
Abstract
Prompt antiretroviral therapy (ART) initiation after AIDS diagnosis, in the absence of certain opportunistic infections such as tuberculosis and cryptococcal meningitis, delays disease progression and death, but system barriers to inpatient ART initiation at large hospitals in the era of modern ART have been less studied. We reviewed hospitalizations for persons newly diagnosed with AIDS at Grady Memorial Hospital in Atlanta, Georgia in 2011 and 2012. Individual- and system-level variables were collected. Logistic regression models were used to estimate the odds ratios (ORs) for ART initiation prior to discharge. With Georgia Department of Health surveillance data, we estimated time to first clinic visit, ART initiation, and viral suppression. In the study population (n = 81), ART was initiated prior to discharge in 10 (12%) patients. Shorter hospital stay was significantly associated with lack of ART initiation at the time of HIV diagnosis (8 versus 24 days, OR: 1.14, 95% confidence interval: 1.04-1.25). Reducing barriers to ART initiation for newly diagnosed HIV-positive patients with short hospital stays may improve time to viral suppression.
Background
Prompt antiretroviral therapy (ART) initiation after AIDS diagnosis, in the absence of tuberculosis and cryptococcal meningitis, delays disease progression, reduces short- and long-term complications, decreases mortality, and reduces transmission. 1 –3 The AIDS Clinical Trials Group Protocol 5164, published over 5 years ago, showed starting therapy within 2 weeks of an opportunistic infection (OI) delays AIDS progression and death by 50%, compared to starting therapy within 4 to 10 weeks after an OI. 4 Yet, median time to ART initiation for HIV-infected adults receiving medical care in the United States has been estimated as long as 10 months, with even longer times to initiation for African Americans, women, and persons living at or below the poverty level. 5
Although prior studies have evaluated demographic, clinical, and behavioral reasons for delayed ART initiation, there has been less focus on system-level variables, such as facility-level operations and provider decision-making, associated with initial ART prescription. System-level barriers, however, may be as important as, if not more than, individual factors in the care continuum, and specifically in the process of initiating ART after an AIDS diagnosis. This is particularly relevant in the Southeastern United States where the HIV/AIDS burden has been recognized increasingly in the setting of larger sociocontextual issues. 6,7
Only recently have investigators begun to use implementation science to evaluate the process of initiating ART: where ART is initiated after diagnosis and how quickly this occurs. Researchers in Philadelphia found that persons diagnosed with HIV/AIDS in an inpatient facility were less likely to link to outpatient care than those diagnosed in other settings and subsequently less likely to start on therapy. 8 In qualitative studies, HIV-infected persons report that barriers to starting on HIV therapy include lack of provision of information about starting ART at the time of diagnosis in a hospital. 9,10 Furthermore, a study from Europe showed shorter time to ART initiation for HIV-infected persons diagnosed at their sites in France compared to their UK site, noting that patients in the French cities often had therapy started in the hospital compared to a deferral-to-the outpatient-setting strategy in the United Kingdom. 11
Given that system-level barriers can be changed, further studies are needed to identify modifiable causes of delayed ART initiation, particularly in the subset of patients with AIDS, in whom rapid progression to mortality is highest. Researchers in San Francisco demonstrated that a program targeting ART initiation in HIV-positive patients in community hospitals could increase ART initiation within 2 weeks of Pneumocystis jirovecii pneumonia (PCP) diagnosis from 50% to over 80%. 12
In the Atlanta metropolitan area, 20% to 50% of persons diagnosed with HIV have AIDS at diagnosis, and first contact with the medical system for these “delayed presenters” will often be a hospital admission. 13 Patients diagnosed with AIDS during hospitalization are a unique target for immediate ART because of ready access to expertise and services but also challenging because of coinfections and comorbidities, concern for drug interactions and absorption, and concern for follow-up and establishment of a long-term payer source. 2 In this study, our purpose was to characterize the prevalence of ART inpatient prescription and current patient- and system-level barriers to inpatient ART initiation for newly diagnosed HIV-positive patients in the hospital.
Methods
Study Setting
In the state of Georgia, Grady Memorial Hospital (GMH) is the largest hospital and is also serving as the public hospital for the city of Atlanta. In 2011, a total of 1141 HIV-infected patients were responsible for almost 2000 inpatient admissions at Grady. We reviewed medical charts from the outpatient GMH-affiliated HIV/AIDS clinic (the Ponce de Leon Center), the GMH emergency room and hospital visit records for each patient. The Ponce de Leon Center is the largest Ryan White–funded clinic in metropolitan Atlanta, which serves the majority of uninsured HIV-positive patients in the city.
Study Sample
All persons 18 years and older admitted to GMH with a new diagnosis of HIV infection either upon or during hospital admission from January 1, 2011, to December 31, 2012, were evaluated for 12 months following discharge, in this retrospective cohort study. Patients were eligible for the study if they were identified as newly diagnosed with HIV and had a CD4 count of
Variable Definitions and Data Collection Methods
Medical charts were abstracted for demographic and clinical information as well as system-level variables, including admission service and duration of hospital stay (days). The primary outcome was inpatient ART initiation (yes/no) defined by the prescription/listing of any antiretroviral (ARV) drugs on the discharge summary of the GMH hospitalization during which AIDS was first diagnosed.
