
Abstract
Objectives:
Little is known about the dynamics of condom use among female sex workers (FSWs) in Iran. We investigated the correlates of consistent condom use (CCU) among FSWs, using data from a national biobehavioral surveillance survey in 2010.
Methods:
A total of 872 FSWs were recruited using a facility-based sampling strategy from 21 sites in 13 cities in Iran. Data were collected through face-to-face interviews using a standardized questionnaire.
Results:
Overall, 33.6% and 17.3% of FSWs reported CCU with paying and nonpaying sex partners, respectively. Consistent condom use with paying partners was significantly associated with temporary marriage, accessing family planning services and history of working in brothels. Conversely, temporary marriage or married status, condom rupture/slippage, and HIV seropositivity remained independently significantly associated with CCU with nonpaying sex partners.
Conclusion:
Our findings indicated the urgent need for scaling up condom promotion interventions catered toward FSWs and their sex partners to practice safe sex consistently.
Introduction
The HIV epidemic in Iran affects subpopulations of people who inject drugs (PWIDs), prisoners, sexual partners of PWIDs, and female sex workers (FSWs). Although the epidemic continues to be driven by unsafe injection, the rate of sexual transmission of HIV has been constantly increasing and around 34% of the identified cases have been infected through unprotected sex. 1 –3 In Iran, FSWs have recently been acknowledged as a subpopulation most at risk of HIV—with an HIV prevalence of 4.5% in 2010—and have been provided with targeted harm reduction services. 4 –7 Fueled by the profound stigmatization and illegal nature of sex work, 8 the epidemiology of HIV and risky behaviors among FSWs are not yet fully studied in Iran. 9
Although our understanding of condom use practices within this population is still limited in Iran, some of the barriers to condom use practices among FSWs are low self-efficacy, limited condom negotiation skills, and low perceived risk of HIV infection. 10,11 The existing body of evidence that suffers from several sampling biases suggests around 70% to 75% of FSWs have reported condom use in their last sexual encounter. 12 –15 Nonetheless, little is known about consistent condom use (CCU) practices among FSWs in Iran as well as factors associated with it.
As consistent and correct use of condoms has been proven to be an effective strategy in preventing HIV transmission, understanding its correlates among FSWs in Iran is important. Therefore, using data from the first national biobehavioral surveillance survey conducted in 2010, we aimed to identify the correlates of CCU with an eye for FSWs’ different sexual practices with paying and nonpaying sex partners. Our findings could inform policies and provide valuable insight into the design and implementation of prevention and harm reduction interventions catered toward FSWs in Iran.
Methods
Study Design and Data Collection
Data were obtained from the first national biobehavioral surveillance survey among FSWs in Iran conducted between April and July 2010. Details of methodology and sampling strategies of the survey are described elsewhere. 16 –18 In brief, participants were recruited from 21 sites in 14 cities by trained interviewers from a geographically representative sample of FSWs. The recruiting sites included specific centers catered toward vulnerable women (ie, FSWs, partners of PWIDs, and women who inject drugs). Facilities were selected based on the presumed level of HIV prevalence in FSWs and input from the local HIV experts on facilities’ logistical and capacity constraints.
A convenience sample of 30 to 45 eligible FSWs was recruited at each site. Inclusion criteria were (1) women aged ≥18 years; (2) women who had sold sex for money, drugs, or goods in the past 12 months preceding the survey; and (3) women who had a history of practicing sex work for at least 6 months. Female sex workers were approached by a trained interviewer who verified their eligibility criteria and collected data using a standardized pilot-tested risk assessment questionnaire. We initially approached 1005 FSWs; the entire data set from 1 province (N = 100) was excluded mainly due to the low-quality data collection and not following our protocol. From the remaining 13 provinces, 32 FSWs were excluded because of ineligibility and 1 because of refusal to give consent (final analytic sample = 872). Data were collected on participants’ demographics, sexual and reproductive health history, knowledge of HIV prevention, sexually transmitted infections (STIs), and risky behaviors.
