
Abstract
Purpose:
To evaluate efficacy and safety of 20 000 IU cholecalciferol weekly in HIV-infected patients.
Methods:
Longitudinal data for 243 HIV-infected patients with paired 25-OH-vitamin D3 values for the same month in 2 consecutive years were stratified by the initiation of supplementation in this retrospective study.
Results:
After 1 year of administration of cholecalciferol 20 000 IU weekly, about 78% of patients with initial vitamin D level <20 µg/L achieved vitamin D levels >20 µg/L and 42% achieved levels >30 µg/L. Supplemented patients with baseline vitamin D levels <20 µg/L showed a significant risk reduction for hypocalcemia (P = .006; risk difference: 20.8%) and a significantly lower increase in alkaline phosphatase (AP) compared to those in the nonsubstituted group.
Conclusion:
The dose of 20 000 IU of cholecalciferol once weekly was found to be safe and effective. Normalization of vitamin D levels within 1 year was observed in 42% to 75% of the patients.
Introduction
HIV-infected patients are considered to have an even higher risk of vitamin D deficiency compared to the general population. 1 Although there are broad recommendations for vitamin D supplementation in HIV-infected patients at risk, 2 the route and strategy of supplementation remain unclear.
In order to promote medication adherence in patients with chronic disease, simple medication strategies with as little medication intake as possible seem to be favorable. Yet, higher risk of fracture in high-dose cholecalciferol formulation has been described. 3,4 Therefore, an intermediate formulation of 20 000 IU cholecalciferol once weekly might have major advantage: it provides a strategy of nondaily application without exceeding the recommended threshold of 4000 IU daily. 5
Despite evident advantages of the above-mentioned supplementation strategy, it has never been evaluated in HIV-infected patients. From today’s point of view, it seems unlikely that more data from prospective studies on this topic will be made available. We therefore retrospectively evaluated the safety and efficacy of supplementation with 20 000 IU cholecalciferol once weekly in a population of HIV-infected patients with low vitamin D levels (<30 µg/L). After 1 year, the changes in vitamin D levels compared to those in a nonsubstituted control group were analyzed. The safety end points were the occurrence of hypercalcemia (>2.65 mmol/L) as well as the vitamin D level of >80 µg/L as probably the highest level that can be achieved without supplementation and might be a threshold for toxicity. 6 –8 The secondary outcome parameters were changes in markers of bone turnover as well as changes in immunological and inflammatory surrogate markers.
Population and Methods
This retrospective analysis was performed at a single specialized HIV clinic in Munich, Germany. HIV-infected patients were screened for levels of vitamin D as part of routine clinical care, between January 2014 and January 2016. Patients with vitamin D data in the same month for 2 consecutive years were included. Patients receiving vitamin D supplementation at baseline, having baseline vitamin D levels ≥30 µg/L, and transsexual patients were excluded. Patient characteristics (sex, age, and antiretroviral therapy [ART]) and relevant laboratory parameters (25-OH-vitamin D3 [vitamin D], serum levels of calcium, phosphate, β-crosslaps, alkaline phosphatase [AP], creatinine, cystatin C, C-reactive protein, insulin, low-density lipoprotein and high-density lipoprotein cholesterol as well as erythrocyte sedimentation rate at 60 and 120 minutes, plasma glucose, and absolute and relative CD4 counts) as well as information on vitamin D supplementation were obtained from patient records. The decision for or against starting a supplementation with vitamin D was made by the corresponding treating physician of the patient at the center (10 different physicians). Patients with documented nonadherence to vitamin D supplementation (where prescribed) were excluded from the study.
Statistical analysis was performed using STATA SE 13.1 (StataCorp, College Station, Texas). Comparison of frequencies between the 2 groups was performed using Fisher exact test, and McNemar test was used for variable frequencies that changed during the course of the study. Comparison of continuous variables between both the groups was performed using the Mann-Whitney U test. For comparison of continuous variables within the groups (paired observations), Wilcoxon signed-rank test was used. P values <.05 were considered statistically significant. As a retrospective analysis of anonymized data, this study is free of ethics approval according to German regulations.
