
Abstract
Objectives:
The prevalence of non-AIDS-related comorbidities is increasing in HIV-infected patients receiving antiretroviral therapy. In Thailand, data regarding the prevalence of non-AIDS comorbidities and factors associated with metabolic complications in HIV-infected patients have not been well-documented.
Methods:
This cross-sectional study was conducted in 2011 and included 874 HIV-infected patients.
Results:
The age of patients was 45(8) years represented as mean (standard deviation [SD]). The current CD4 count was 502(247) cells/mm3. In all, 388 (44%) of the included patients had at least 1non-AIDS comorbidity. The most frequently documented comorbidities were hyperlipidemia in 271 (70%) patients. Using multivariate analysis, older age(odds ratio [OR] = 1.82, 95% confidence interval [CI] = 1.51-2.19), male sex (OR = 1.55, 95%CI = 1.14-2.11), high current CD4 count(OR = 1.00, 95%CI = 1.00-1.00), and taking abacavir (ABC)-containing(OR = 2.59, 95%CI = 1.16-5.78)and didanosine (ddI)-containing antiretroviral regimens (OR = 4.16, 95%CI = 1.09-15.84)were associated with the presence of metabolic complications (all Ps<.05).
Conclusion:
The prevalence of comorbidities is substantially high. Clinical monitoring and effective management of these comorbidities and metabolic complications are recommended, especially in HIV-infected patients who present with these associated factors.
Introduction
In 2013, the reported prevalence of HIV-infected patients in the adult Thai population was 1.1%. 1 Currently, HIV infection is a chronic but manageable disease. All HIV-infected patients require long-term effective antiretroviral treatment. Thailand is a middle-income country that produces affordable generic antiretroviral drugs. Most patients, therefore, have access to antiretroviral therapies. 2 Such patients not only live longer but also experience long-term toxicities that result from antiretroviral drugs along with HIV-related comorbidities. 3,4
The existing literature shows that non-AIDS-related comorbidities are increasing. These include cardiovascular disease, metabolic syndrome, renal and bone diseases, cancer, and neurocognitive impairment. 5,6 Such comorbidities are more prevalent among HIV-infected patients compared to the general population. 5,6 In developing countries, a systematic review of the epidemiology of comorbidities in HIV/AIDS and noncommunicable diseases found that more than one-third of HIV-infected patients had an underlying cardiovascular disorder. The reported prevalence of metabolic syndrome ranges from 11% to 28% in HIV-infected patients. 7 In addition, some studies have reported a slightly increased prevalence of metabolic syndrome. 7,8 Age is one of the major risk factors for non-AIDS-related comorbidities. Other risk factors include a low immune status, the duration of antiretroviral drug exposure, the use of injected drugs, male gender, and specific drug regimens. 5,6,9,10 This is a cross-sectional study with the objective of describing (1) the prevalence of non-AIDS comorbidities and (2) the factors associated with metabolic complications among Thai HIV-infected patients.
Methods
Selection and Description of Participants
A cross-sectional study was conducted at the Bamrasnaradura Infectious Diseases Institute, Ministry of Public Health, Nonthaburi, Thailand. This institute is a 300-bed tertiary HIV referral center located directly northwest of Bangkok. The institutional ethics committee of the Bamrasnaradura Infectious Disease Institute reviewed and approved the study. Inclusion criteria were as follows: (1) HIV-infected patients who were aged 18 years or older and (2) HIV-infected patients who had received HIV care at the Bamrasnaradura Infectious Disease Institute in 2011.
Data Collection
All patients’ identification numbers were obtained from the annual database of the institute. The data were extracted from medical records.International Classification of Diseases, Tenth Revision(ICD-10) diagnostic code was used to identify comorbid conditions in the Bamrasnaradura Infectious Disease Institute electronic database. All data were retrieved, including baseline demographics, clinical characteristics, and antiretroviral drug regimens. The metabolic comorbidities in the study included hyperlipidemia, hypertension, diabetes mellitus, and impaired fasting glucose. Viral hepatitis coinfections included hepatitis B and hepatitis C. Neurological diseases included stroke, Parkinson disease, epilepsy, and dementia. Cardiovascular diseases included congestive heart failure, myocardial infarction, and cardiomyopathy. Thyroid diseases included hyperthyroid, hypothyroid, thyrotoxicosis, and nontoxic thyroid nodules.