Dependent Variables
The current analysis explores the correlates of recent CCU with paying and nonpaying sex partners among FSWs in Iran. Consistent condom use was treated as a binary variable. Respondents were asked “Have you been using condoms consistently with your paying/nonpaying sex partners in the past month?” and the responses were coded as always and otherwise. The “otherwise” category was a pooled category of other responses in our sample including often, sometimes, and never.
Independent Variables
Sociodemographic variables examined included age (≤24 or >24), marital status (single, married, temporary marriage, or widow/divorced), education (no schooling, primary school, guidance school, high school, or university degree), having children (yes or no), and sufficient knowledge of sexual transmission of HIV (yes or no). Sexual-related correlates included condom rupture/slippage in the past month (yes or no), history of STIs (yes or no), multiple sex partners in the past month (yes or no), history of abortion (yes or no), history of accessing family planning services (yes or no), history of receiving free condoms from HIV prevention services (yes or no), condom accessibility in the past month (≤1 hour or >1 hour), and history of working in a brothel (yes or no). Data were also collected on other independent variables including history of having an HIV test result (yes or no), self-perceived risk of HIV (yes or no), HIV serostatus (positive or negative), sex under the influence of substances (ie, illicit drugs or alcohol) in the past month (yes or no), daily drug use in the past month (yes or no), and history of illicit drug injection (yes or no).
Data Analysis
Frequencies and descriptive statistics were computed for all main outcomes. Two predictive logistic regression models were constructed to investigate the correlates of CCU with paying and nonpaying sex partners. Crude and adjusted odds ratios (AORs), as well as 95% confidence intervals (95% CI), were reported. Variables with a P value <0.2 in the bivariable analysis were entered into the multivariable regression model. The final analytic sample for regression analyses included 606 and 392 participants who provided valid responses to CCU with paying and nonpaying sex partner variables, respectively. Survey package of Stata version 11 (Stata Corp) was used throughout the analysis.
Results
Descriptive statistics of FSWs stratified by the type of sexual partner are presented in Table 1. Median (Q1, Q3) age of the participants was 30 (25, 37). A total of 33.6% (95% CI: 24.7-43.9) and 17.3% (95% CI: 12.3-23.9) reported CCU with paying and nonpaying sex partners, respectively. Although participants reported different sources for obtaining condoms, only 6.0%, 43.7%, and 6.5% reported obtaining condoms from family planning centers, drop-in centers, and peer outreach, respectively. Conversely, pharmacies (52.1%) were cited as the most common place for obtaining condoms. A total of 531 (63.1%) FSWs reported protected sex with their last paying sex partner; condom use was suggested by clients in only 16.6% of the time. Similarly, among the 172 (37.0%) FSWs who reported protected sex with their last nonpaying sex partner, condom use was suggested by sex partners in only 12.2% of the time. Moreover, while partner refusal (37.6%) was reported as the main reason for not using condoms in their last paid sex, FSWs reported using nonbarrier contraceptive methods (31.0%) as the main reason for not using condoms in their last nonpaid sex.
Consistent Condom Use Stratified by Partner Type among Female Sex Workers in Iran.
