
Abstract
Background:
There is a growing number of new Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome infections in Ghana despite the implementation of condom utilisation campaigns. Attitudes toward the use of condoms are culturally dependent, but most condom use attitude studies ignore this. Obstacles such as embarrassment to purchase or inability to negotiate use are due to Ghana’s strong adversarial cultural norms against condom use.
Method:
From February 2025 to April 2025, an institution-based cross-sectional study was carried out using a systematic sampling approach to select 1748 seropositive heterosexual participants from four regions of Ghana. The study utilised the University of Chicago Los Angeles Multidimensional Condom Attitudes Scale as the instrument for data collection. Condom use attitudes were evaluated based on the mean scores of the five psychometric properties of the scale. Multivariable logistic regression established the associations between dependent and independent variables. Outcome variables with a p-value < 0.05 were deemed statistically significant. The odds ratio with a 95% confidence interval was computed to determine the strength of an association.
Results:
Despite more than half of the respondents having positive condom use attitudes (n = 884; 50.6%), the majority (n = 1171; 67%) of respondents engaged in unprotected sex. While few participants in the Ashanti Region (n = 120; 27.1%) and Bono Region (n = 150; 34.4%) had a positive condom use attitude, the majority of participants in the Volta Region (n = 336; 77.6%) and Central Regions (n = 278; 63.3%) had a positive condom use attitude. Based on the means, perceived embarrassment about condom negotiation and use was high in the Ashanti Region (4.87 ± 1.12), Bono Region (4.68 ± 1.18), Central Region (4.41 ± 1.64), except the Volta Region (3.98 ± 1.38). Perceived embarrassment about condom purchase was high in the Ashanti Region (4.43 ± 1.10), Bono Region (4.19 ± 1.01), but low among counterparts in the Central (3.71 ± 1.35) and Volta (3.17 ± 1.89) Regions based on the means. Compared to participants in Ashanti Region, counterparts in the Bono Region (aOR = 0.64, 95% CI = 0.45–0.91), Central Region (aOR = 0.17, 95% CI = 0.12–0.25), and Volta Regions (aOR = 0.11, 95% CI = 0.08–0.17) had a lower likelihood of consistent condom use. Relative to participants who were sexually inactive, those who were sexually active had lower odds of using condoms (aOR = 0.74, 95% CI = 0.57–0.97).
Conclusion:
Regions from which antiretroviral medications were obtained, engaging in sexual activity and frequency of condom use in the previous year, and the likelihood of condom use in the future were the determinants of condom use attitude. The Ashanti and Bono Regions had a negative condom use attitude due to high perceived sexual health stigma, high perceived embarrassment associated with condom with condom purchase purchases and negotiations, and use. In contrast, counterparts in the Volta and Central Regions had positive condom use attitudes due to a low perceived sexual health stigma, low perceived embarrassment associated with condom negotiation and use, as well as low perceived embarrassment associated with condom purchases. Human Immunodeficiency Virus-positive populations in the Volta and Central Region are more likely to use condoms consistently and implement Human Immunodeficiency Virus preventive strategies due to the positive condom use attitudes compared to their counterparts in the Ashanti and Bono Regions. Implementing a condom use education campaign focused on addressing the negative cultural norms against condom use attitudes and emphasising the need for consistent condom use among the seropositive population is encouraged.
Keywords
Introduction
Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) prevalence among adults in Ghana is 1.67%, with regional variations,1,2 which continues to pose a public health problem despite national efforts to reduce local transmission. 3 The public health threat to Ghana’s productive population necessitated interventions such as enhanced early access to antiretroviral medications (ARVs) at no cost to people living with HIV/AIDS (PLWHA), regardless of the patient’s immunologic state or viral load. 4 The execution of programs to target populations at risk is vital for decreasing HIV infection in Ghana. 3 The national HIV estimates show that 334,721 people living with PLWHA in Ghana, including 22,926 women, 105,460 men, with 12,614 AIDS related deaths. 5 On the regional level, the Ashanti Region recorded 2997 new infections, the Central Region recorded 1140, the Bono Region recorded 875, while the Volta Region recorded 809 new infections. 5 Although the Ashanti Region has the highest HIV population in Ghana, the Bono Region recorded the highest prevalence of 2.66%, representing 20,134 PLWHA in the region, while the Volta Region recorded the lowest prevalence of 1.28%. 4
The primary method of contraception promoted at the HIV/AIDS clinics is the male condom, which is the predominant method of protection used by 77.0% of PLWHA. 6 Condom use remains low,7,8 especially among married individuals in Ghana, because of sociocultural norms. 9 Due to cultural expectations, married couples perceive condom use as undesirable; however, for HIV-positive populations, condoms provide a dual role of HIV transmission prevention and contraception. 8 Before the introduction of female condoms, women in heterosexual relationships were at a higher risk of HIV infection due to their lack of control over whether a condom was used by male partners. 4 Condoms are no longer biologically male-directed, and their use requires either male or female compliance and collaboration. Female condom use was unfortunately very low (4.5%) 10 relative to the high use (51%) 11 of male-controlled condoms in Ghana. The low utilisation has been attributed to partner disapproval, reduction in tactile sensation or pleasure during sexual encounters and lack of knowledge of their existence due to poor promotions to the public. 10 A study reported that almost half of PLWHA engaged in inconsistent condom use during sexual intercourse with irregular partners. 9 A greater proportion of PLWHA acknowledged engaging in unprotected sexual intercourse with casual partners. 9 Inconsistent condom use was substantially connected with not knowing that condoms are still needed if both partners are HIV positive, having a regular partner whose HIV status was either positive or unknown, and not receiving antiretroviral treatment. Despite progress, the benefits of condom use for PLWHA are not being completely realised. 12 Epidemiological and laboratory research demonstrate that condoms are effective in preventing HIV and sexually transmitted illnesses (STDs). 13 Condoms must be utilised consistently and correctly to attain optimal protection against HIV. 14 The transmission of HIV and STDs can occur with a single sexual encounter with an affected partner due to inconsistent or non-use of condoms. 14 Skills training and social support are efficacious strategies for fostering consistent condom utilisation, suggesting that education alone may be inadequate. 15 Condom use among HIV-positive individuals, especially during the acute phase of the disease in Ghana, could be a crucial part of HIV preventive strategies. Risk perceptions and self-efficacy are essential factors influencing condom utilisation, with increased usage rates noted in casual relationships relative to regular partnerships. 15
In Ghana, 65% of women and 62% of men are aware that ARVs are effective in treating HIV. 16 A recent study in Ghana suggests that over 50% of PLWHA on ARV in the Northern Region of Ghana use condoms consistently, have reduced sexual partners, reduced unprotected sex with married/regular partners and avoided casual sex. 3 The motivations for PLWHA to adopt safe sexual behaviours included the desire to prevent HIV transmission and to seek better health outcomes from ARV.3,17 A study in the Western Region of Ghana shows that viral load testing appears to support viral non-suppression. 18 The viral suppression rate among PLWHA on ARVs in the Western Region was below the United Nations Programme on HIV and AIDS (UNAIDS) target, and the non-suppression rate was high. 18 Viral load suppression appears to be hampered by both poor and fair adherence to ARVs, as well as by treatment durations of 6 months–2 years before viral load testing. 18 Increased access to ARV in Ghana may elevate reproductive aspirations but concurrently reduce condom utilisation, posing a complicated challenge for public health initiatives. An expected consequence of heightened reproductive aspirations among HIV-positive women may limit condom use. Reduced condom use can either facilitate women’s attainment of intended pregnancies or elevate the incidence of sexual HIV transmission.8,19,20 The possibility of unintended pregnancy or vertical transmission of HIV infection can be mitigated by reduced viral load among populations on ARVs. 8 Unfortunately, as of 2024, approximately 52.6% of PLWHA nationwide were not on ARVs in Ghana. 5 Research shows that the majority of PLWHA and those on ARV adopt positive sexual behaviour such as consistent condom use, lowering the number of sexual partners and facilitating partner(s) HIV testing due to the impact of counselling received before and after commencing ARV.21–24 PLWHA may be living with partners who may not have acquired HIV, or they may be in serodiscordant relationships. 14 Couple and partner testing, consistent condom usage, and providing ARV to the spouse living with HIV are critical prevention strategies for serodiscordant couples. 12 Condom use is important even if both partners have HIV to prevent reinfection. 25