Statistical Analysis
Means (standard deviation, SD) and frequencies (%) were used to describe patients’ baseline characteristics and the prevalence of comorbidities. Gender, antiretroviral drug regimens, and comorbidities were classified as categorical variables. Age, CD4 counts, plasma HIV-RNA levels, and the duration of receiving antiretroviral drugs were treated as continuous variables. Logistic regression was used to assess the association between metabolic complications and interesting potential variables. The odds ratio (OR) and its 95% confidence interval were estimated. In this study, the logistic regression analyses showed that data using “antiretroviral drug regimen” and “each antiretroviral drug” were independent variables. In univariate analyses, any variables with a P value <.1 were included in the multivariate analyses. Variables were found to be significant at P value < 0.05. All analyses were performed using SPSS version 15.0.
Results
The study involved 874 patients. The mean age of the patients was 45(8) years, and 502 (57%) participants were male. CD4 counts were 502(247) cells/mm3, and 853 (97%) of the patients had plasma HIV-RNA levels <40 copies/mL. Patients’ baseline characteristics are summarized in Table 1. Of the 874 patients, 388 (44%) had comorbidities. The number of comorbidities and the number of comorbidities stratified by age are shown in Figure1A and B, respectively. Of all the patients, 347 (89%) had metabolic complications, including hyperlipidemia in 271 (70%) patients, hypertension in 106 (27%) patients, diabetes mellitus in 93 (24%) patients, and impaired fasting glucose in 31 (8.0%) patients. The prevalence of each individual comorbidity is presented in Table 2.
Baseline Characteristics of 874 HIV-Infected Patients.
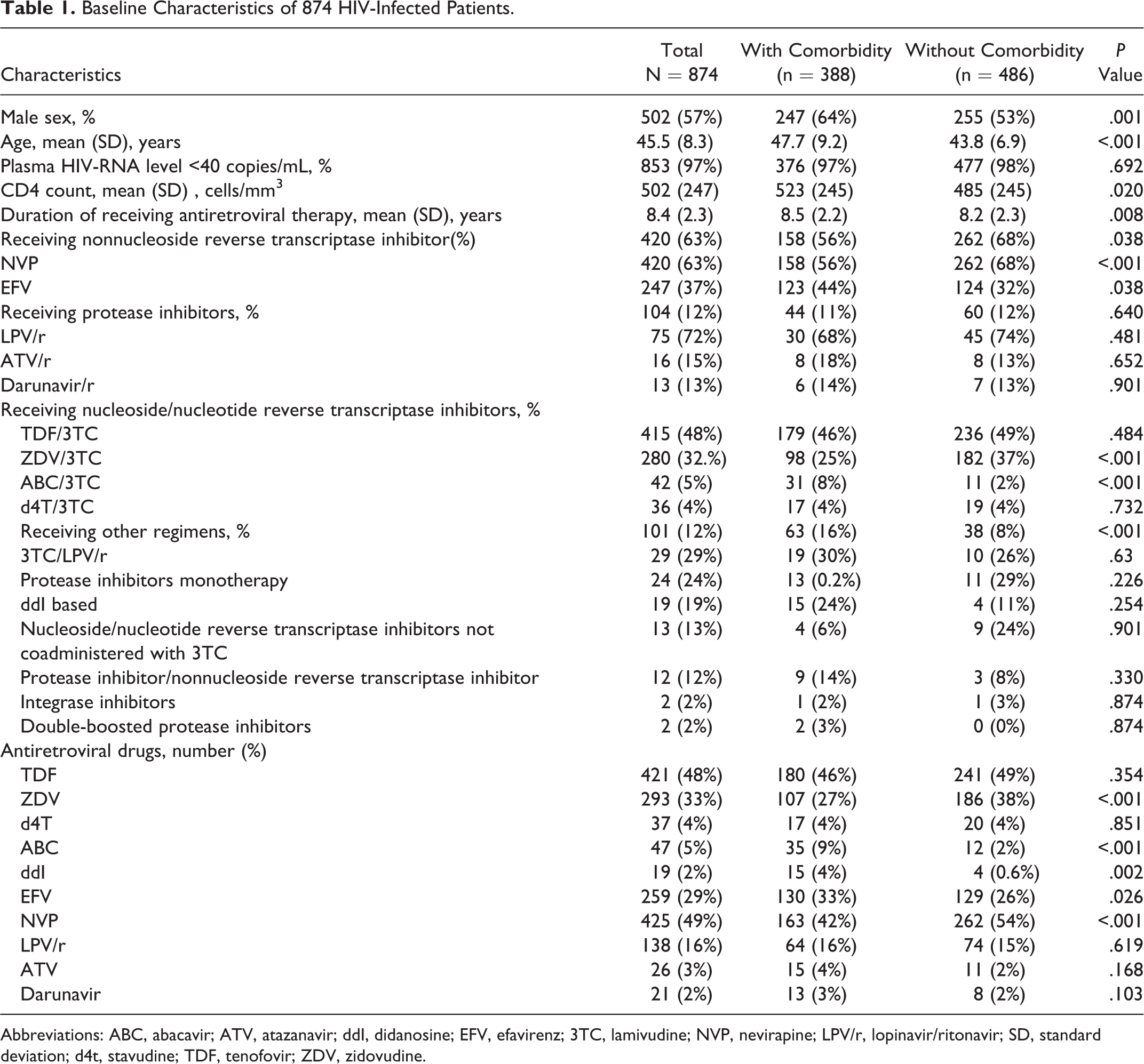
Abbreviations: ABC, abacavir; ATV, atazanavir; ddI, didanosine; EFV, efavirenz; 3TC, lamivudine; NVP, nevirapine; LPV/r, lopinavir/ritonavir; SD, standard deviation; d4t, stavudine; TDF, tenofovir; ZDV, zidovudine.