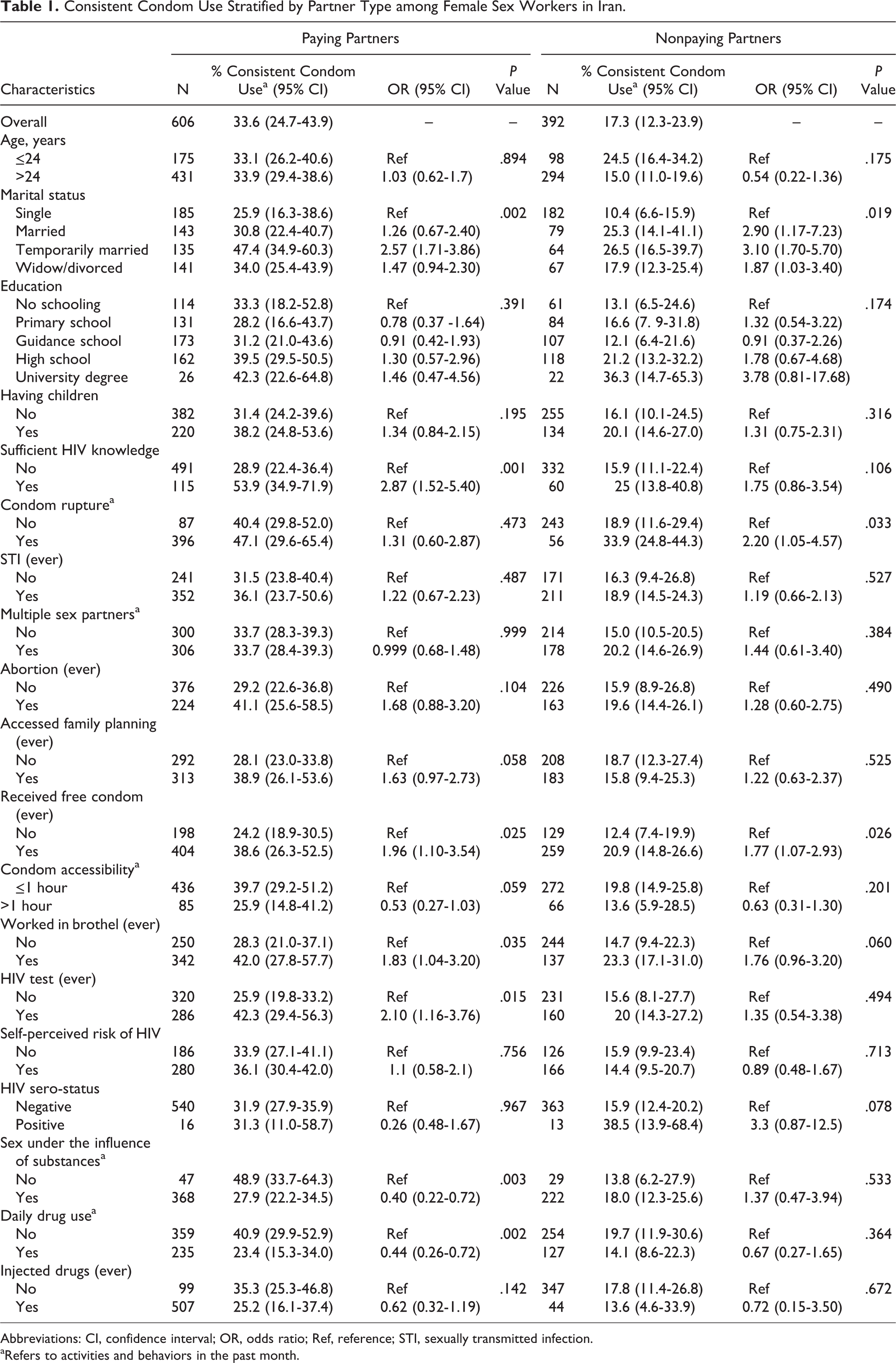
Abbreviations: CI, confidence interval; OR, odds ratio; Ref, reference; STI, sexually transmitted infection.
aRefers to activities and behaviors in the past month.
