteristics of study participants at medical wards of JUMC 2017.

JUMC: Jimma University Medical Center; SD: standard deviation.
Community-acquired pneumonia and urinary tract infection;
Asthma, dyspepsia and renal disorders.
Hyperthyroidism and renal disorders.
Out of the 673 patients’ prescriptions analyzed, 521 prescriptions comprised potential drug interactions and it was found that 967 drug interactions were present. The prevalence rate of pDDIs among cardiac patients admitted to medical wards was 4.83 per patient and 1.44 per prescription regardless of the severity during their hospital stay.
Overall the prevalence rate of pDDIs was 74.41%. About 441 (45.0%) pDDIs were moderate and nearly one-third were major in severity. One-fourth of the pDDIs occurred due to PK interactions. About 496 (51.30%) were delayed in onset and above two-third resulted in cardiovascular system alterations. The risk of hemorrhage and toxicity will occur in up to 273 (28.23) prescriptions. Nearly in one-fourth of the prescriptions, multiple clinical effects will occur due to pDDI. With regard to pDDI management, in about 378 (39.10%) prescriptions, the use of alternative product is warranted. The need for dose adjustment and continued monitoring was for about 279 (28.85%) and 247 (25.54) prescriptions, respectively (Table 4).
Prevalence of potential drug–drug interactions among study participants at medical wards of JUMC 2017.

JUMC: Jimma University Medical Center; DDI: drug–drug interaction.
From the top 10 pDDIs, drug interaction between aspirin and furosemide occurred in about 173 (33.20%) prescriptions. Drug interaction between omeprazole and clopidogrel accounted for 75 (14.40%) prescriptions. About 288 (55.27%) prescriptions showed a major pDDI from the top 10 DDIs assessed during the study period (Table 5).
Top 10 major and moderate potential drug–drug interactions with their potential risks among study participants at medical wards of JUMC 2017.

JUMC: Jimma University Medical Center.
Associated factors for pDDIs
On the univariate analysis, older age was significantly associated to the occurrence of DDIs (COR (95% confidence interval (CI)): 1.21 (2.04–33.67), p = 0.027). The adjusted analysis also remained in the same direction (AOR (95% CI): 1.067 (2.33–27.12), p = 0.049), indicating older age as an independent predictor for pDDIs’ occurrence. Behavioral measures (i.e. being smoker, khat chewer, and alcoholic) was relatively associated with pDDIs’ occurrence. Long hospital stay (⩾7 days) was found to be a predictor for DDIs’ occurrence (AOR (95% CI): 2.80 (1.71–4.61), p = 0.024). Moreover, polypharmacy was significantly associated with pDDIs’ occurrence (COR (95% CI): 1.27 (0.62–2.51), p = 0.055) and it was an independent predictor for DDIs (AOR (95% CI): 1.64 (0.66–4.11), p = 0.041) (Table 6).
Factors associated with potential drug–drug interactions among study participants at medical wards of JUMC 2017.

