
Abstract
Infection with multiple pathogens concurrently has become less common since the introduction of potent antiretroviral agent and effective prophylactic agents. We describe a patient with pulmonary alveolar proteinosis (PAP) admitted with pneumonia who was found to have AIDS and diagnosed with Pneumocystis jiroveci pneumonia, human herpesvirus type 1 (HHV-1), and a concomitant cytomegalovirus viremia. Polymerase chain reaction viral load was used for diagnosis of HHV-1 and follow-up. The patient was treated with trimethoprim–sulfamethoxazole and ganciclovir and had a resolution of pneumonia. Since patients with PAP who are diagnosed as having AIDS could be concomitantly infected with multiple pathogens, rapid accurate diagnosis and treatment may have a positive effect on outcome.
Keywords
Introduction
Herpes simplex viruses (HSVs), Pneumocystis jiroveci pneumonia (PJP), and cytomegalovirus (CMV) infections are known opportunistic infections (OIs) associated with AIDS. Coinfection with multiple pathogens was commonly seen in the pre-highly active antiretroviral (pre-HAART) era. Due to effective prophylaxis and HAART, the incidence of OIs has considerably decreased in recent years. Herpes simplex virus infection in HIV-infected patients present mainly as meningoencephalitis or genital infections. Herpes simplex pneumonitis associated with HIV has been uncommonly described. High index of suspicion and use of polymerase chain reaction (PCR) can greatly enhance the diagnostic accuracy of this uncommon infection and lead to better outcome.
Case Report
A 52-year-old female recently diagnosed with pulmonary alveolar proteinosis (PAP) by lung biopsy was admitted with worsening dyspnea. The patient underwent a therapeutic total lung lavage as treatment for PAP. After the lavage, the patient developed worsening hypoxemia and was emergently intubated and transferred to the intensive care unit.
On physical examination, the patient had a temperature of 98.7°C, blood pressure of 100/68, pulse of 110/min, and a respiratory rate of 34/min. Cardiovascular examination revealed normal heart sounds. Pulmonary examination revealed crepitation in bilateral lung fields. The abdomen was soft without organomegaly, and the neurologic examination was unremarkable. Laboratory studies included white blood cell count of 9000 cells/µL, with 94% segs, 5% lymphocytes, and 1% monocytes; hemoglobin 13 g/dL; and platelets of 239 × 103/µL. Complete metabolic panel revealed a blood urea nitrogen of 16 mg/dL and creatinine of 0.37 mg/dL, with an estimated glomerular filtration rate >60; aspartate aminotransferase of 78 units/L, alanine aminotransferase of 187 units/L, alkaline phosphatase of 94 units/L, and lactate dehydrogenase of 530 units/L. Arterial blood gas prior to intubation revealed a pH of 7.5, P
A chest X-ray (CXR) revealed bilateral perihilar infiltrates. High-resolution computed tomography of the chest showed diffuse bilateral ground glass opacities with interlobular septal thickening (Figure 1). The patient was empirically started on cefepime and vancomycin for hospital-acquired pneumonia. Bronchoscopy with bronchoalveolar lavage (BAL) revealed sharp carina with no endobronchial lesions. There was no evidence of hemorrhage or necrosis. Minimal amount of secretions were noted. Blood and urine cultures were negative.

Computed tomography (CT) chest on admission.
Bronchoalveolar lavage cultures were negative for bacteria, mycobacteria, and fungi. Bronchoalveolar lavage respiratory virus PCR panel was positive for HSV-1 and an HSV PCR VL of 8 million copies/mL. The lung biopsy revealed multiple PJP organisms in the intra-alveolar space (Figure 2). In addition, the histopathology revealed intranuclear inclusion bodies and multinucleated giant cells consistent with HSV along with a positive immuno stain for HSV. A serum CMV PCR was 498 000 copies/mL. Serum HSV PCR VL was 97 copies/mL. There was no evidence of CMV pneumonitis on lung pathology.
