
Abstract
Background
Acquired immunodeficiency syndrome, caused by the human immunodeficiency virus, has remained a public health threat for the last decades with significantly high burden. Despite the introduction of various human immunodeficiency virus (HIV) prevention strategies targeting high-risk populations, including preexposure prophylaxis, there remains a notable gap in the literature regarding Pre-Exposure Prophylaxis (PrEP) practice among female sex workers (FSWs) in Ethiopia, particularly using advanced analytical methods like structural equation modeling. This study aimed to assess practice and associated factors of preexposure prophylaxis among urban female sex workers in Northwest Ethiopia.
Methods
A cross-sectional study was carried out at organizations of Organizations for Social Service, Health Development, Mehabere Hiwot for Social Development, and African Network for the Prevention and Protection Against Child Abuse and Neglect that serve FSWs. Systematic random sampling technique was employed among 549 FSWs. An interviewer-administered questionnaire was used to collect the data. Generalized structural equation modeling was employed to identify factors associated with PrEP practice. As the mediation of effects was present, the direct, indirect, and total effects were determined. A final model was selected based on the statistical significance of the path coefficient.
Results
In this study, the practice of preexposure prophylaxis was 28.00% with 95% CI = 25.34% to 32.72%. Thus, female sex workers with an education level of college and above had both direct and indirect positive effects on PrEP practice when mediated by knowledge, knowledge had both direct and indirect effects on PrEP practice when mediated by attitude. Whereas, FSWs who had duration of sex work for 3 to 5 years had only a positive direct effect on PrEP practice compared to those who were living in sex work for less than three years duration.
Conclusion
However, HIV remains a public health problem, and the practice of preexposure prophylaxis in this study was found to be low. FSWs having higher education levels, attitudes, and knowledge demonstrate a significantly positive effect on their likelihood to practice PrEP. They suggested enhancing their health outcomes and reducing the risk of HIV transmission. The result of this study was also significant for communities that are serving in a given organization targeting integrated HIV testing and counseling services among key populations.
Plain Language Summary Title
HIV Pre-exposure Prophylaxis Practice among Urban Female Sex Workers in Northwest Ethiopia: Using Generalized Structural Equation Modelling
Background
Acquired Immunodeficiency Syndrome, caused by the Human Immunodeficiency Virus, has remained a public health threat for the last decades with significantly high burden. Despite the introduction of various HIV prevention strategies targeting high-risk populations, including pre-exposure prophylaxis, there remains a notable gap in the literature regarding PrEP practice among FSWs in Ethiopia, particularly using advanced analytical methods like structural equation modeling. This study aimed to assess practice and associated factors of pre-exposure prophylaxis among urban female sex workers in Northwest Ethiopia.
Methods
A cross-sectional study was carried out at organizations of OSSHD, MSD, and ANPPCAN that serve FSWs. Systematic random sampling technique was employed among 549 FSWs. An intervieweradministered questionnaire was used to collect the data. Generalized structural equation modeling was employed to identify factors associated with PrEP practice. As the mediation of effects was present, the direct, indirect, and total effects were determined. A final model was selected based on the statistical significance of the path coefficient.
Result
In this study, the practice of pre-exposure prophylaxis was 28% with 95% CI = 25.34%, 32.72%. Thus, female sex workers with an education level of college and above had both direct and indirect positive effects on PrEP practice when mediated by knowledge, knowledge had both direct and indirect effects on PrEP practice when mediated by attitude. Whereas, FSWs who had duration of sex work for 3-5 years had only a positive direct effect on PrEP practice compared to those who were living in sex work for less than three years duration.
Conclusion
However, HIV remains a public health problem, and the practice of pre-exposure prophylaxis in this study was found to be low. FSWs having higher education levels, attitudes, and knowledge demonstrate a significantly positive effect on their likelihood to practice PrEP.