Results
Longitudinal data over 12 months for 243 patients were included; male sex was dominant (n = 197; 81.1%). The median age was 46.0 years. Eighty-six (35.4%) patients were started on supplementation of vitamin D with 20 000 IU cholecalciferol once weekly. The median time of supplementation at 12 months of follow-up was 11.0 months. The relevant laboratory parameters at baseline and after 12 months are presented in Table 1.
Comparison of Laboratory Parameters in the Entire Population and Per Group (Substituted Versus Nonsubstituted).a

Abbreviation: ns, not significant.
aThe data are expressed as the median (95% confidence interval).
Patients with Vitamin D Insufficiency
The subgroup of the patients with vitamin D insufficiency (20.0-29.9 µg/L) consisted of 63 patients (54 males [85.7%], median age 45 years). Of these, 12 (19.0%) patients started supplementation after initial testing, while 51 (81.0%) patients remained without supplementation. Median time of supplementation was 11 months.
The detailed laboratory results of this subgroup are presented in Table 2. The substituted and nonsubstituted patients did not differ in age (41 versus 46 years, respectively, P = .204) or sex (rate of male patients: 66.7% versus 90.0%, respectively, P = 0.058). After 1 year, 75.0% of the patients with the supplementation of vitamin D showed vitamin D levels ≥30 µg/L compared to 21.6% of the patients without supplementation (P = .001). The highest vitamin D level observed was 51.8 µg/L in the group of cholecalciferol-substituted patients (Figure 1).
Laboratory Results in the Subgroup of Patients with Vitamin D Levels between 20.0 and 29.9 µg/L.a