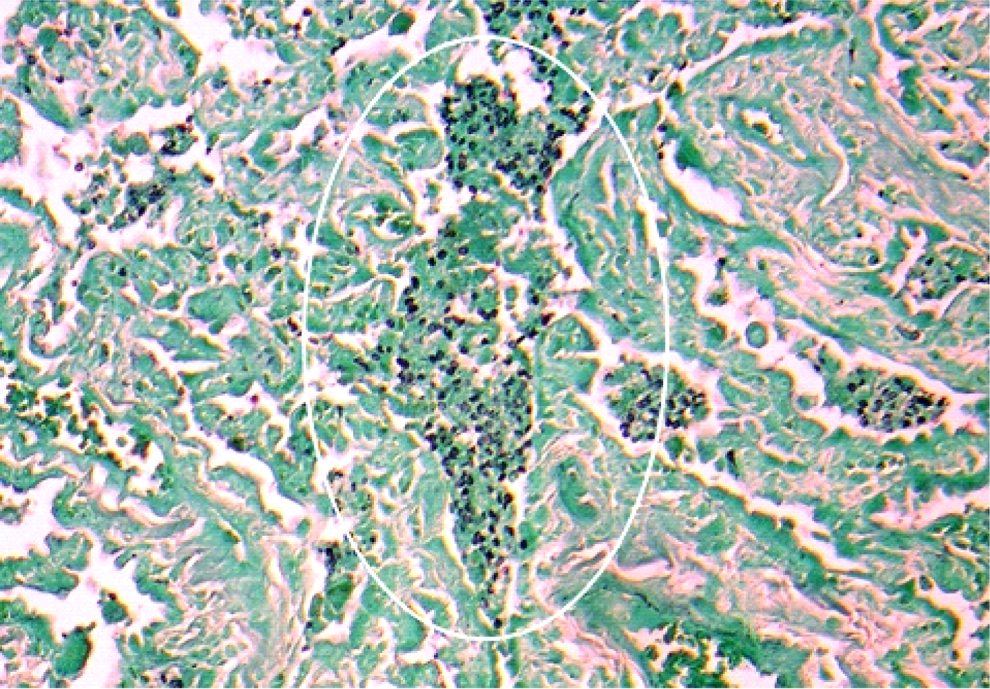
Histopathology consistent with Pneumocystis jiroveci pneumonia (PJP) on GMS stain. Abbreviation: GMS, Grocott’s Methanamine Stain.
Treatment was initially started with intravenous acyclovir 10 mg/kg in addition to trimethoprim-sulfamethoxazole (TMP/SMX) 15 mg/kg along with prednisone 40 mg 3 times daily. The patient was switched to ganciclovir at 5 mg/kg every 12 hours as induction therapy in view of CMV disease. Ophthalmologic examination and colonoscopy were deferred due to the patient’s clinical condition.
Over the course of 7 days, the patient continued to improve clinically with resolution of her lung infiltrates on repeat chest imaging and decreasing oxygen requirements on mechanical ventilation. The patient was extubated on day 8 of hospital stay. Repeat measurements of HSV showed complete resolution in serum and in BAL. One week after treatment initiation, there was a significant decrease in serum CMV levels to 4000 copies/mL.
The patient was discharged to a long-term rehabilitation facility 3 weeks after the initial diagnosis, with valganciclovir 900 mg oral daily and TMP/SFX prophylaxis (160/800) 3 times a week. A repeat CMV VL at the time of discharge was undetectable. The patient was seen in the outpatient HIV clinic 6 weeks after discharge when her CMV and HSV PCR continued to remain undetectable. She was initiated on emtricitabine/tenofovir and darunavir/cobicistat.
Discussion
Despite significant advances in diagnosis and management of HIV infection and OIs, underdiagnosis of HIV infection continues to be a clinical challenge and patients continue to present with undetected HIV infection and underdiagnosed OIs.
The HSV is a double-stranded DNA virus. It belongs to the family herpesviridae, subfamily Alpha Herpesviridae. There are 2 types of HSVs that cause infections in humans—human herpesvirus (HHV) 1 commonly associated with oropharyngeal and central nervous system disease and HHV-2 mostly associated with genital infections.
Dissemination of HSV infection generally occurs in patients with impaired T-cell immunity such as organ transplant recipients and HIV infection. The HSV pneumonitis is a relatively rare infection even in immunocompromised hosts. 1,2 Pathologically 3 patterns of HSV pneumonitis have been described—necrotizing tracheobronchitis, necrotizing pneumonia, and interstitial pneumonitis, the form most commonly encountered. Pathologically HSV interstitial pneumonitis is characterized by diffuse alveolar damage with lymphocytic infiltration, alveolar hemorrhage, and hyaline membrane formation. 3 -5
The HSV pneumonitis in HIV-infected patients has been described in 4 cases. 3,4,6 -8 Similar to our patient, these patients had a low CD4 counts <50 cells/mm3 and an HIV VL >50 000 copies/mL. 3,4,6,8 Three of the 4 patients were diagnosed with HHV-2 pneumonitis; the diagnosis was made on BAL with histopathology showing the typical HSV inclusion bodies. In difference to our case, quantitative HSV using PCR was not measured. Despite timely intervention, the 4 described patients had an unfavorable outcome, with death occurring in 1 week of starting treatment. Our case survived and was discharged from the hospital.