Background
Acquired immunodeficiency syndrome (AIDS), caused by the human immunodeficiency virus (HIV), is a major global public health issue (HIV), which has been a major global public health issue for the last decades persistently. 1 According to the World Health Organization (WHO) 2018 report, around 37.9 million people been reported to live with HIV/AIDS worldwide, of this 53% were key populations, including female sex workers (FSWs) and females accounted for 63% of all new HIV infections in 2020.2–4 In Ethiopia, the overall HIV prevalence among FSWs was 23% higher than the general population prevalence (0.9%).1,5 Female sex workers in low- and middle-income countries experience overlapping burdens of high HIV prevalence alongside high rates of sexually transmitted infections 6 since they are involved in sexual activity. These activities are exposed to HIV acquisition which is 21 times higher compared to the general population due to their vulnerability results of work-related risk factors.1,5
In Ethiopia, there are HIV prevention measures specially for high-risk populations such as condom use, health education, needle hygiene, combination prevention on adolescents and girls, combination prevention programs on key populations, and Pre-Exposure Prophylaxis (PrEP). 7 It is the use of ART medication by HIV-negative people to reduce the risk of acquisition of HIV infection. 8 Pre-Exposure Prophylaxis is freely available, a relatively new intervention being offered to FSWs and other populations with a high risk of HIV acquisition HIV. 6 It is classified as injectable, implantable, topical, and daily oral PrEP. Of these, daily oral PrEP is an effective for HIV prevention measures following the US Food and Drug Administration's approval of Truvada, a trade name of tenofovir disoproxil fumarate + emtricitabine. 9 In Ethiopia, PrEP is introduced in the national comprehensive HIV prevention, care, and treatment guidelines (2018-2020) following WHO's recommendation as an HIV prevention measure for HIV-negative FSWs and negative partners of discordant couples.1,12
While previous studies have identified sociodemographic and behavioral factors influencing PrEP practice, such as age, marital status, and stigma,10–14 there is limited empirical evidence addressing PrEP practices among FSWs in the study area, particularly using advanced analytical methods like structural equation modeling to capture the complex relationships between latent variables influencing PrEP uptake, allowing for a more nuanced understanding of these dynamics specific to FSWs. Therefore, this study aimed to assess PrEP practice and the factors associated with PrEP practice among urban FSWs in Northwest Ethiopia, using Generalized Structural Equation Modeling.
Methods
Study Setting, Design, and Period
The study was conducted at Organizations for Social Service, Health Development (OSSHD), Mehabere Hiwot for Social Development (MSD), and the African Network for the Prevention and Protection Against Child Abuse and Neglect (ANPPCAN). These are nongovernmental door funded organizations that serve integrated HIV testing and counseling intervention among key populations primarily for FSWs including; peer sessions, condom distribution, family planning, and sexually transmitted infection screening, 15 which are found in Gondar. Gondar is far about 727 km from Addis Ababa (the capital city of Ethiopia). According to the Central Statistics Agency population projection, the population of Gondar was estimated to be 360,600 in 2017. 16 In 2015, the estimated number of FSWs at Gondar was 4091. 17 This cross-sectional study was carried out from May 22 to June 28, 2022.
Populations
All urban FSWs who got service from OSSHD, MSD, and ANPPCAN health organizations in Gondar were the source population. Urban FSWs ≥18 years of age who got service from OSSHD, MSD, and ANPPCAN health organizations during the data collection period were the study population. Whereas those who were known as HIV positive (based on their records from the organizations) were excluded from the study.
Sample Size Determination
The number of free parameters that were obtained from published literature was taken into consideration when determining the sample size for generalized structural equation modeling. The minimal sufficient sample size for structural equation modeling was calculated using a rule of thumb, which was used to establish the sample size. 18 The proportion of cases to model parameters that need statistical estimates can be anywhere between 5 and 20 times the number of free parameters in the model that need to be estimated. 19 The required sample size to address the objectives of this study was calculated by the 1:10 ratio. 20 The lowest required sample size was found to be 561 when taking into account the 51 free parameters that need to be estimated and assuming a 10% nonresponse rate.