Most individuals obtain their condoms through purchase rather than through free distribution schemes. 26 Persons acquiring condoms in retail establishments face multiple obstacles. 26 The majority of establishments concealed condoms beneath the counter, offering just one brand of male condoms and a restricted variety of lubricants. 26 Obstacles and unease associated with procuring condoms can lead to humiliation, adversely affecting both condom acquisition and utilisation. 26 Due to Ghana’s strong social and religious norms, 27 condom use, especially in marriage, is viewed as a deviant activity and often attributed to promiscuity.28–31 Broader religious and social penalties associated with condom use have resulted in secret-keeping and negative health outcomes.29–31
While embarrassment about condom negotiation and use for women can be a barrier, it can also facilitate individuals to explore alternate means of HIV prevention, such as the female-controlled barrier method, which may empower women to take ownership of their sexual health without the need for discussion with male partners. 32 According to Asiedu and Myers-Bowman 33 because of greater stigma associated with HIV/AIDS in Ghana, women are less likely to negotiate the use of condoms successfully. Moreover, in Ghana, women are disproportionately affected by the stigma associated with condom use proposals because the mere possession of a condom can be associated with adultery. 34 Individuals adopt numerous cognitive and behavioural techniques to overcome humiliation, which tend to decrease with age and experience.35,36 Studies show embarrassment about condom negotiation is a universal concern, affecting condom use regardless of the cultural context. 36 The power dynamics in sexual interactions often hinder condom negotiation, particularly for women, who may feel forced to forgo condom use.29,32,37 Women report higher degrees of embarrassment compared to men, particularly regarding condom negotiation and use, which can impair their capacity to advocate for safer sex practices.38,39
According to Helweg-Larsen and Collins, 40 condom identity stigma describes the social perceptions linked to condom possession. A person may be perceived as interesting, strong, active, promiscuous, or deviant. 40 These identity images (e.g., positive halos and bad stigma) associated with condom users or their possession can either promote or hinder condom use. 40 However, the term sexual health-related stigma (SHS) was used in place of the term condom identity stigma by the authors of this study to provide a more universal understanding of the term and also enhance understanding of the implications of condom use or their possession in the creation and maintenance of desirable and undesirable self-images and social impressions.
Differences in condom use attitudes between HIV-positive men and women could foster an understanding of the interpersonal processes involved in condom use in heterosexual relationships. Research shows that there is gender variation in the experience of SHS. 41 Men experience less SHS than women. 42 Compared to women, men reported higher rates of condom-protected sexual activity because men feel more in control over condom use than women. 42 Condom use differs functionally between men and women, raising the possibility that the differences in SHS may be a consequence of the respondent’s gender rather than the nature of condom attitudes in general. 43 In a conservative society like Ghana, largely influenced by culture and religion,27,28 variations in SHS between men and women could impact the use of condoms. The high negative SHS associated with women may lead to abandonment, physical aggression and allegations of infidelity when women insist or propose their use to their male partners.44,45 Thus, power imbalances in heterosexual relationships and sexual decision-making significantly impede condom use.46,47
According to Helweg-Larsen and Collins 40 existing instruments have predominantly concentrated on five characteristics of risky sexual behavior based on the expectancy-value models of decision-making: (a) the intraindividual and intrapsychic factors influencing risky sexual behaviours; (b) variables pertinent to conscious, rational, planned and deliberative decision-making while overlooking either the social and interpersonal determinants or fail to utilise alternative conceptual frameworks for analysing human behaviour; (c) an emphasis on the belief systems purportedly linked to condom utilization (e.g. the theories of reasoned and planned action); (d) an emphasis on health threats as the primary determinant of sexual behavior overall and condom use specifically, neglecting other significant variables unrelated to health that may influence sexual conduct and (e) a predominant focus on knowledge of disease mechanisms and education regarding risky sexual behaviours, disregarding numerous other relevant models of social influence. These shortcomings of popular condom use attitude scales are incorporated in the University of Chicago Los Angeles – Multidimensional Condom Attitudes Scale (UCLA-MCAS). 38
The psychometric factors influencing condom use among PLWHA in Kabriku et al.’s 3 study in the Northern Region of Ghana may differ from those in the other regions of Ghana. For instance, the differences in gender norms, levels of experiences of SHS, clinical practices and policies at different antiretroviral clinics in the Northern Region could influence condom use attitudes; thus, these attitudes could differ from the rest of Ghana. The adaptation of condom use attitude measurement instruments for Ghanaian sociocultural contexts is lacking.42,48,49 Current condom use attitude scales from other countries may not reflect PLWHA’s perspectives and may overlook the cultural nuances affecting condom use in Ghana.42,48,49 Moreover, despite Ghana being a multicultural and multiethnic country, condom use awareness campaigns are the same regardless of the cultural variations across regions. Most of the programs aimed at reducing HIV incidence in Ghana have overfocussed on condom use among adolescents and key populations.50,51 Limited studies have examined the determinants of condom use attitudes among PLWHA. The impact of Ghana’s multicultural variations, as well as critical psychometric factors incorporated in UCLA-MCAS, were not accounted for in Kabriku et al.’s 3 study. Therefore, the current study seeks to fill the research gap by assessing the determinants of condom use attitudes among PLWHA using the UCLA-MCAS in four regions of Ghana. The study aimed to assess the determinants of condom use attitudes among seropositive populations in four regions of Ghana.
Method and materials
Study design and study period
Following study approval and pretesting, a three-month period from February 2025 to April 2025 was used to undertake a cross-sectional systematic approach. This approach involved selecting HIV-seropositive participants attending antiretroviral care clinics in four Ghana regions, facilitating a comparison of condom use attitudes among PLWHA.
Study setting
The study focused on the Bono, Ashanti, Central and Volta Regions. Based on the Ghana AIDS Commission’s 2019 fact sheet estimates, 4 the Bono and Ashanti Regions recorded the highest rate of new HIV infections, while the Central and Volta Regions recorded the lowest rate of new HIV infections. The selection of two regions, each with the highest and lowest PLWHA in Ghana, was to allow for an understanding of the characteristics of PLWHA and determine their condom use attitudes.
Study population
The study population comprised HIV seropositive individuals who presented at ARV clinics seeking various types of care related to their diagnosis, aged 18 years and older.
Inclusion and exclusion criteria
Inclusion criteria
(a) HIV seropositive clients who are aged 18 years and older.
(b) Clients who can speak Twi, Ewe or English.
(c) Individual diagnosed as HIV seropositive for at least 12 months before the commencement of the study.
(d) Respondents with the above characteristics, willing and consented to participate in the study, were enrolled.
(e) Individuals with no form of visual or hearing impairment.
Exclusion criteria
(a) Minors.
(b) Individuals with visual and hearing impairment.
(c) HIV positive individuals who resided outside of the study regions and did not consent to participate in the study.