Covariates from the chart review included demographics, insurance type, admission CD4 count and viral load, and OIs at presentation. Homelessness, comorbid mental illnesses, transmission category, and active substance abuse at the time of hospitalization were documented as reported by the inpatient primary care team, infectious disease consultants, or social workers in the medical chart. Renal dysfunction was defined as acute or chronic kidney disease, based on diagnoses and comorbidities listed in the admission history of present illness and discharge summary and/or a discharge serum creatinine >1.5 mg/dL. Admission service was medicine (eg general medicine, medical intensive care) versus surgery (eg, orthopedics, neurosurgery, surgical intensive care). Admission service was included in the analysis to evaluate how context may factor into hospital ART initiation. Electronic records for 1 year after diagnosis hospitalization were also reviewed to evaluate 3 outcomes: (1) time to linkage to care, (2) time to ART prescription, and (3) time to viral suppression. Time to linkage to care at an outpatient HIV clinic was defined as the number of days from the date of GMH discharge to the first outpatient clinic visit with an HIV medical provider. For those persons without any notes on linkage to care or laboratory data in the electronic medical chart, we cross-referenced our list with data from the Georgia Department of Public Health (GDPH) surveillance branch, to determine whether the patients pursued care in Georgia outside the GMH system. Per GDPH definition, persons who had a CD4 or viral load reported to the state through mandatory laboratory reporting procedures after the day of diagnosis were defined as “linked,” with the associated date of linkage recorded.
Time to ART initiation for those initiated at a GMH outpatient clinic during the study period was defined as days from the discharge date to the date of provider documenting the first ART prescription.
Time to viral suppression was defined as the number of days from the date of first positive HIV serology result in the hospital to the date of first plasma HIV RNA result showing an HIV viral load
The percentage of patients who linked to care in 90 days after diagnosis and the percentage of patients who achieved viral suppression within 12 months of diagnosis based on the above definitions were also determined.
Statistical Analyses
Fisher exact test was performed to determine the associations between categorical study variables and ART initiation, and Student t test or the Wilcoxon rank-sum test was used for normally distributed and nonnormally distributed continuous variables, respectively. Variables with test P < .10 were further studied in logistic regression models to estimate the odds ratios (ORs) for ART initiation prior to discharge. The software SAS 9.3 was used for all data analysis.
Ethics and Consent to Participate
This study was approved by the institutional review board of the Emory University (IRB00005499). Patient consent was not obtained as all data were collected retrospectively after routine medical practices and data were anonymized prior to analysis. There were no interventions or patient contact as part of this study.
Results
During the 2-year study period, 179 HIV-infected hospitalized patients were identified by the GMH social work team. Of these, 92 patients had newly diagnosed AIDS during hospitalization, and 11 patients were admitted with tuberculosis or cryptococcal meningitis, leaving 81 patients eligible for analysis (Figure 1). In our study sample, the majority were men (n = 66, 81%), African American (n = 65, 80%), and had a mean age of 42 years (Table 1). Additionally, most persons (n = 61, 75%) were uninsured, 24 (30%) had documented active substance abuse, 13 (16%) were actively homeless, and 9 (11%) had comorbid mental illness. Mental illnesses included major depression, bipolar disorder, and posttraumatic stress disorder. HIV-positive patients were generally US born (83%) and about one-third identified themselves as men who have sex with men. Over half (54%) had CD4 counts less than 50, median CD4 count was 36 (interquartile range [IQR]: 14-131), and median admission viral load was 260 000 copies/mL (IQR 101 000, 583 000).