Sampling Procedure
In Gondar, three health organizations (OSSHD, MSD, and ANPPCAN) are found. These organizations were selected purposely because they delivered integrated HIV testing and counseling, and other SRH services for FSWs. Then to select samples from each organization, samples were proportionally allocated, which was estimated based on their average FSWs flow for HIV, STI, and SRH services in the months before data collection. Following the sample's proportionate distribution to each organization, 576 samples from OSSHD, MSD, and ANPPCAN were chosen using a systematic random sampling technique, with K = 3, 2, and 4, respectively. Ultimately, each organization's initial participant was chosen by a lottery method. After obtaining consent, the chosen respondents took part in the survey willingly (Figure 1).
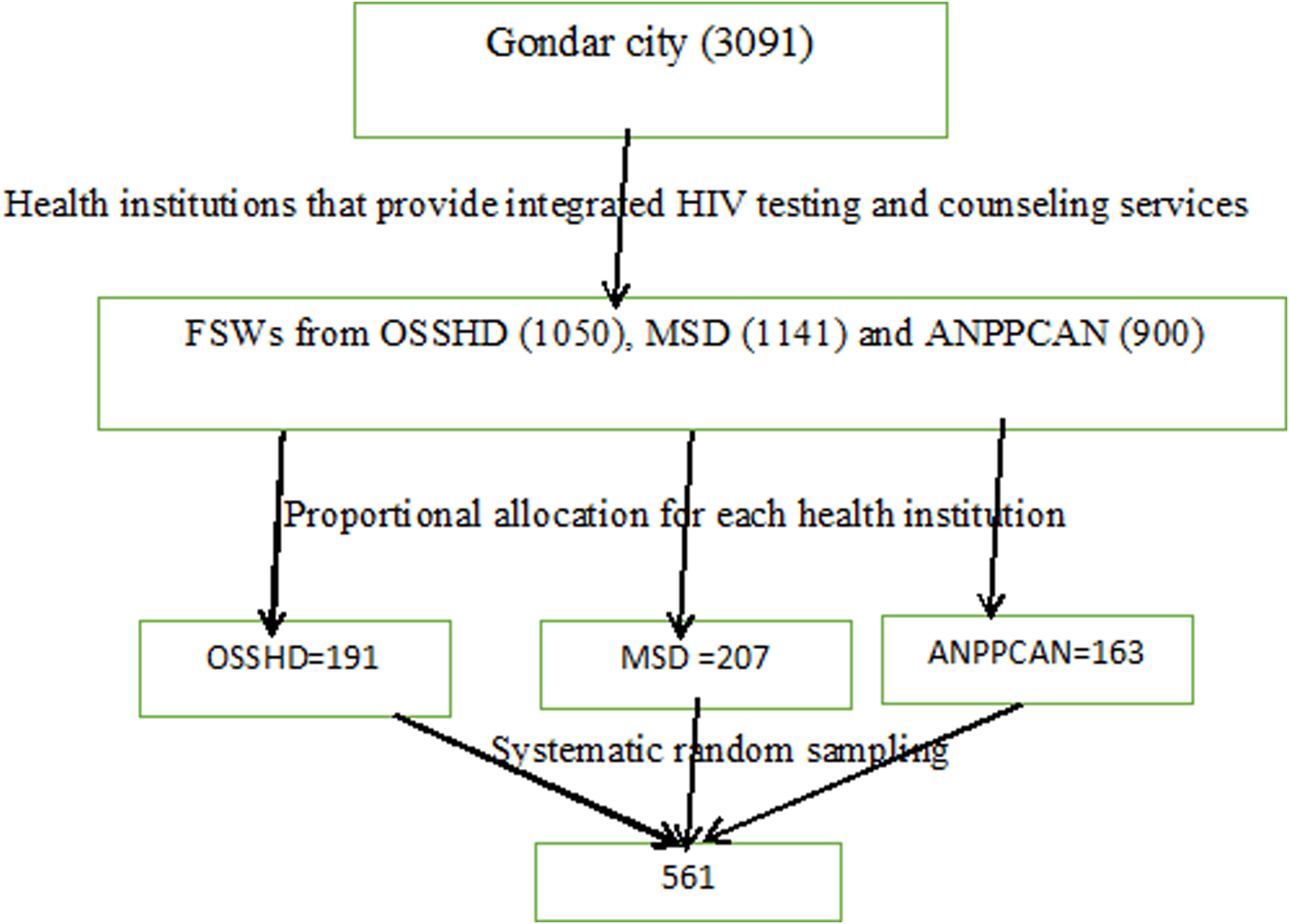
Schematic presentation of the sampling procedure used in the study conducted among urban female sex workers in northwest Ethiopia, 2022.