Overall, higher prevalence of CCU with paying sex partners was reported among FSWs who were in temporary marital relationships (odds ratio [OR] = 2.57; 95% CI: 1.71-3.86), had sufficient knowledge of sexual transmission of HIV (OR = 2.87; 95% CI: 1.52-5.40), had accessed family planning services (OR = 1.63; 95% CI: 0.97-2.73), had received free condoms from prevention services (OR = 1.96; 95% CI: 1.10-3.54), had ever worked in brothels (OR = 1.83; 95% CI: 1.04-3.20), and had ever tested for HIV (OR = 2.10; 95% CI: 1.16-3.76). Moreover, lower prevalence of CCU with paying sex partners was reported among FSWs who could not access condoms in less than 1 hour (OR = 0.53; 95% CI: 0.27-1.03), were under the influence of substances before sex (OR = 0.40; 95% CI: 0.22-0.72), and were using drugs daily in the past month (OR = 0.44; 95% CI: 0.26-0.72). Conversely, higher prevalence of CCU with nonpaying sex partners was reported among FSWs who were in temporary marital relationships (OR = 3.10; 95% CI: 1.70-5.70), reported condom rupture/slippage (OR = 2.20; 95% CI: 1.05-4.57), and had received free condoms from prevention services (OR = 1.77; 95% CI: 1.07-2.93).
The results of the multivariable analyses are presented in Table 2. In the multivariable logistic regression model for paying sex partners, temporary marriage (adjusted OR [AOR] = 2.65; 95% CI: 1.65-4.24), accessing family planning services (AOR = 1.75; 95% CI: 1.08-2.86), and history of working in brothels (AOR = 1.73; 95% CI: 1.02-3.00) remained independently significantly associated with CCU. On the other hand, temporary marriage (AOR = 2.22; 95% CI: 1.12-4.39) or married status (AOR = 3.25; 95% CI: 1.38-7.65), condom rupture/slippage (AOR = 2.05; 95% CI: 1.19-3.54), and HIV seropositivity (AOR = 5.07; 95% CI: 1.19-21.62) remained independently significantly associated with CCU with nonpaying sex partners.
Correlates of Consistent Condom Use with Paying and Nonpaying Sex Partners among Female Sex Workers in Iran.
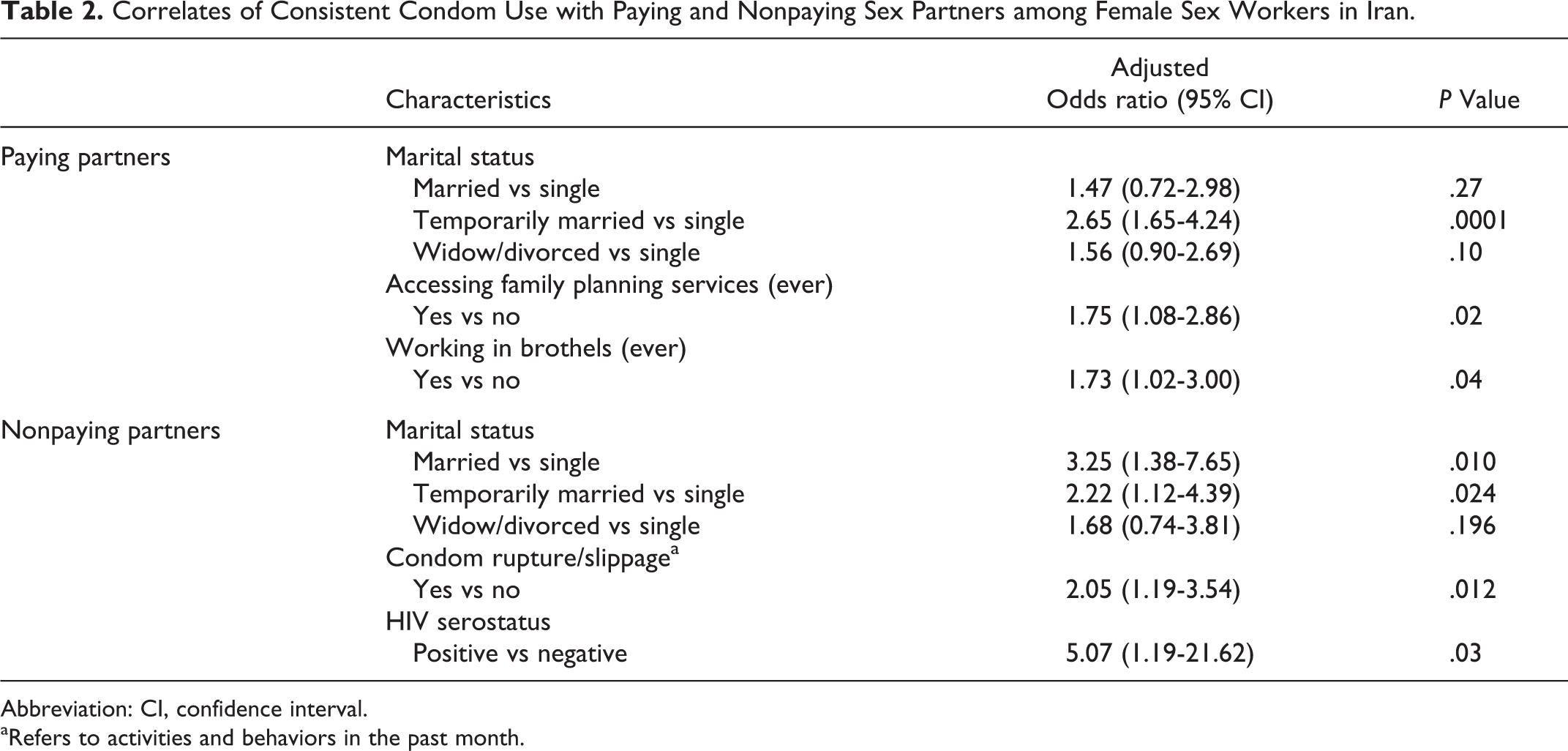
Abbreviation: CI, confidence interval.
aRefers to activities and behaviors in the past month.
Discussion