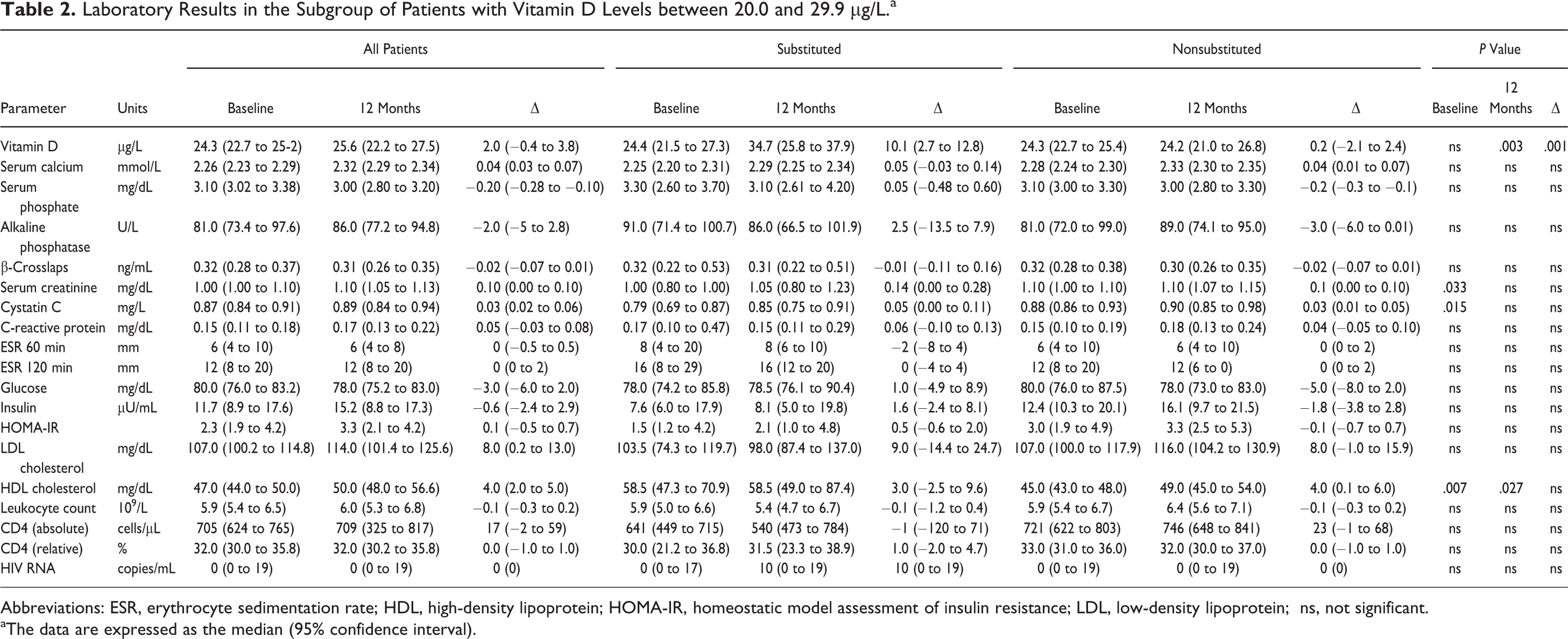
Abbreviations: ESR, erythrocyte sedimentation rate; HDL, high-density lipoprotein; HOMA-IR, homeostatic model assessment of insulin resistance; LDL, low-density lipoprotein; ns, not significant.
aThe data are expressed as the median (95% confidence interval).

Overview of changes in serum vitamin D levels (g/L) after a 12-month period in patients receiving substitution with 20 000 IU cholecalciferol and in nonsubstituted patients. No significant changes in the serum vitamin D levels were found in the nonsubstituted group. Significant changes in the vitamin D levels within a 12-month period were found in the substituted group. The data are expressed as the mean/interquartile range.
At baseline, 13 of the 63 patients, that is, 2 (16.7%) in the subgroup of cholecalciferol-substituted patients and 11 (21.6%) in the subgroup of nonsubstituted patients (P = 1.000), had calcium levels <2.20 mmol/L. After 12 months, 7 patients showed hypocalcemia, that is, 1 in the substituted group and 6 in the nonsubstituted group (8.3% versus 11.8%, respectively, P = 1.000).
Patients with Vitamin D Deficiency
The subgroup of the patients with vitamin D levels <20.0 µg/L consisted of 180 patients (143 males [79.4%], median age 47 years). Of these, 74 (41.1%) started supplementation after initial testing, while 106 (58.9%) remained without supplementation. Median time of supplementation was 11 months.
The detailed laboratory results for this subgroup are shown in Table 3. The cholecalciferol-substituted and nonsubstituted patients did not differ in age (47 versus 47 years, P = .491) or sex (rate of male patients: 81.9% versus 77.8%, respectively, P = .574).