Operational Definitions
Pre-exposure prophylaxis practice: It was measured if the respondents answered “YES” to the question are you taking preexposure prophylaxis? And coded as “1.” Otherwise, the respondents answered “No” and coded it as “0.” 21
Knowledge: This was measured by 11 “Yes/No” questions of knowledge adapted from different literatures.12,22,23 If the study participants answered above the mean value (Mean = 4.84), he/she was considered as having adequate knowledge. Otherwise, if respondents answered below the mean value, he/she was considered as having inadequate knowledge.
Attitude: Assessed by 8 items using 5 response formats from strongly disagree (1) to strongly agree (5) adapted from previous literature. 23 Participants with scores above the mean value (>17.89) indicated favorable attitudes. Otherwise, an unfavorable attitude.
Sex work: Reported having had sex in exchange for money, goods, or services at any point in their lives. 14
Data Collection Tool and Procedures
Data were collected using an interviewer-administrated structured questionnaire designed to assess the practice of PrEP. The instrument was developed by reviewing different literature and modified to the local context. First, the questionnaires were prepared in English then translated into the local language Amharic and translated back to English to check the consistency by an independent translator. The questionnaire consisted of sociodemographic, knowledge, attitude, and PrEP practice-related questionnaires. The data were collected by four trained Bachelor of Science (BSc) Nurses and supervised by one Master of Science (MSc) nurse after training was provided. Data collectors were females to keep the gender match.
Data Quality Control
The Amharic version of the questionnaires was used to collect the data. To ensure the quality of data, pretests were done at Debark town on 29 study participants. Findings from the pretest were used in modifying the data collection tool. Supervisors and data collectors received two days of training covering the goal, the purpose, patient approach, confidentiality, and consent-taking techniques. The supervisor and lead investigator reviewed the completed questionnaires daily and weekly to ensure consistency and completeness. The data collectors were fluent in Amharic.
Data Processing and Analysis
The filled questionnaires were exported from the open data kit/ODK to STATA version 16 for cleaning, coding, and analysis. Descriptive and summary statistics were presented in the form of text and tables. Confirmatory factor analysis demonstrates items for latent variables significantly or insignificantly load the hypothesized factor structure to fit the data and to do structural equation modeling. Confirmatory factor analysis demonstrated knowledge indicators showed that all 11 items were significantly loaded and included from the instrument, for attitude; 2 items were excluded and 7 were included in the measurement using information criteria of AIC and BIC. Sample size adequacy was checked by Kaiser-Meyer Olkin, which was 0.87 and when its value is greater than 0.7 indicates a sizeable sampling adequacy. 24 The internal consistency reliability of the instrument was checked to show the internal homogeneity of items using Cronbach α, which was 0.88 for knowledge and 0.83 for attitude latent variables. The analysis was started with the hypothesized model, and modifications were performed iteratively by including mediator variables, if theoretically supported, and comparing the information criteria of each model fitted. The generalized structural equation model was employed to examine factors affecting PrEP practice. Therefore, when the mediation of effects was statistically significant, then the direct, indirect, and total effects were determined using the nonlinear combination of the estimator technique.
Results
Characteristics of Participants
The total sample size was 549 respondents who gave their consent to participate with a response rate of 98.00%. The mean age of the respondents was 27.40 years with a standard deviation of ±5.96. Regarding the reason the study respondents entered into sex work life; the majority were due to financial problems 358 (65.2%) (Table 1).