Study variables
The outcome variable was the condom use attitude score. A total condom use attitude was computed by averaging the scores of the 19 items from the MCAS (range: 1–7), with scores ⩾4.40 classified as ‘good attitude’ and <4.40 as ‘poor attitude’. The MCAS has a Cronbach’s alpha score of 0.803, which suggests a high internal consistency.
Explanatory variables. The explanatory variables examined in this study encompassed a range of sociodemographic, knowledge of viral load and sexual involvement, as well as relationship status relative to HIV status. Gender was categorised as women or men. Religious affiliation was categorised as Catholic/orthodox, Pentecostal/protestant, Islam, Traditional or other religions. Relationship status was categorised as single, married, divorced, widow/widower and separated. However, relationship status relative to HIV status was categorised as sero-discordant couple, seroconcordant couple or single with no sexual partner. These variables were selected based on theoretical relevance and prior literature indicating their potential influence on condom use attitude.38,52–55
Sample size determination
According to the 2019 HIV fact sheet published by the Ghana AIDS Commission in 2020, the total number of PLHIV in the Bono, Ashanti, Central and Volta Regions was 20,134, 76,672, 22,021 and 15, 091 respectively. 4 Using Slovin’s formula, the sample size was determined as follows: Sample size (n) = N/1 + Ne 2 . Where n = sample size, N = population size, e = margin of error (the level of precision or sampling error) at 5% margin of error → e = 0.05 at a 95% confidence interval. Using the formula, the sample size for the Bono Region = 20,134/1 + 20,134 (0.05) 2 = 392. A 10% adjustment for non-response = 436. Similar arithmetic computations were done for the Ashanti, Central and Volta Regions. Sample sizes for the Ashanti, Central and Volta Regions were 442, 437 and 433, respectively.
Data collection tool
A modified version of the validated UCLA-MCAS originally developed by Helweg-Larsen and Collins 40 was used as the data collection tool. The modified version UCLA-MCAS used in this study consisted of a 19-item instrument measuring 5 distinct factors as follows: (a) 3-items measuring reliability and effectiveness of condoms, (b) 3-items measuring sexual pleasure associated with condom use, (c) 5-items measuring the SHS (Identity Stigma), (d) 3-items measuring the embarrassment about negotiation and use of condoms and (e) 5-items measuring the embarrassment about the purchase of condoms. The objective of the UCLA-MCAS was to assist researchers in evaluating condom use attitudes from a multidimensional perspective among college students. However, to the best of our knowledge, this study is the first of its kind to use the UCLA-MCAS to study condom use attitudes among a population subtype such as PLWHA. The questionnaire consists of three sections. The first section consists of items exploring participants’ demographic and background characteristics, including age, gender, marital status, religion, sexual experience and condom use during the last sexual experience.
The second section explored participants’ knowledge of their viral load, condom use during the last sex with the opposite sex and their viral load assessment schedule. The third section explored participants’ condom use attitudes from the 19-item instrument of the UCLA-MCAS. Participants were asked to respond to a seven-point Likert scale that ranged from strongly disagree to strongly agree, where 1 = strongly disagree, 2 = slightly disagree, 3 = disagree, 4 = Neutral, 5 = agree, 6 = slightly agree and 7 = strongly agree. Respondents were asked to choose the level of agreement with each statement that most represented their opinion. To validate the resultant questionnaire, the research team translated and adjusted the research instruments. Specifically, the tool’s usability, content’s validity, and the conceptual construction’s validity were measured. The original tool was written in English and translated into Ewe, Fante and Twi which are the local languages spoken in the Volta, Central, Bono and Ashanti Regions by the research team and supported by a language expert with experience in the health sciences who also carried out an independent second translation for comparison and transcribed back to English to check for consistency and correctness of the translation. Through consensus, an expert panel modified and combined the two forward-translated versions into the Ewe, Fante and Twi versions. This was an attempt to produce an instrument of the highest quality. An interdisciplinary four-member team, who were also experts in transcultural psychiatry and family medicine in Ghana, evaluated the questionnaire during the translation, reverse translation and entire questionnaire assessment process. To assess for potential mistranslations and language misunderstandings and subsequently monitor the process, the research team monitored the process and deliberated over the question items and data during regularly scheduled meeting sessions. Reliability analysis was conducted by computing Cronbach’s α and composite reliability. Scales with Cronbach α and composite reliability of 0.8 and 0.70, respectively, were considered to have met the minimum threshold. 56 The modified questionnaire was administered in all the selected health facilities across the regions. After the validation process, the questionnaire was deployed in the four study regions.
Data collection procedure
A two-stage sampling technique was used to first select the hospitals and then the respondents from the selected hospitals. The sampling of respondents was done by the principal investigator, assisted by three trained assistants. During stage one in the Bono, Ashanti and Central Regions, a Ghana Health Service-managed hospital was chosen from among five hospitals using balloting. However, in the Volta Region, a Christian Health Association of Ghana-managed facility was purposively included in the eligible accredited ARV-designated care facilities to introduce diversity. In each of the four regions, five urban health facilities were selected based on the criteria that they provided ARV services with a larger HIV seropositive population attendance that could provide the required number of respondents estimated within the three-month stipulated time frame for the study. Based on these criteria, the first five hospitals with large attendances at clinics that provided ARV services were chosen from each region. Out of the five initial ARV clinics, one clinic was chosen from each region through balloting, and that facility represented the region for the study. In all, a total of four urban health facilities were chosen for this study. The principal investigator and three field officers with a working knowledge and understanding of Ewe, Twi and Fante, three major local languages spoken in the study regions, collected the data. The Tafo Government Hospital was selected in the Ashanti Region. The Dunkwa on Offin Government Hospital represented the Central Region. The remaining facilities were the Sunyani Municipal Hospital and Saint Anthony’s Catholic Hospital, representing the Bono Region and the Volta Region, respectively.
In stage two, simple random and systematic proportional sampling techniques were deployed to select eligible respondents at the ARV clinics. Study participants were chosen carefully after screening to ensure they all met the study’s inclusion criteria. The numbers of eligible participants were arranged from top to bottom, with the number of participants who reported first in a day placed on top and followed in order of the time of hospital reporting. For instance, for the Bono Region, the sampling interval was determined as follows: the sampling interval (nth folder) to pick a respondent was determined by dividing the total number of participants’ hospital attendance in the past 3 months of the previous year before the commencement of data collection by the estimated sample size.
The first participant’s hospital number to pick was determined using balloting, and the subsequent eligible respondents’ hospital numbers were selected at the intervals until the estimated sample size was obtained for that region. For the Bono Region, a total ARV attendance of 850 was reported in the previous 3 months before the study. The sampling interval was determined as follows: 850/436 ≈ 2nd interval. Participants whose folder numbers were positioned at the 2nd and 1st intervals in the queue in the Ashanti, Central and Volta Regions who met the inclusion criteria and expressed interest in the study were enrolled. This process was repeated separately for each region until the required sample size for each ARV clinic was attained. A written informed consent was provided, and participation was entirely voluntary.