JUMC: Jimma University Medical Center; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; pDDIs: potential drug–drug interactions.
Discussion
This study is the first of its kind to be carried out at JUMC inpatient medical wards. Potential drug interaction occurs when two drugs known to interact are concurrently prescribed, regardless of whether adverse events occur. In actual drug interaction, clinically meaningful alteration of the effect of an object drug occurs as a result of co-administration of another drug (precipitant drug). Potential drug interactions necessarily happen before actual drug interactions. 23
The importance of drug interactions in clinical practice primarily involves knowing or predicting those occasions when a potential interaction is likely to pose significant consequences for the patient. To predict the possible consequences of the administration of two or more drugs, health professionals should have practical knowledge of the pharmacological mechanism involved in drug interactions, drugs associated with great risk, and the most susceptible patient group. 24 Different strategies can be used to minimize the risks associated with potentially harmful drug combinations, such as reducing exposure to concurrent administration, using an alternative treatment, making a dosage adjustment, and monitoring the patient closely. 23
Drug interaction is one of the very important issues in drug therapy, especially in patients with multiple medical conditions, like patients with cardiovascular disorders. The study highlighted the overall prevalence rate of pDDIs (77.41%) from the combinations of the prescribed drugs. This is a high figure that highlights the importance of this previously unstudied problem in our hospital. Our study findings showed a higher prevalence of pDDIs as compared to reports from India (52.17%) among hospitalized patients, 25 South India (30.67%), 26 Pakistan (52%), 27 and Nepal (21.3%). 23 The reason for the higher prevalence of pDDIs in our study could be due to consideration of all grades of pDDIs; about two-fifth of our study populations were older patients and we follow the admitted cardiac patients throughout their hospital stay, which may increase drug interaction risks from multiple-drug exposure in inpatients.
In this study, pDDIs are classified on the basis of onset, severity, and evidence of occurrence. Based on the onset of pDDIs, 38.57% are rapid and 51.30% are delayed, and on the basis of severity about 32.68% of pDDIs were major and 45.60% and 21.72% were moderate and minor pDDIs, respectively. Therefore, minor types of pDDIs on the basis of severity and delayed types of pDDIs on the basis of onset were greater in number compared to the others. Delayed type of DDI could take up to several days or weeks to occur, without needing immediate concern or medical intervention. 28
Unlike this study, many other studies reported lower percentages of delayed onset pDDIs, ranging from 48.7% to 50%.29,30 But higher percentages of delayed onset pDDIs were reported from Iran (89.2%). 31 Therefore, even if there was an interaction occurring during the concomitant administration, it may not manifest itself immediately. If these combinations of drugs were to be continued on an outpatient basis, this could potentially lead to decreased efficacy, leading to therapeutic failures or potential for delayed adverse events. Hence, the duration of concomitant drug use should also be taken into account when prescribing relevant interacting drugs. In addition, the identification of these interactions at the time of discharge is important because the effect of an interaction may not appear until the patient has been transferred to another hospital unit. The greatest concern is that the effect will not appear until after hospital discharge. This situation highlights the importance of the medication reconciliation process for patient safety upon discharge from the hospital admission.
In this study, a higher number of observed pDDIs were due to PD mechanisms (59.36%) compared to PK type of interactions (25.34%). These findings differ from those reported from Nepal and by Sharma et al., 23 Vonbach et al., 32 and Aparasu et al. 33 The most common management plan found in this study for most of the drug interactions was using alternative medication and dose adjustment. Despite the importance of PD drug interaction in some scenarios (in synergism cases), it will pose clinically meaningful interactions. For example, the combination of angiotensin-converting enzyme (ACE) inhibitors with potassium-sparing diuretics such as amiloride or spironolactone can increase potassium retention so strongly that life-threatening hyperkalemia ensues. Therefore, patient-specific monitoring is the crucial step in clinical practice.
The mean age in this study was 42.54 ± 7.89 years. Majority (44%) of the patients in this study belonged to the age group ⩾ 55 years and also the pDDIs were widely seen in patients of the same age group. Our study showed similar data as those from South India, 34 but are in contrast with those from European countries.32,35,36 This can be explained by the fact that our study enrolled hospitalized patients, where elderly individuals were exposed to more multiple regimens than younger individuals, which in turn increases the risk of pDDIs.
The pDDIs are common in elderly patients during hospitalization. Hence, health professionals give priority to elderly patients, especially to those being treated with polypharmacy for chronic disease, taking drugs with a narrow therapeutic index, and taking drugs metabolized by enzymes susceptible to induction or inhibition. This is because they have the highest probability of experiencing pDDIs with their prescribed medications. Age-related physiological changes and altered PK and PD consequences place elderly patients at a high risk of pDDI-related adverse events. Therefore, by combining their knowledge and skills, health care providers should develop a comprehensive plan to enable the best pharmacotherapy while reducing the risks of drug interactions. 37
The average duration of hospital stay in this study was 7.43 ± 3.86 days. It was also seen that there is a relationship between increased prevalence of pDDIs in the population and the increased duration of stay. A chi-square analysis shows that patients who stayed longer than 7 days in hospital had significant pDDIs as compared to earlier discharged patients (p = 0.024). Available studies also have shown that the increased length of stay increases the probability of pDDIs’ occurrence.32,38,39 This might be because the chance of taking multiple drugs increases with longer stays in the hospital, which in turn increases the risk for pDDIs.
Polypharmacy is an important factor which leads to pDDIs; the more the number of items per prescription, the more the likelihood of pDDIs’ occurrence. This study also showed that the prevalence of pDDIs was associated with the number of drugs administered (p = 0.041). The prevalence of pDDIs in this study was about 59.5% in patients taking polypharmacy. Different studies showed that the number of medications has been shown to be a predictive factor for the occurrence of pDDIs at hospitals.40–42 Therefore, this study was in line with different scientific backgrounds in which hospitalized patients contract the likelihood of pDDIs due to severe and multiple illnesses, comorbid conditions, chronic therapeutic regimen, multiple medications, and frequent changes in drug therapy. This shows the importance of paying attention during the hospital stay through close medical monitoring combined with continuous nursing and pharmaceutical care.
Health care providers should be more aware of pDDIs and should collaborate to develop educational programs and improve patients’ counseling to avoid/reduce improper use of medications. Our recommendation is to pay more attention for patient’s medication list before considering this combination as desirable or undesirable drug interaction.
The limitation of this study is that the sampling method was convenient and the small number of participants which limits the ability to make broader generalizations from the results. Also, the Micromedex drug interaction checker used in this study did not take into consideration the prescribed dose, frequency of administration, and route of administration. However, our study revealed the magnitude of pDDIs among admitted cardiac patients and the need to take proactive measures to reduce these additional burdens on our patients.
Conclusion
This study demonstrated a high prevalence of pDDIs among hospitalized cardiac patients in medical wards due to the complexity of pharmacotherapy. The prevalence rate is directly related to age, number of prescribed drugs, length of hospital stay, history of tobacco use, and khat chewing. PD DDI was the common mechanism of pDDIs. Older age, long hospital stay, and polypharmacy were independent predictors for the occurrence of pDDIs. Therefore, development and implementation of cautionary guidelines and computer-based screening could help physicians and pharmacists to prevent potentially dangerous drug interactions in order to avoid harmful effects on patients.
Footnotes
Acknowledgements
We would like to express our heartfelt gratitude to the Institute of Health sciences, Jimma University, for giving us the chance to conduct this research. Our acknowledgment extends to all the study participants for their time and willingness to respond and to data collectors and the supervisor for their friendly work.
Author contributions
The analysis was conceptualized by N.D., T.M., D.A., and A.T. Data collection was managed by N.D. and T.M. and data analysis was conducted by N.D. and T.M. with support from D.A. and A.T. T.M. drafted the manuscript. All authors participated in editing, feedback, and revisions of the manuscript.
Availability of data and materials
The data sets generated during and/or analyzed in this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the institutional review board of Jimma University (no. 173/2017).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Jimma University, Ethiopia.
Informed consent
Written informed consent was obtained from all subjects before the start of the study.