Sociodemographic and Other Characteristics of Urban Female Sex Workers in Northwest Ethiopia, 2022 (N = 549).a
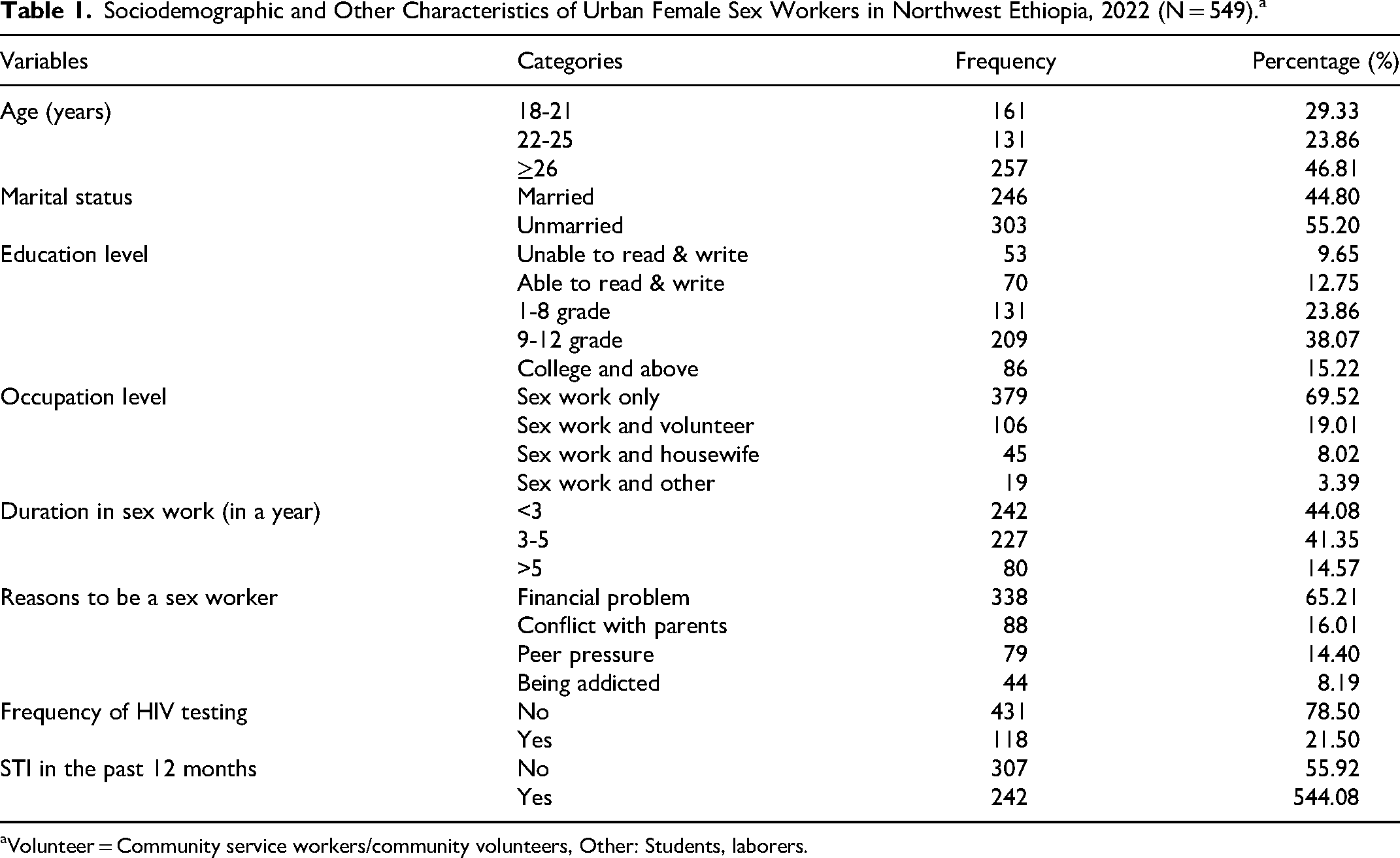
Volunteer = Community service workers/community volunteers, Other: Students, laborers.