Invitations were sent out in person, either by the principal investigator or a member of the research team, for recruitment. The process was aided by the unit heads and nurse managers, who sent out study leaflets created by the research team informing eligible participants that a researcher was visiting the units and inviting volunteers. In addition, unit heads and nurse managers were requested to offer physical space where the questionnaire could be completed. The questionnaires were completed in a way that did not conflict with ARV service delivery or keep clients waiting after service. Respondents who consented to participate in the study were enrolled. About 20 min were allotted for the completion of each questionnaire. The process was repeated until the proportionate estimated sample size for each ARV clinic in each region was obtained. All the distributed questionnaires were returned immediately and checked for completeness and accuracy of responses by a field officer of the research team. Thus, a 100% response rate was achieved. Data collection commenced simultaneously in the Bono, Ashanti, Central and Western Regions, spanning approximately 16 weeks. While respondents in the Ashanti Region were sampled by the principal investigator, data collection in the Bono, Central and Volta Regions was carried out by three field officers. The researchers believed this sampling technique would offer the best results for achieving the study objectives, as the method was likely to yield both an objective outcome representative of the target population and could be generalisable.
Data quality and assurance
The questionnaire was meticulously designed and pretested to ensure data quality. Before the initiation of fieldwork, the lead investigator conducted intensive training for three field officers, encompassing the study’s objectives, checklist, sampling methodologies and effective techniques for eliciting responses from participants. The questionnaire underwent pretesting on 10% of the total sample size at hospitals outside the facilities designated for the study, separately in each region. This was done to verify that the instrument accurately assessed the necessary information for the study and to rectify ambiguous language. Data were meticulously cleaned daily before inclusion in a spreadsheet. All participants' details have been de-identified.
Data processing and analysis
Descriptive analysis was performed on respondents’ demographics. A further analysis establishing an association between respondents’ sociodemographic factors and knowledge of viral load was carried out. Data were analysed using SPSS version 27. Continuous data were summarised using mean, median and standard deviation, and categorical data were summarised with frequencies and percentages. Reliability analysis was conducted by computing Cronbach’s Alpha (α) and composite reliability. Scales with Cronbach’s α and composite reliability of 0.8 and 0.70, respectively, were considered to have met the minimum threshold. 56 In this study, the Cronbach α and composite reliability of all construct items exceeded 0.7. Therefore, the scale had satisfactory reliability. A UCLA-MCAS self-assessment checklist containing five psychometric properties was presented using mean, median and standard deviation. The total average score of the five areas was obtained, and the overall median was categorised as high and low to indicate respondents’ performance. A score above the overall median was categorised as high, and a score below or equal to the overall median was categorised as low. Normality tests performed on the continuous variables using the Shapiro–Wilk test and graphical charts showed that the data were not normally distributed. Thus, the Mann–Whitney U test and Kruskal–Wallis’s test were used to determine the relationship between condom use attitude and the explanatory variables. Inferential analysis was done using binary logistic regression to explore the relationship and the strength of the explanatory variables associated with condom use attitudes. Unadjusted logistic regression was done first for each variable to obtain the crude odds ratio. Based on available literature, age, marital status and gender are potential confounders. Thus, age, marital status and gender were adjusted for potential confounders.57,58 Variables significant at p-value < 0.05 in the bivariate analysis were added in a multivariable logistic regression model to obtain adjusted odds ratios (aOR). Based on the Hosmer–Lemeshow goodness-of-fit test, a p-value of 0.516 obtained for the model indicates that the model is a good fit.
Results
Demographics of participants and knowledge of viral load and assessment
Table 1 shows the demographic information of participants as well as their knowledge of viral loads in the four regions of Ghana. Most of the participants were women (67.4%). About 43% of respondents were married. A majority of respondents had sexual encounters with either a man/woman within the last 12 months (58.1%) before the commencement of the study. More than half of the respondents (n = 649; 63.9%) had sexual encounters in the last quarter of the previous year. About 67.0% of respondents engaged in unprotected sex. More than half of the respondents (61.1%) reported knowing their viral load, with most (64.7%) repeating their viral load assessments 12 months after initiation of the ARV schedule.
Demographics of participants, sexual history and knowledge of viral load (N = 1748).
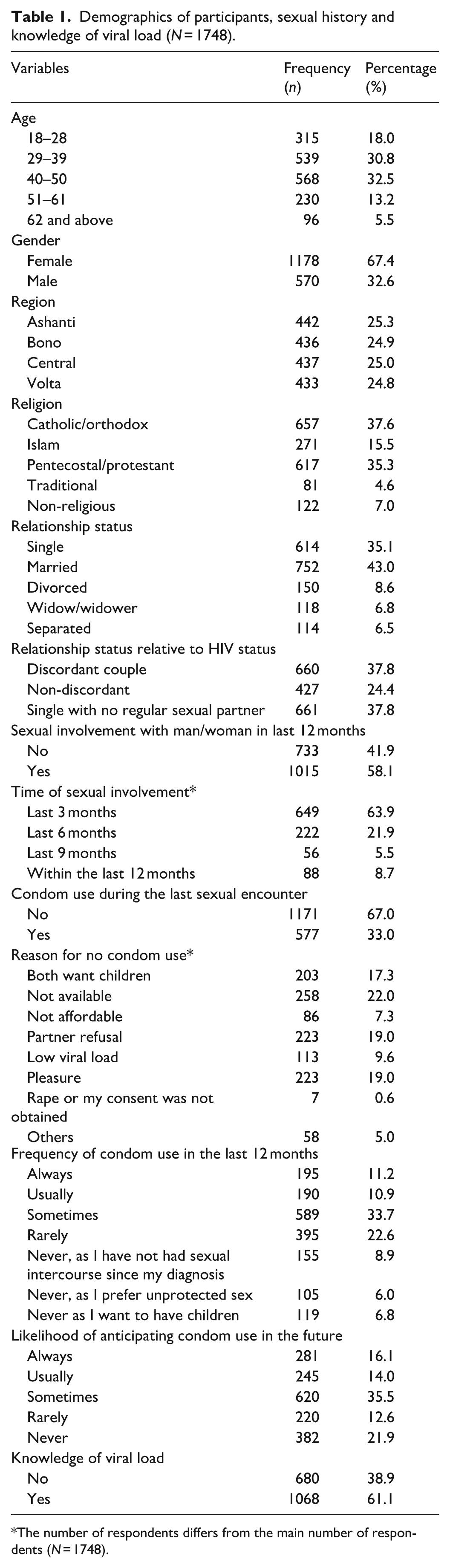
The number of respondents differs from the main number of respondents (N = 1748).
Description and reliability of items for the UCLA-MCAS self-assessment checklist
Table 2 shows the minimum score, maximum score, median, mean and standard deviation of items associated with the UCLA-MCAS self-assessment checklist. To determine these scores, respondents were asked to choose the best level of agreement with each statement from a 7-point Likert scale. For positive statements, strongly agree = 7, agree = 6, slightly agree = 5, neutral = 4 slightly disagree = 3, disagree = 2 and strongly disagree = 1. The reverse score was used for negative statements. For factual statements such as condom reliability and effectiveness, a correct response was categorised as low risk, while an incorrect response was categorised as high risk. However, for assessing attitudes such as pleasure and SHS, affirmative responses indicated poor attitudes, while those disagreeing with the statements indicated good condom use attitudes. The combined overall average score for condom attitude was 4.40.
Description and reliability.

The composite mean for feeling embarrassed about condom negotiation and use is 4.49, indicating that respondents slightly agreed with statements of embarrassment about condom negotiation and use. Expectedly, the mean scores for the statements ‘When I suggest using a condom, I am almost always embarrassed’ and ‘It is really hard to bring up the issue of using condoms to my partner’ were 4.64 and 4.47, respectively, indicating respondents’ slight agreement with the statements.
Condom effectiveness and reliability had the highest composite mean among the five psychometric properties of the UCLA-MCAS scale. The composite mean for condom reliability and effectiveness was 5.45, indicating that the majority of respondents agreed that condoms were reliable and effective against STIs, including HIV.