The Prevalence of Individual Comorbidities.

The multivariate analyses of factors associated with metabolic complications are shown in Tables 3 and 4. The analyses showed that abacavir (ABC)/lamivudine (3TC)-containing regimens (OR = 3.05), age (increasing in 10-year intervals; OR = 1.84), male gender (OR = 1.53), and current CD4 count (OR = 1.00) were associated with an increase in the metabolic complications in HIV-infected patients. Nevirapine (NVP; OR = 0.67)-containing regimens were found to provide a protective effect. For individual antiretroviral drugs, the analysis showed that didanosine(ddI; OR = 4.16), ABC(OR = 2.59), male gender (OR = 1.55), age (increasing in 10-year intervals; OR = 1.82), and current CD4 count (OR = 1.00) were associated with increasing metabolic complications.
Univariate and Multivariate Analysis of Factors Associated with “Metabolic Complications.”a

Abbreviations: ABC, abacavir; ART, antiretroviral therapy; CI, confidence interval; 3TC, lamivudine; NVP, nevirapine; OR, odds ratio; ZDV, zidovudine.
aAdjusted association of metabolic complications with age (increasing every 10 years), gender, current CD4 count, duration of receiving antiretroviral drug, and antiretroviral drug regimen. Antiretrovial drug means individual antiretroviral drugs. Antiretroviral drug regimen means the ARV regimen that consists of antiretroviral drug that we want to see the association.
Univariate and Multivariate Analysis of Factors Associated with “Metabolic Complications.”a

Abbreviations: ABC, abacavir; ART, antiretroviral therapy; CI, confidence interval; ddI, didanosine; EFV, efavirenz; NVP, nevirapine; OR, odds ratio; ZDV, zidovudine.
aAdjusted association of metabolic complications with age (increasing every 10 years), gender, current CD4 count, duration of receiving antiretroviral drug, and antiretroviral drug regimen. Antiretrovial drug means individual antiretroviral drugs. Antiretroviral drug regimen means the ARV regimen that consists of antiretroviral drug that we want to see the association.