Pre-Exposure Prophylaxis Practice among Urban FSWs
Among respondents, 158 (28.80%) with 95% CI = 25.34% to 32.72% were practiced PrEP. Among participants who did not utilize PrEP; 183 (47.00%) were due to stigma and 61 (16.00%) due to cost. Moreover, 25 (6.00%) were previous utilizers but stopped now; 22 (88.00%) were due to side effects (Table 2).
PrEP Practice among Urban Female sex Workers in Northwest Ethiopia, 2022 (N = 549).
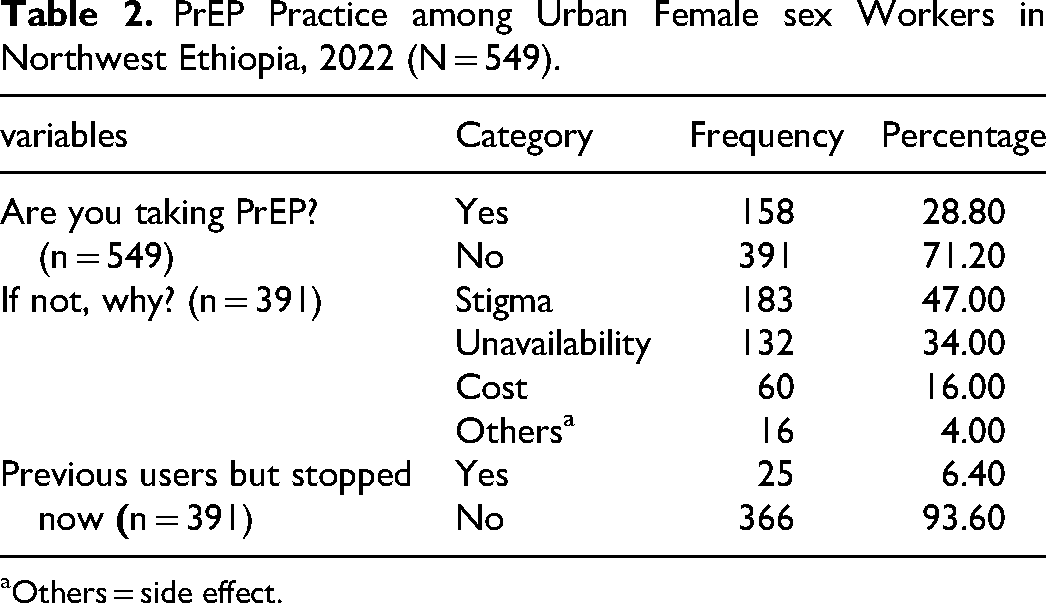
Others = side effect.
Factors Associated with PrEP Practice
In this study findings, study participants who had an education level of college and above had direct (adjusted β = 0.90, 95%CI = 0.42-1.38) and indirect (adjusted β = 0.24, 95%CI = 0.01-0.47) effects, resulting a total positive direct (adjusted β = 0.89, 95%CI = 0.52-1.08) effect on PrEP practice when mediated by knowledge as compared to, those who were unable to read and write. Knowledge had direct (adjusted β = 1.32, 95%CI = 0.41-1.53) and indirect (adjusted β = 0.62, 95%CI = 0.10-0.24), resulting in total positive (adjusted β = 1.94, 95%CI = 0.99-2.89) effect on PrEP practice when mediated by attitude as compared their counterpart. Moreover, those who had a duration of living in sex work between 3 and 5 years had a positive direct (adjusted β = 0.53,95%CI = 0.06-1.01) effect on PrEP practice as compared to those who are living in sex work less than 3 years (Table 3).