A composite score for SHS was 4.48, indicating that respondents slightly agreed with the statements on the SHS. The mean scores for the statements ‘People who suggest condom use are a little bit jerky’, ‘Women think men who use condoms are jerks’ and ‘Men who suggest using a condom are boring’ are 4.47, 4.45 and 4.87, respectively, indicating slight agreement with the statements.
Relationships between condom use attitudes, sexual history, demographic information and knowledge of viral load
Table 3 shows different levels of association between demographics and condom use attitudes of respondents. Among the regions, the mean score for perceived embarrassment associated with condom purchases was highest in the Ashanti Region (5.77) and lowest in the Volta Region (3.17), with p< 0.001. Among the age groups, respondents between the ages of 18 and 28 years experienced the highest SHS associated with condoms, with a mean of 4.64 and a p-value of 0.001. Moreover, married women experienced the highest level of SHS (4.57), with the lowest SHS (4.21) experienced by respondents who were separated (p= 0.008).
Association between condom use attitude and demographics and knowledge of viral load.

CRE: reliability and effectiveness; P: pleasure; SHS: sexual health-related stigma; EACU: embarrassment about condom negotiation and use; EACP: embarrassment about condom purchase.
Associations were determined using the Mann–Whitney U test at a significance level (α = 0.05). All other variables and their associations were determined using the Kruskal–Wallis test at the significance level (α = 0.05).
While the Ashanti Region recorded the highest perceived interruption of sexual pleasure associated with condom use, counterparts in the Volta Region recorded the lowest perceived interruption of sexual pleasure associated with condom use, with a p value of <0.001
The condom reliability and effectiveness psychometric rating was greatest among the age group 51–61 years, with a mean of 5.01 and p-value = 0.001. Among the regions, condom reliability and effectiveness were highest in the Ashanti Region (5.77), with the lowest condom reliability and effectiveness recorded in the Central region (4.78), with a p-value of < 0.001.
Determinants of condom use attitudes
Table 4 presents the binary logistic regression analysis, which examined the number of variables that best determine participants’ condom use among the study population. The model shows that out of the several factors, 10 variables were significantly associated with high condom use attitudes.
Determinants of condom use attitudes.
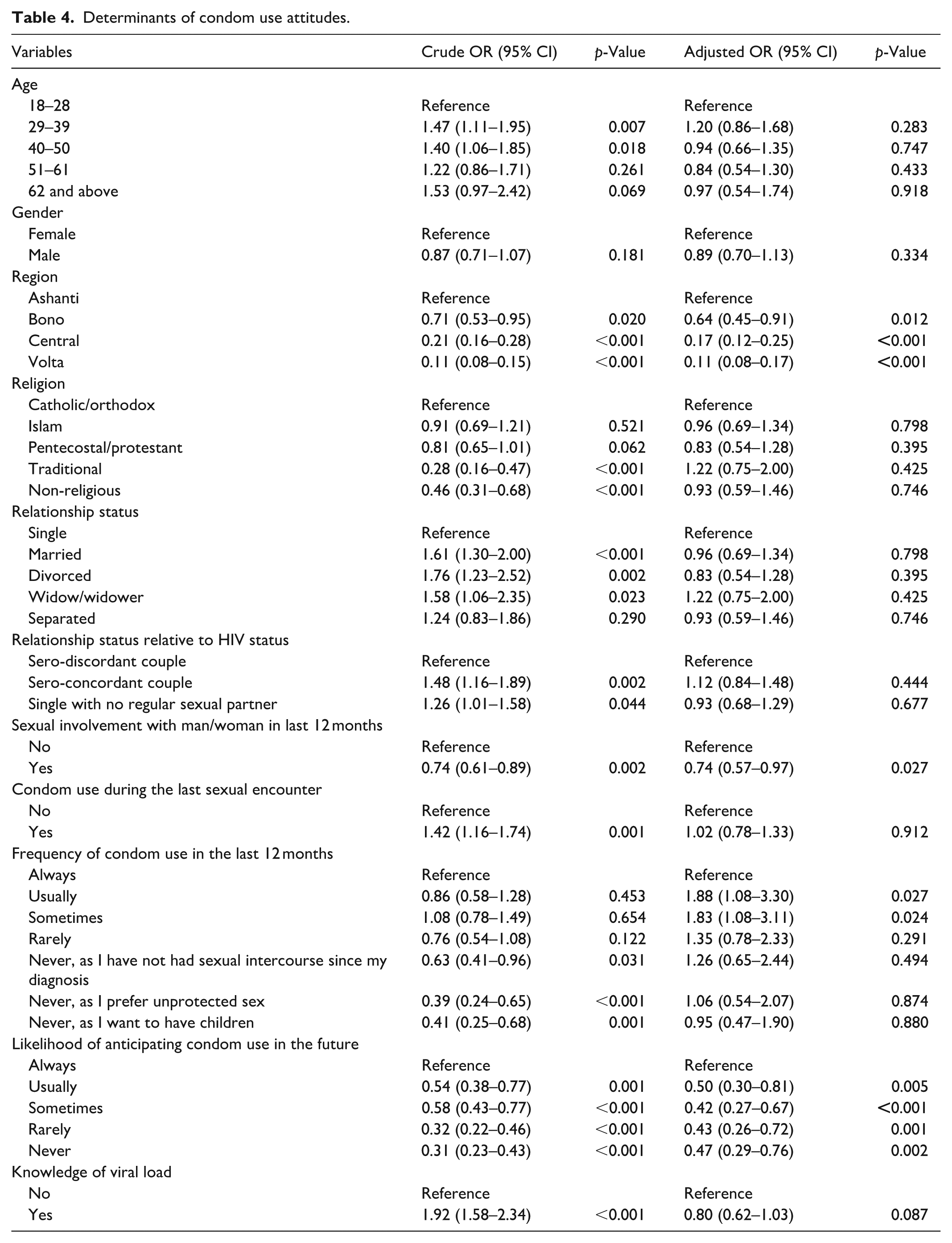
After adjusting for possible confounders, participants residing in the Bono region (aOR = 0.64, 95% CI: 0.45–0.91); Central Region (aOR = 0.17, 95% CI: 0.45–0.91) and Volta Region (aOR = 0.11, 95% CI: 0.08–0.17) had lower odds of using condoms compared to their counterparts in the Ashanti region.
Participants who were sexually involved with men/women in the last 12 months had 26% lower odds of using condoms compared to those who were sexually inactive (0.74, 95% CI: 0.57–0.97).
Participants who reported ‘usually’ using condoms in the last 12 months had 1.88 times higher odds of having a high condom use attitude compared to those who always used a condom (95% CI: 1.08–3.30). Additionally, participants who reported using condoms ‘sometimes’ in the last 12 months had 1.83 times higher odds of having a high condom use attitude compared to those who always used a condom (95% CI: 1.08–3.11).
The likelihood of anticipating condom use in the future was associated with condom use. Participants who reported anticipating using condoms ‘usually’ in the future had 50% (0.50, 95% CI: 0.30–0.81) lower odds of having a high condom use attitude compared to those who anticipating using condoms ‘always’ in the future. Participants who reported using a condom ‘sometimes’ in the future had 58% (0.42, 95% CI: 0.27–0.67) lower odds of using a condom compared to those who anticipated using a condom ‘always’ in the future.
Regional variations in condom use attitude
Table 5 shows the regional variations in condom use attitudes among the four study regions. Overall, about 50.6% of participants had a positive condom-use attitude. The region from which participants attended the ARV clinic was statistically significant with condom use attitude, with a p-value < 0.001 indicating strong evidence of association. While the Ashanti and Bono Regions recorded the highest negative condom use attitude (n = 322; 72.9%), the Volta Region had the highest positive condom use attitude (n = 336; 77.6%).