Laboratory Results in the Subgroup of Patients with Vitamin D Levels Below 20.0 µg/L.a
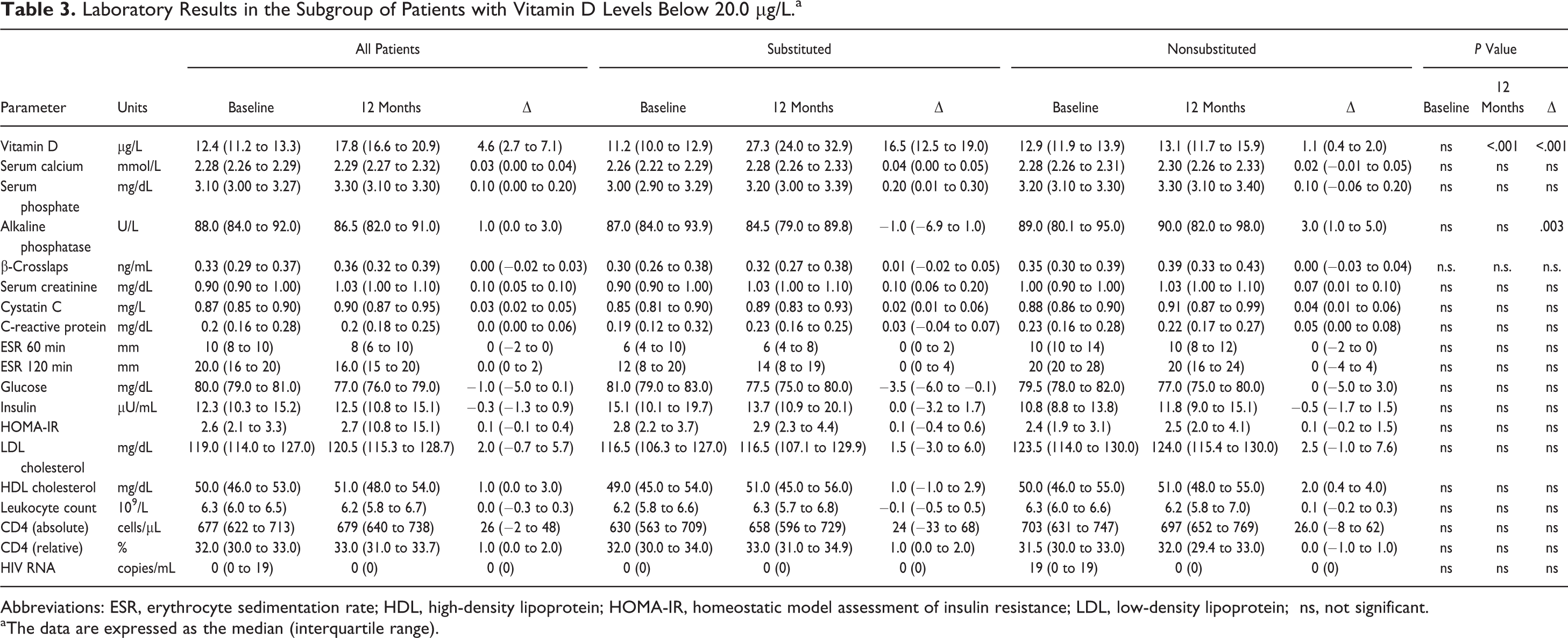
Abbreviations: ESR, erythrocyte sedimentation rate; HDL, high-density lipoprotein; HOMA-IR, homeostatic model assessment of insulin resistance; LDL, low-density lipoprotein; ns, not significant.
aThe data are expressed as the median (interquartile range).
After 12 months, 77.8% of patients on supplementation and 22.2% of patients without supplementation had vitamin D levels ≥20 µg/L (P < .001); 41.7% of substituted patients and 2.8% of the control population had values ≥30 µg/L (P < .001). The highest vitamin D level observed was 53.6 µg/L in the group of substituted patients.
At baseline, 40 (22.2%) of the 180 patients had a calcium level of <2.20 mmol/L. Hypocalcemia (<2.20 mmol/L) was prevalent in 22 of 74 patients (29.7%) and in 18 of 106 patients (17.0%) with and without vitamin D supplementation, respectively (P = .043). After 12 months, 21 patients had hypocalcemia, 14 in the nonsubstituted and 7 in the cholecalciferol-substituted group (13.2% versus 9.5%, respectively; P = .637).
The proportion of patients with calcium levels <2.20 mmol/L was significantly reduced after 12 months in the substituted group (P = .006; risk difference: 20.8%, 95% confidence interval [CI 95%]: 6.1%-35.5%) as compared to the nonsignificant change among the patients without supplementation (P = .481; risk difference: 3.7%, CI 95%: −4.8% to 12.3%).
Two cases of hypercalcemia (>2.65 mmol/L) were reported. Both were found in the group of patients without supplementation at baseline, and 1 of them persisted at 12 months.