The Direct, Indirect, and Total Effects of Variables on PrEP Practice Mediated by Knowledge and Attitude among Urban Female Sex Workers in Northwest Ethiopia, 2022(N = 549).
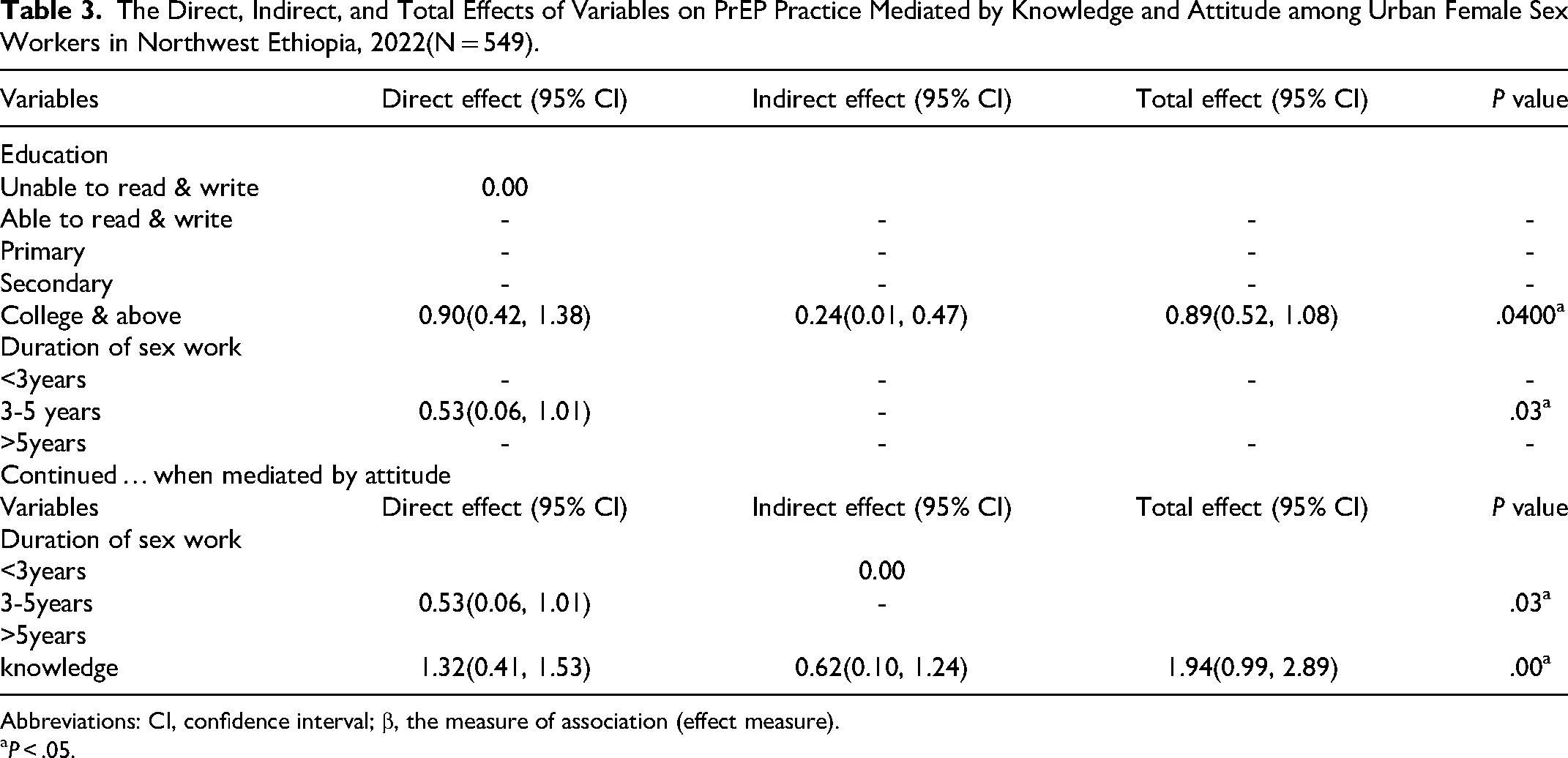
Abbreviations: CI, confidence interval; β, the measure of association (effect measure).
aP < .05.