Association between region and condom use attitude.
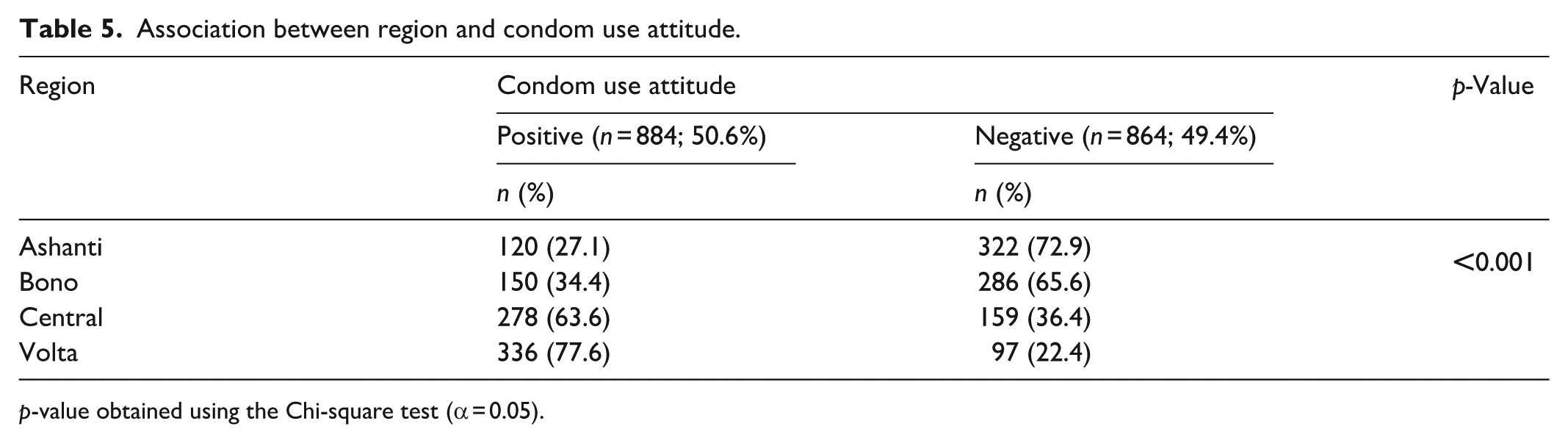
p-value obtained using the Chi-square test (α = 0.05).
Discussion
Ghana is a multicultural and multiethnic country 59 and the four study regions may differ in terms of sociocultural norms about condom use. Thus, the 1748 respondents who participated in the study across four regions of Ghana may have different world views about condom use. Each of the four regions contributed about one-fourth of the participants to the study. A little over one-fourth of the participants were between 40 and 50 years old, with a greater number being women. The greater number of HIV infections among female respondents (Table 1) highlights young women’s increased susceptibility to the virus. 60 This outcome is consistent with the Ghana AIDS Commission’s National and Sub-National HIV and AIDS Estimates and Projections: 2020 Report. 61 The gendered nature of HIV infection in Ghana could be the result of several reasons. Women are disproportionately affected by the virus due to their increasing participation in riskier sexual practices, including unprotected sex. 62 Women are biologically more prone to HIV infection than men because of the larger mucosal surface exposed during penile penetration. 63 The walls of the vaginal mucosa are thin and more easily torn, creating an entry point for HIV into the bloodstream. 64 The greater number of female infections in Ghana could also be due to the country’s implementation of a robust Prevention of Mother-to-Child Transmission (PMTCT) program. 60 The PMTCT policy had achieved a 99.9% HIV testing rate for registered pregnant women, 65 of which 91.4% of HIV-negative rates were recorded among infants with seropositive mothers in Ghanaian studies. 66 Unlike women, men are only screened opportunistically for HIV symptom distress.
Two-thirds of participants not using condoms during their last sexual encounter (Table 1), despite respondents’ awareness of their seropositive status is not only an indication of poor use but also could have a negative implication for Ghana’s HIV infection control.
Condom reliability and effectiveness had the highest composite mean score of 5.45, with regional variations. Nonetheless, the generally high condom reliability and effectiveness rating did not translate into actual condom use (Table 1). Even though there is a high condom awareness campaign on both traditional and social media, the differences in condom reliability and effectiveness among the regions, coupled with the poor use, may be due to the lack of culturally tailored messages to effect the necessary behavioural change in the regions. Ghana is a multicultural and multiethnic country with different socio-cultural norms about condom use. Each region’s unique cultural norms could promote or limit participants’ perception of condom reliability and effectiveness. More than half of the participants (n = 1068; 61%) knew their viral loads. Participants with knowledge of their viral load reported greater perception of condom reliability and effectiveness compared to their counterparts with no knowledge of their HIV viral loads (Table 3). However, those with knowledge of their viral loads believed condoms interfered with sexual pleasure. This variance in the perceptions of condom reliability and effectiveness and pleasure associated with condom use could be due to the differences in the overall perception of sexual risk between the two groups. While those with no knowledge of their loads were likely to prioritise safety over pleasure, those with knowledge of viral loads may be likely to engage in unprotected sex due to a false sense of security rooted in their knowledge of their viral load statuses.
Age was statistically significant with sexual health stigma, with SHS decreasing with age. While those aged 18–28 years perceived the greatest SHS, the older participants had the lowest SHS perception. Since SHS directly determines condom use,67,68 the older age population are more likely to engage in condom use than the younger population. This is because older people have a more permissive attitude toward their sexual behaviour than younger respondents. 69 Condom users had a greater perception of SHS relative to non-users. From Table 3, respondents who reported using condoms during the last sexual encounter had a greater perception of SHS compared to respondents who had unprotected sex during the last sexual encounter. Additionally, respondents who reported using condoms ‘usually’ in the past year had a greater perception of SHS compared to those who reported ‘never’ using condoms (Table 3). It is possible that participants engaged in condomless sex as a result of the high perception of SHS associated with condom use. This is consistent with a Chinese study that reported high odds of condomless anal intercourse among men who have sex with men, due to perceived SHS. 70 A high level of SHS was observed in the Ashanti, Bono and Central Regions, whereas stigma associated with condom use was relatively low in the Volta Region. The negative attitudes toward condom use in the Ashanti, Bono and Central Regions may be attributed, in part, to the heightened SHS prevalent in these areas. Conversely, the more favourable attitudes toward condom use observed in the Volta Region may be influenced by the comparatively lower levels of SHS. This finding aligns with a study conducted in China among men who have sex with men. 67 In that study, Shen et al. 67 posited that lower levels of SHS were associated with an increased willingness to negotiate condom use, largely due to reduced feelings of embarrassment when purchasing condoms. Drawing on Shen et al.’s 67 argument, the elevated levels of SHS observed in the Ashanti, Bono and Central Regions may be explained by comparatively higher levels of embarrassment associated with condom negotiation and, more notably, condom purchases, as indicated in Table 5. In contrast, respondents from the Volta Region reported the lowest levels of perceived SHS, with most disagreeing that they experienced embarrassment during condom negotiation or when purchasing condoms (Table 5).