In our analysis of a national survey of FSWs in Iran, we found that only one-third of FSWs had consistently used condoms with their paying sex partners and less than one-fifth had consistently used condoms with their nonpaying sex partners in the past month. Consistent condom use with paying partners was associated with being temporarily or permanently married, having accessed family planning services, and history of working in brothels. Conversely, CCU with nonpaying sex partners was associated with being temporarily married, reporting a history of condom rupture/slippage and HIV seropositivity. Our findings are comparable to an existing body of evidence pointing to a significantly higher rate of recent condom use (ie, last sex) among FSWs in Iran (around 70%) and suggest that CCU is considerably lower than condom use at the last sexual encounter. 12,14,15,19
Reported condom use with nonpaying sex partners was significantly lower than that with paying sex partners. This implies an elevated risk of infection among nonpaying partners of FSWs that could bridge HIV/STIs to the general population. 20,21 Indeed, this is a relatively common finding in studies across other contexts. For example, studies in India, Senegal, Uzbekistan, and Congo suggest significantly higher rates of CCU with commercial partners compared to noncommercial ones. 22 –25 This could be due to the affection and trust involved in FSWs’ intimate relationships—where condom use is perceived as a symbol of unfaithfulness which raises mistrust—or their reduced perception of risk of HIV transmission with their intimate partners. 22 –25 Moreover, studies among FSWs have associated nonbarrier modern contraception methods with reduced condom use, reflecting on a perceived decreased need for using barrier methods (ie, condom). 26 –28 Female sex workers citing the use of nonbarrier modern contraception methods as the main reason for not using condoms with their nonpaying sex partners suggests that the main motivation behind condom use with nonpaying sex partners may be the avoidance of unwanted pregnancies and not protection against HIV/STIs.