Discussion
The present study demonstrates that almost half of the HIV-infected patients had at least 1comorbidity. The same trend was found in a retrospective study conducted in 2007 to 2008 in Nigeria, which showed that 36% of HIV-infected patients had at least 1comorbidity. 11 This figure is considered to be high; therefore, medical management of HIV that addresses comorbidities is necessary.The most prevalent comorbidities in this study were metabolic complications, including hyperlipidemia, hypertension, and diabetes mellitus. This finding corresponds to the findings of a previous cross-sectional study, which showed a high prevalence for hyperlipidemia among Thai HIV-infected patients. 12 Hypertension and hyperlipidemia have also been documented as common comorbidities in Asian and Caucasian populations. 10,13,14,15 Between 2000 and 2012, a systematic review of the epidemiology of comorbidities in developing countries found that cardiovascular diseases accounted for more than one-third of HIV-infected patients. However, the prevalence of diabetes mellitus was low compared to the results of the current study. 7 Studies in South Africa and Nigeria found high prevalence of hypertension but a low prevalence of hyperlipidemia. 9,11 A retrospective case–control study in Taiwan showed that 20% of patients had hyperglycemia and 10% of those had diabetes. 16 Differences in lifestyle, drug regimens (including antiretroviral regimens and patients’ co-administration of drugs for clarification), economic status, and the presence or absence of national health policies may be factors that contribute to the discord in results between studies. With regard to neuropsychiatric events, a cross-sectional study among Thais in 2004 found that 37% of them displayed neurocognitive impairments. This is in contrast to our study, which found a low prevalence. 17 Two cross-sectional studies in Brazil and Canada found that mental health problems had the highest comorbidity prevalence. 6,18 Underestimation may be an explanation as to why our study showed a low prevalence of neurocognitive impairments and mental health problems.
In terms of associated factors, this study shows that every 10-year increase in age was associated with a 1.8-fold risk of having metabolic complications. Older adults had a higher chance of having comorbidities compared to younger adults, which is consistent with other studies. 5,6,10,15,18 A study in the Unites States showed that male gender was a risk factor for metabolic complications. 13 Protease inhibitor-containing regimens were a risk factor for comorbidities in previous studies in the Unites States and the Netherlands. 5,13 Antiretroviral drugs have both positive and negative effects, and they are associated with an increased risk of metabolic complications such as cardiovascular disease, insulin resistance, and dyslipidemia. A meta-analysis showed that specific protease inhibitors and ABC were associated with myocardial infarction. 8,19 Using ddI, stavudine (d4T), efavirenz (EFV), lopinavir/ritonavir(LPV/r), or zidovudine (ZDV) were associated with dyslipidemia and diabetes mellitus. 8 Both ABC and ddI were, in our study, associated with metabolic complications. Our study showed no association between using protease inhibitors and metabolic complications. This finding may be explained by the low number of patients in the study who received protease inhibitors. One explanation for ABC being a risk factor for metabolic complications but not myocardial infarction is that physicians might choose ABC for patients with chronic diseases prior to administering antiretroviral drugs. The NVP is well tolerated, and this study also found that NVP provides a protective effect.
The prevalence of dyslipidemia in Thailand was studied in 2009, and 47%, 38%, and 29% of the patients had low high-density lipoprotein cholesterol, high triglycerides, or high low-density lipoprotein cholesterol, respectively. 20 The prevalence of diabetes mellitus and hypertension were approximately 9.6% and 22%, respectively, in 2003 and 2004. 21,22 This study showed a higher prevalence of dyslipidemia, diabetes mellitus, and hypertension in HIV-infected patients than in the general population. The same trend was found in the cross-sectional studies in Canada and the Netherlands, showing that HIV-infected patients displayed a higher prevalence of comorbidities than the general population. 5,6 The reason for this may be that HIV-infected patients express higher levels of markers of systemic inflammation and coagulation than the general population, and this may be a side effect of antiretroviral drug use. 5
There are several limitations in our study. First, uninfected HIV patients were not used for comparison. Second, data for some associated factors, such as smoking, BMI, and illegal drug use, were not available. Third, some laboratory measurements were also missing, such as lipid parameters and fasting blood glucose. Fourth, we retrieved the data for ICD-10 diagnostic codes from a hospital database. Thus, some patients in our study were not screened for each comorbidity, and some comorbidities were not recorded with an ICD-10 diagnostic code.
The prevalence of non-AIDS comorbidities, particularly metabolic complications, is high in a middle-income country.Therefore, a comprehensive approach to managing such complications should be used when treating HIV-infected patients to achieve long-term survival.
Footnotes
Acknowledgments
The authors would like to thank the staff of the Bamrasnaradura Infectious Diseases Institute for their cooperation in data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.