Pneumocystis jiroveci pneumonia remains the most common OI in patients living with HIV/AIDS having a CD4 count <200 cells/mm3. Bronchoscopy with BAL analysis is the gold standard for diagnosis. The treatment of choice remains TMP/SFX. 9 There is 1 case describing a coinfection of disseminated HHV-1 and PJP in an HIV-infected patient. 8 The patient had a CD4 count 10 -12 of 52 cells/mm,3 was admitted with shortness of breath, and was found to have interstitial pneumonitis on CXR and BAL specimen revealed PJP. The patient was started on TMP/SFX; and due to lack of clinical response to treatment, an endobronchial aspirate was performed. A qualitative HHV-1 DNA by PCR was found to be positive, and a quantitative HSV VL was not done. Whole blood samples were positive for HHV-1 by PCR. The patient however succumbed to his infection 3 weeks later. Our patient had PJP, which was diagnosed by BAL analysis, in addition HSV pneumonitis was diagnosed with both a quantitative HHV-1 PCR VL and stains showing the typical multinucleated inclusion bodies of HSV infection. Follow-up HSV VL showed a significant reduction from 8 million to 4000 copies/mL that paralleled the clinical response to treatment.
The CMV is a double-stranded DNA virus. It is a member of the family herpesviridae and is classified in the subfamily betaherpesviridae. The virus is designated human herpesvirus type 5 (HHV-5). The CMV disease in AIDS patients presents most commonly as retinitis, pneumonitis, or colitis. 10 Infection occurs typically in patients with a CD4 count of <100 cells/mm3. The quantitative CMV PCR is highly sensitive to CMV disease. 10 -12 El Amari et al 13 found that a value of >1000 copies/mL was associated with a 15-fold increase in the risk of CMV-related end-organ damage, an increased likelihood of AIDS-defining OIs and overall mortality. 9,13 The incidence of CMV viremia without end-organ damage is approximately 30%. 9
Our patient had a positive quantitative serum CMV VL PCR with a value of 498 000 copies/mL highly suggestive of active CMV disease. A BAL CMV PCR was negative for CMV and so were histological stains for the presence of CMV inclusion bodies, which essentially ruled out the diagnosis of CMV pneumonitis. The patient had no symptomatology suggestive of CMV colitis; neither did she have eye involvement to suggest CMV retinitis.
Pulmonary alveolar proteinosis is a diffuse lung disease characterized by accumulation of large amounts of proteinaceous material in the alveoli. 14 Pulmonary alveolar proteinosis can be congenital, idiopathic (also referred to as primary), or secondary when associated with systemic diseases most commonly seen with hematologic malignancies and HIV. 12,15,16
The association of PAP with HIV is well known and has been described in various case reports since the early 1980s. 17 -22 Decreased macrophage function appears to be a unifying feature of PAP. The altered immune function and opportunistic lung infections contribute to the alveolar lining breakdown, impaired clearance, and transudation of constituents of plasma into alveoli are thought to be contributing to the pathogenesis of PAP in HIV. 23
Conclusion
To our knowledge there are no reported cases of HSV pneumonitis in an HIV-infected patient with PAP. In summary, we have described the case of a patient with AIDS and PAP who had a concomitant PJP, HSV-1 pneumonitis, and CMV infection. The patient had a diagnosis of PAP, but her HIV status was not previously known. The case highlights several important clinical points. First, clinicians should be aware of the association between PAP and HIV infection; hence patients diagnosed with PAP should be tested for HIV. Second, patients who are newly diagnosed with HIV having a low CD4 count may be infected concomitantly with multiple pathogens clinicians should be aware of this and look for more than 1 pathogen. Multiple pathogens in a single patient were more commonly seen in the early years of the HIV epidemic; in recent years with the advent of HAART and better prophylactic agents, the overall incidence of OIs and concomitant infection with multiple pathogens has drastically been reduced. 24 Third, HSV pneumonitis can be a concomitant pathogen in patients with PJP, coinfection with this virus should be suspected and looked for especially in patients who do not respond well to anti-PJP treatment; to our knowledge, HHV-1 VL has not been utilized in BAL specimens of HIV-infected patients, we suggest that the test has the potential of being a useful tool in the diagnosis and management of patients with HSV pneumonitis. Fourth, CMV disease even without clear end organ involvement could be present and as suggested by Singh 25 could contribute to the state of immunosuppression, by a potential interaction of 2 viruses and potentiation of their pathogenicity. 26
Footnotes
Authors’ Note
Anita Bapat has done the case report and Eliahu Bishburg and Sandhya Nagarakanti helped in editing the case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.