There was a strong statistical difference between the four regions and condoms interfering with sexual pleasure. Respondents in the Volta Region had a better condom use attitude than the Ashanti, Bono and Central Regions (Table 5). Participants who were aware of their viral load status generally expressed a neutral attitude toward the notion that condom use diminishes sexual pleasure. Hanbury and Eastham 71 suggested that respondents with awareness of their viral load status may have nuanced views on condom use, recognising both the protective benefits and their potential to reduce sexual pleasure, leading to ambivalence rather than a definitive stance on whether condoms interfere with sexual pleasure. Conversely, respondents lacking awareness of their viral load status predominantly disagreed with the assertion that condom use detracts from sexual pleasure. Human sexual behaviour is primarily motivated by pleasure. 72 Any artifice that obstructs the pleasure of sex is therefore likely to be avoided or accepted with reluctance. 73 This is especially the reality with latex condoms, which are the mainstay of contemporary global initiatives aimed at stopping the spread of STIs. In addition to limiting physical touch, decreasing tactile sensation and attenuating heat transmission, condoms also impose a mechanical barrier between sex partners, all of which lessen the pleasure of sexual activity.73,74 A study among senior high school students in Ghana showed that false beliefs that condoms interfere with the pleasure of sexual activity made condom use unappealing to young people. 40 Based on the arguments by scholars that directly correlate poor condom use behaviour with poor pleasure perception,73,75 it is possible that actual condom use among respondents with knowledge of their viral load status may be poor.
There were regional differences in the perceived embarrassment associated with condom negotiation and use, with respondents in the Ashanti and Bono regions having the highest perceived embarrassment associated with condom negotiation and use. The conservative cultural norms in the Ashanti and Bono regions may perpetuate stigma around condom negotiation, making it difficult for sexually active individuals to negotiate for their use. Research shows that in culturally conservative contexts, negotiating for condom use can be associated with infidelity, promiscuity and lack of trust in a partner. 76 These negative connotations around condom-use discussions may deter sexually active individuals from negotiating for their use. 76 Additionally, in Africa, condom related communications can be taboo, and sexually active individuals may feel embarrassed to bring up discussions about condoms due to fear of judgment or rejection. 77 In regions with such strong conservative cultures, sexual discussions are often avoided, and condom use negotiation can be regarded as a violation of cultural norms due to the symbolic meaning that associates condoms with sex, deviant behaviour and promiscuity.32,77 In some cases, condoms are often associated with disease prevention, which can create a sense of awkwardness or discomfort. 78 These perceptions can lead to embarrassment, as negotiating to use condoms may be interpreted as either a desire to maintain emotional distance rather than promote physical closeness or a desire to prevent diseases rather than promote well-being. 32 Thus, the high perceived embarrassment associated with condom negotiation and use in the Ashanti and Bono Regions could limit their use and increase risky sexual behaviour among HIV-positive individuals. While respondents in the Central Region were neutral in their responses to perceived embarrassment about condom negotiation and use, those in the Volta Region denied any embarrassment in condom negotiation and use. More disturbingly, results from Tables 3 and 4 show a likely decline in consistent condom use among the study population. The likelihood of condom use among participants who reported ‘usually’, ‘sometimes’ rarely and ‘never’ in the future was low compared to counterparts who reported ‘always’ using condoms (Table 4). Strikingly, participants who reported consistent use in the past year (with higher odds) had lower odds of future use. Moreover, there appears to be a direct link between the frequency of condom use and perceived embarrassment associated with condom negotiation and use. A comparison of the extent of perceived embarrassment associated with condom negotiation and use between consistent and non-condom users shows that consistent users faced the greatest perception of embarrassment associated with condom negotiation and use compared to non-users. For instance, participants who reported using condoms ‘always’ had the greatest perception of embarrassment associated with condom negotiation and use in the future than their counterparts who reported ‘never’ using condoms (Table 3). Thus, condomless sex in the future is expected as consistent users may want to avoid societal judgment or the embarrassment associated with condom negotiation and use. Without adequate viral suppression, the inconsistent condom use of participants in both the previous year and in the future could increase Ghana’s new HIV infection numbers. It is possible participants who engaged in condomless sex may perceive less responsibility to protect their partners. Awareness of the implications of such risky sexual behaviour and the possibility that inconsistent use may accelerate disease progression had little impact on behavioural change in the study population. Available data from the Ghana AIDS Commission reported by Effah 79 and Graphic Online 80 indicated that fifty people acquire the virus daily. Outcomes are consistent between this current study and a study in Ceará State, Brazil. 81 According to Siqueira et al. 81 about 56.6% of HIV-positive individuals in their study avoided using condoms during the last sexual encounter, compared to 1171 (67%) respondents in this study.
While the Ashanti and Bono Regions had the highest perceived embarrassment associated with condom purchase, respondents in the Bono Region were neutral. A study shows that cultural views greatly influence attitudes toward condom purchases. 77 A previous Ghanaian study has attributed the high perceived embarrassment associated with condom purchases in the Ashanti Region to the region’s culturally conservative norms, which largely reject condom purchases, viewing condoms as contradictory to traditional values. 28 In the majority of the communities in the Ashanti Region, condom purchase is associated with immoral sexual behaviour, such as sexual promiscuity. 82 Oswalt et al. 83 explained that in context with high perceived embarrassment associated with condom purchase, participants were more likely to avoid condom purchases, citing fear of being judged as promiscuous or irresponsible. The high perceived embarrassment associated with condom purchase in the Ashanti and Bono Regions would not only encourage condomless sex but also complicate Ghana’s efforts to promote sexual health programs. However, respondents in the Volta and Central Regions had low perceived embarrassment to purchase condoms, likely attributable to the high condom use attitude, as shown in Table 5.
Compared to participants who were not sexually active, participants who were sexually active had lower odds of using condoms, as shown in Table 4. None of the three regions, Bono, Central and Volta Regions, had higher odds than the Ashanti Region of using condoms during the last sexual encounter, with aORs of 0.64 times, 0.17 times and 0.11 times, respectively (Table 4). Participants who reported inconsistent use, such as ‘usually’ and ‘sometimes’ in the previous year, had 1.88 times and 1.83 times higher odds of using condoms in the past year compared to consistent users, such as ‘always’ using condoms. The possible explanation is that the habitual condom use could have significantly increased the odds of condom use at the most recent sexual intercourse. 84 Evidence shows that consistent users could have an established pattern of safer sexual practices that favour condom use. 85 Nevertheless, the effectiveness of condoms against STIs when used consistently may be over 95%, 86 while inconsistent use without the deployment of safe HIV transmission precautions could provide minimal or no protection against HIV, resulting in only 8% of HIV infections being averted. 86
Table 5 demonstrates regional differences in condom use attitudes. Even though more than half of the participants (n = 884; 50.6%) had positive condom use attitudes (Table 5), actual use was poor (Table 1). Two-thirds or more than half of respondents in the Ashanti and Bono Regions, respectively, had poor condom use attitudes. However, their counterparts from the Volta and Central regions indicated good condom use attitudes. The differences in condom use attitudes may be attributable to several factors. The poor condom use attitude in the Ashanti and Bono Regions could be due to the high perceived SHS and high embarrassment with negotiating condom use. Moreover, the Ashanti Region alone was impacted by both a high perceived interference with sexual pleasure and a high embarrassment during condom purchase. Conversely, the Volta Region had the lowest perceived interference with sexual pleasure, the lowest perceived embarrassment to purchase condoms, as well as the lowest perceived embarrassment associated with condom negotiation and use (Table 5). Ghana is a country with a strong religious influence, and these religious edicts can introduce conservative views limiting condom use and negatively influencing condom use attitudes. Additionally, the Volta and Central Regions may have more robust sexual health dissemination systems and greater access to educational programs regarding condom use than those in the Ashanti and Bono Regions of Ghana. 87 Ocran and Alldred 28 argued that most condom use programs in culturally conservative areas of Ghana, such as the Ashanti and Bono Regions, promote condom use alongside predominantly abstinence-based and morally focused programmes to avoid community rejection. This duality of sex education interventions limits condom use promotion and positive condom use attitudes. 28 Even though condom use attitude was high, actual use was poor. The regional variations in condom use attitudes may also be attributable to high condom use awareness campaigns. However, the low actual use could be due to the promotion of generic messages instead of culturally tailored information consistent with the various cultural norms in each region. It can be assumed that the cultural norms in the Volta and Central Regions may be more permissive to condom use than those in the Ashanti and Bono Regions.