Discussion
Bone health in HIV-infected patients has come to the fore in the recent years due to a noticeable risk of decreased bone mineral density and an increased incidence of fractures in this population. Both HIV itself and its specific antiretroviral drugs might contribute to this phenomenon, since some substances used in ART have a potential influence on different key mechanisms of bone turnover, for example, vitamin D metabolism, kidney function, and phosphate homeostasis. 9 –12
To the best of our knowledge, there is only 1 more recent study investigating cholecalciferol supplementation in a weekly dosing in HIV-infected patients, 13 whereas pulsatile cholecalciferol supplementation in HIV-infected patients has only been studied at frequencies of twice weekly on the one hand 14 or monthly or longer intervals on the other hand, until now. 15 –20
Our study population administered 20 000 IU cholecalciferol once weekly resulted in a median vitamin D level of 28.5 µg/L after 12 months. Therefore, this supplementation strategy not only was feasible and effective but also resulted in a favored vitamin D levels of about 20 to 40 µg/L, possibly with an optimum level of around 30 µg/L, 21 –24 regardless of the baseline levels.
Our cumulative dose of 80 000 IU of cholecalciferol per month equals an average daily intake of 2600 IU which is below the maximum recommended dose of 4000 IU daily in continuous therapy. 5 Nevertheless, vitamin D levels >30 µg/L were only achieved in about 75% of the patients with initial vitamin D levels of 20.0 to 29.9 µg/L and in 40% of the patients with initial vitamin D levels of <20 µg/L. In this context, a possibility of nonadherence to regular intake has to be discussed, since our cohort study failed to provide documented information about the adherence to cholecalciferol supplementation. Of note, only 3 patients in the subgroup of substituted patients did not demonstrate a raise in their vitamin D levels after 12 months.
Our data highlight a decrease in the serum AP concentrations in the cholecalciferol-substituted group versus an AP increase in the nonsubstituted group (P = .006). Since all the data were derived from routine testing, no data on bone-specific AP levels can be provided; however, a major contribution of vitamin D to this effect seems likely. Yet, the clinical relevance of these findings remains unclear.
We did not observe any medication-related hypercalcemia; only 2 patients with hypercalcemia after 12 months were already hypercalcemic at the baseline testing. The frequency of hypocalcemia increased significantly in the group supplemented with vitamin D. Although we do not advise patients on the use of supplemental calcium, we cannot exclude the possibility of intake of over-the-counter calcium supplements; however, we do not have any evidence of that in the relevant subsets of the patients.
For all other analyzed parameters of inflammation, immune system, and (bone) metabolism, no significant differences were found between the 2 study groups, cholecalciferol-substituted and non-substituted.
Our study has several limitations, first is the retrospective and nonrandomized design of the study. However, baseline characteristics, particularly median vitamin D levels, were comparable between the substituted and the nonsubstituted patients. Therefore, treatment by indication bias did not seem to have played a relevant role.
In the subgroup of patients with vitamin D insufficiency, a statistical difference in kidney function parameters between the patients who remained without supplementation and those with supplementation was found in the course of further follow-up. At the same time, a difference (that slightly failed to reach statistical significance) was found in the percentage of male patients. Therefore, the higher mean serum creatinine levels might reflect the higher number of male patients, since the normal range for serum creatinine is higher for Caucasian men compared to that of Caucasian women.
Vitamin D levels are known to show seasonal changes, which has to be taken into consideration for interpretation of these data. Yet, the use of matched pairs of data for the same month in 2 consecutive years together with the analysis of changes from baseline rather than absolute values in our cohort minimized the effect of seasonal influence.
We cannot provide data on adherence. Yet, our data clearly demonstrate that application of cholecalciferol once weekly does lead to a significant improvement in vitamin D levels in patients in a clinical setting.
Finally, we cannot provide information on changes in fracture risk as “hard” outcome parameter.
We summarize that a once-weekly administration of 20 000 IU cholecalciferol for patients with vitamin D levels <30 µg/L proved safe and effective. In about 75% of patients, vitamin D levels increased from <20 µg/L to 20 to 30 µg/L or from 20 to 30 µg/L to >30 µg/L. The treatment resulted in a significant decrease in AP levels, already occurring after 12 months, although the meaning of this finding is unclear.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.