Discussion
Pre-exposure prophylaxis is one of the prevention methods that were recently introduced in Ethiopia. It is a daily medication that can reduce the risk of sexually transmitted HIV infection more than 90%. 25
The study found that 28.00% of respondents practiced PrEP. This finding is higher than the study done in the United States showed that; PrEP was only (17.40%) 26 and the study done in Portugal was (0.40%). 27 This difference might be due to countries with more long-standing PrEP programs having higher PrEP practices. Among FSWs, who are not currently users, 183 (47.00%), were due to stigma. Stigma was found to be a barrier to PrEP use, as it can lead to unfavorable attitudes and judgments about FSWs using PrEP. 28 This finding is supported study in South India that revealed that the major obstacle (47.20%) for PrEP uptake was stigma 29 and from PrEP evidence; stigma influences by leading others to believe users are engaged in high-risk sex. 30 The study found that education level for college and above had direct, indirect, and total positive effects on PrEP practice when mediated by knowledge. This finding was supported by the study conducted in Portugal 27 revealed that education level at university was associated with the increased practice of PrEP. This might be due to increased educational levels make FSWs to communicate with regarding PrEP as HIV prevention. Moreover, knowledge had direct, indirect, and total positive effects on PrEP uptake when mediated by attitude. This finding was supported by a study done in Zimbabwe that revealed that more knowledge about PrEP moderately increased the likelihood of PrEP practice. 31 The duration of living in sex work for 3 to 5 years had a higher likelihood of PrEP practice compared to those with less than 3 years of experience. This suggests that experience and familiarity with the risks of HIV transmission may contribute to a greater acceptance and utilization of preventive measures. This finding is supported by the study done in Uganda showed that PrEP was significantly associated with those who were less than 5 years engaged in sex work than long duration in sex work. 32
Strengths and Limitations of This Study
This study assessed different factors for the practice of PrEP among FSWs, which provide updated information as the basis for future studies and may offer suggestions for strengthened PrEP education programs for FSWs. In addition, GSEM was used in this study, which allows for the effect of direct, indirect, and total effects of the independent variables’ respective effects on the outcome variable. However, the data were collected through a face-to-face interview, and this may be prone to social desirability bias and could be subjected to reporting errors, or there might be social desirability bias.
Conclusion
In this study, the practice of PrEP has many implications for policymakers and HIV/AIDS prevention and protection control programs to provide data on HIV prevention measures for FSWs. Female sex workers having higher education levels, PrEP attitudes, and adequate knowledge demonstrate a significantly positive effect on their likelihood to practice PrEP. They suggested enhancing their health outcomes and reducing the risk of HIV transmission. The result of this study is also significant for communities that are serving in a given organization targeting integrated HIV testing and counseling services among key populations.
Footnotes
Authors’ Note
Ethical Approval and Informed Consent: The Ethical Review Committee of the College of Medicine and Health Sciences, University of Gondar had secured the ethical clearance letter (approval #IPH2117). Written informed consent was obtained from all participants before inclusion in the study. The data were anonymized before analysis to protect patient confidentiality. Participants were created to declare that they have the right to withdraw from the investigation at any time without consequence. Availability of Data and Materials: All necessary data are included in this manuscript.
Acknowledgments
The authors would like to thank; the University of Gondar and the Institute of Public Health, department of Epidemiology and Biostatistics, the authors also thank the nongovernmental organizations (OSSHD, MSD, and ANPPCAN) branch managers, supervisors, data collectors, and study participants.
Authors’ Contribution
Conceptualization: LA and EG, data curation: LA, formal analysis: LA, investigation: LA and AG, methodology: LA and AG, software LA, validation: LA and EG, visualization: LA and TA, writing original draft: LA and TA, editing the manuscript. All authors contributed to the article and approved the submitted version accordingly based on the above descriptions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.