Limitations
Questionnaires were the only instrument used to gather data; it is therefore recommended that future studies include in-depth interviews, focus group discussions or a stratified sampling technique to obtain the diverse views of respondents. Because it included only four ARV clinics across Ghana’s 4 of 16 regions, the findings are not nationally generalisable or representative. It is suggested that future studies cover all 16 of Ghana.
The high women-to-men ratio in the sample could be due to sampling error as a result of the sampling technique used. As a result, biases associated with the systematic design, such as selection bias, may be the cause of the high women-to-men ratio observed. It is suggested that future studies deploy a stratified sampling or population-based study to objectively compare the gender ratio of HIV infections between men and women in Ghana.
Conclusion
The study focused on the determinants of condom use attitudes among seropositive individuals in four regions of Ghana with varied cultural orientations. Region of treatment, engagement in sexual activity in the previous year, frequency of condom use in the previous year, and the likelihood of condom use in the future were the determinants of condom use attitude. A significant majority of participants had a positive condom use attitude despite the poor actual use. The Ashanti and Bono had a negative condom use attitude due to a high perceived sexual health stigma, high perceived embarrassment associated with condom negotiations and use, as well as high perceived embarrassment associated with condom purchases. In contrast, counterparts in the Volta and Central Regions had a positive condom use attitude due to a low perceived sexual health stigma related to condoms, low perceived embarrassment associated with condom negotiation and use, as well as low perceived embarrassment associated with condom purchases. Generally, the high perceived sexual health stigma, high perceived embarrassment associated with condom negotiations and use, as well as high perceived embarrassment associated with condom purchases, hampered consistent condom use in the study regions. This implies that the HIV-positive populations in the Volta and Central Region are more likely to use condoms consistently and implement HIV preventive strategies due to the positive condom use attitudes compared to their counterparts in the Ashanti and Bono Regions, with negative condom use attitudes.
Policy implications for practice
Despite Ghana being a multicultural and multiethnic country, the current National Condom Strategy as well as condom promotion campaign assumes that the cultural norms against condom use in the regions are either similar or non-existent. However, the results of the study suggest that there are regional variations in cultural norms against condom use and negotiations to use. The lack of culturally tailored messages in Ghana’s condom promotion campaigns in the regions may have contributed to the poor condom use attitudes in some regions and the rising numbers of new HIV infections. The lack of culturally tailored messages for each region necessitates the development and implementation of regionally specific HIV prevention plans, as the sociocultural norms against condom use may differ. Thus, culturally tailored HIV/AIDS interventions are required in the face of the glaring differences in SHS and embarrassment associated with condom purchase as well as negotiating to use condoms.
To reduce the perceived embarrassment about condom use, targeted campaigns aimed at challenging conventional sexual norms and normalising condom use, as well as conversations about sexual health, should be implemented in the Ashanti and Bono Regions. Moreover, there must be training for providers at ARV clinics in the Ashanti and Bono regions on patient-centred practices and stigma-sensitive communication so that clients can freely discuss their sexual health issues in a judgment-free care setting. Due to the high level of embarrassment about condom purchases, calls on the Ghana AIDS Commission to consider the implementation of condom access strategies in a discreet and non-stigmatising setting. Interventions such as the installation of condom vending machines in public restrooms, neighbourhood pharmacies or peer-led outreach programs are recommended. Nonetheless, the relatively high positive condom use attitudes in the Volta and Central Regions provide an opportunity for policymakers to improve and scale up existing condom use stigma reduction strategies. Health authorities and policy makers in the Volta and Central Regions collaborate with their counterparts in the Ashanti and Bono Regions to replicate best practices attained in the Volta and Central Regions in the Ashanti and Bono Regions.
These regionally specific outcomes on condom use attitudes can be utilised by the Ghana AIDS Commission and the Ministry of Health in designing a sexual health education curriculum that incorporates cultural differences into condom use-related stigma and attitudes campaigns in different regions of Ghana. Based on this region-specific evidence, future versions of the Ghana National Condom Strategy and the National HIV and AIDS Strategic Plan need to have messages specific to each regional situation.
Overall, this study shows that HIV prevention is far more than educating a population about condom use, as psychological barriers could limit their use. However, a combination of biomedical HIV prevention strategies (condom use) with culturally appropriate behavioural interventions that deal with stigma may increase condom use. Thus, for Ghana to attain the UNAIDS 95-95-95 targets for HIV prevention and treatment, the country should consider the implementation of a multi-faceted approach that reduces psychological barriers to consistent condom use among HIV-positive heterosexuals.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251379306 – Supplemental material for Regional and cultural determinants of condom use attitudes among HIV seropositive heterosexuals in Ghana: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121251379306 for Regional and cultural determinants of condom use attitudes among HIV seropositive heterosexuals in Ghana: A cross-sectional study by Abdul-Karim Abubakari, Janet Gross, Emmanuel Adusei-Poku, Isaac Kwabena Boateng, Richard Odame Asare and Phanuel Kelvin Dzamefe in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251379306 – Supplemental material for Regional and cultural determinants of condom use attitudes among HIV seropositive heterosexuals in Ghana: A cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121251379306 for Regional and cultural determinants of condom use attitudes among HIV seropositive heterosexuals in Ghana: A cross-sectional study by Abdul-Karim Abubakari, Janet Gross, Emmanuel Adusei-Poku, Isaac Kwabena Boateng, Richard Odame Asare and Phanuel Kelvin Dzamefe in SAGE Open Medicine
Footnotes
Acknowledgements
We gratefully acknowledge the many staff and the managers of the selected hospitals who were involved in the study. They have contributed to and supported this work. We sincerely thank Mr. Seth Boateng and Dr. Frimpong at the Kwame Nkrumah University of Science and Technology, Akan language and Psychiatry departments, respectively. Also, to Mr. Asare Boateng at the Ghana Institute of Languages, Accra, Mr. Hayford Asare, and Mrs. Victoria Asare for their assistance with the fieldwork. Lastly, to the numerous individuals and organisations who have worked with us to present our findings. We have been privileged to work with many dedicated professionals.
Ethical considerations
This study was ethically approved by the Committee on Human Research Publications and Ethics at the School of Medicine and Dentistry, Kwame Nkrumah University of Science and Technology (Ref. CHRPE/AP/331/25). The study was conducted in conformity with the Declaration of Helsinki of 1975 as revised in 2024. The manuscript formatting was guided by the STROBE guideline. 88 Permissions were obtained from the managers of the selected hospitals.
Consent to participate
Participants were provided with information on the purpose and nature of the study. Each participant signed an informed consent form before data were collected. All respondents’ details have been de-identified. In other words, the anonymity of respondents and confidentiality were ensured by keeping personal information safe on a computer secured with a password changed every 3 days. The principal investigator was the only researcher with access to respondents’ personal information. Consent was received from all participants prior to conducting this study.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data may compromise the privacy of study participants and are therefore only available upon request. Due to these conditions, interested researchers can access the underlying data by sending an e-mail request through the Committee on Human Research, Publication and Ethics, Kwame Nkrumah University of Science and Technology at (
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.