On the other hand, rates of CCU with paying sex partners were fairly low (33.6%), which could stem from FSWs’ lack of condom negotiation and their paying partners’ refusal to use condoms. 22,29 Poor safe sex negotiation skills with clients have been reported as a factor that influences FSWs condom use and safe sex practices across various settings, despite their acknowledgment of the primacy of HIV risks associated with sex work. 22,24,26,30 This is in line with our finding that partner refusal was reported as the main reason for noncondom use, and paying sex partners had proposed to have protected sex in only 16% of the time. Additionally, the fact that less than 7% of FSWs reported obtaining condoms from peer groups points to the missed potential of employing peer-based interventions for FSWs. 31
Furthermore, married FSWs reported higher CCU with both paying and nonpaying sex partners, which is consistent with the findings of a study in Central Asia (ie, Uzbekistan) that reports married women to be more likely to use condoms consistently. This could be due to married FSWs’ concern about infecting their intimate partners, particularly in settings where involving in sex work is highly stigmatized and/or they are involved in sex work without their spouse’s knowledge. 24 Female sex workers’ concern about infecting their nonpaying sex partners might also partly explain the very high odds of CCU among HIV-seropositive FSWs in our study; however, any interpretation should be made with caution due to the cross-sectional design of the survey and given that data on FSWs’ knowledge of their HIV status were not collected in the study.
Additionally, a history of working in brothels and accessing family planning services—one of the main reasons for FSWs’ referrals to harm reduction services 5 —were significantly associated with higher rates of CCU with paying partners. The former association could be attributed to the regulations in place within brothels that often requires clients to use condoms. The latter, however, could point to the important role that family planning services could play in improving safe sex practices among FSWs. Nonetheless, despite the fact that family planning services targeting FSWs are not significantly affected by Iran’s recent shift in population control policies, 32,33 less than half of the FSWs reported not having ever received family planning services (eg, STI counselling, free condoms). This calls for further research on barriers to accessing the existing services and ways to make them more visible to FSWs.
Our study has several limitations that warrant discussion. The data presented here were collected in 2010 and may not completely reflect current practices of FSWs in Iran; however, publishing our findings was not feasible, considering the sensitivities around this issue. Similar to all studies with voluntary participants and self-reported data, our findings are prone to selection bias, social desirability bias, and recall bias. Our findings may also not be generalizable to all FSWs living in Iran as we recruited participants from facilities where we chose for data collection. Moreover, we did not collect data on gender identity, violence, or coercion into sex work, which have been shown to play an important role in shaping condom use practices among FSWs. 34 –37 Nonetheless, while achieving a gold-standard survey methodology to provide a representative sample of FSWs in Iran continues to be a challenging practice, efforts were made to reduce potential biases by engaging local organizations and staff as well as experienced interviewers.
Conclusion
Considering the limited available data on FSWs in Iran, findings of this survey could serve as a basis for tracking and monitoring the risky sexual behaviors of FSWs and guiding policy makers in developing strategies to optimize the service provisions for FSWs in Iran. Collectively, our findings indicate the importance of reemphasizing consistent and correct safe sex practices for FSWs. Although the reproductive health needs of FSWs continue to be unmet in Iran, 17 further efforts should be made to improve FSWs’ risk perception of HIV, safe sex negotiation skills, and access to prevention services. Developing studies to reach paying and nonpaying sex partners of FSWs is an urgent priority; populations who are currently overlooked in surveillance services in Iran but have a key role in increasing safe sex practices among FSWs.
Footnotes
Acknowledgments
The authors are grateful to the participants for their time. Our gratitude also goes to the provincial supervisors who helped with data collection.
Declaration of Conflicting Interests
The author(s) declared a potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Abbas Sedaghat has been actively involved in HIV policy planning in Iran and is supported by the Ministry of Health. The rest of the authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey was financially supported by the Global Fund to fight AIDS, Tuberculosis and Malaria and the Ministry of Health of Iran in 2010. However, the authors received no funding for this specific paper.
Ethical Consideration
Ethical issues in our study included the guarantee of the participants’ confidentiality and verbal consent. Participants were briefed about the purpose of the survey, their voluntary participation, the incentives, and the anonymity of all collected data. Participants’ refusal to take part in the study did not interfere with or impact the services or treatment provided to them. The ethics committee of the Kerman University of Medical Sciences reviewed and approved the study protocol (2010—no 90/122).