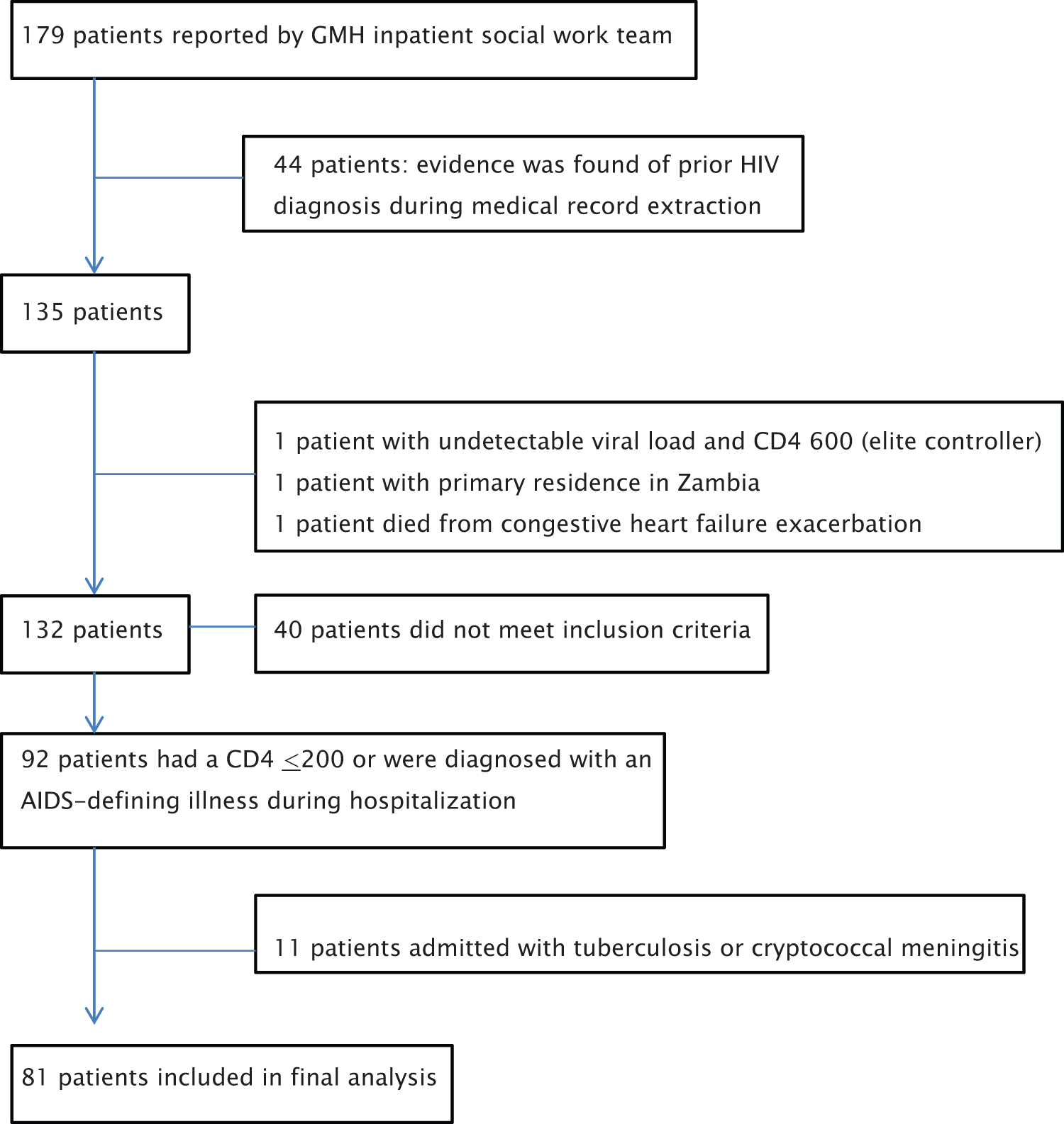
Derivation of the study population.
Characteristics of Persons Newly Diagnosed with AIDS, and Univariate Associations with Inpatient ART Initiation, Grady Hospital, Atlanta, Georgia, 2011 to 2012.a,b

Abbreviations: ART, antiretroviral therapy; IQR, interquartile range; PCP, Pneumocystis jirovecii pneumonia; SD, standard deviation.
an = 81.
bBoldface indicates statistically significant difference (P < .10).
cMedian (IQR) is reported for nonnormally distributed variables.
Forty-two (52%) had an OI during hospitalization, and 24 (30%) were admitted with PCP. Other OIs or AIDS-defining illnesses diagnosed during hospitalization were tuberculosis (n = 7), cerebral toxoplasmosis (n = 5), non-central nervous system (CNS) cryptococcus (n = 4), lymphoma (n = 4), esophageal candidiasis (n = 2), HIV encephalopathy (n = 2), disseminated Mycobacterium avium complex infection (n = 2), progressive multifocal leukoencephalopathy (n = 2), HIV wasting syndrome (n = 2), and cytomegalovirus (CMV) retinitis (n = 1). Almost a quarter (23%) of patients had renal dysfunction either at admission or during hospitalization.
Median hospital stay was 9 days (IQR: 5-17), and most patients were admitted to a medicine service (89%). In only 10 patients (12%), ART was initiated prior to discharge. Characteristics and inpatient ART initiation was similar among insured patients.
In general, demographic and behavioral characteristics were not associated with inpatient ART initiation. In univariate analysis, ART initiation in the hospital was associated with renal dysfunction, longer hospital stay, and admission to a nonmedicine service. In multivariable analysis, longer hospital stay was significantly associated with higher odds of an HIV-positive patient starting on ART in the hospital, including after adjusting for renal function (OR: 1.14, 95% confidence interval [CI]: 1.05-1.23). Inpatients who started ART prior to discharge had a median stay of 24 days (IQR: 20-36), compared to a median of 8 days (IQR: 5-13) for those who did not start ART during their hospital stay (P = .001).
Admission to a medicine service was associated with lower odds of an HIV-positive patient starting on ART in the hospital, including after adjusting for renal function (OR: 0.09, 95% CI: 0.01-0.58) or after adjusting for hospitalization duration (OR: 0.09, 95% CI: 0.01-0.81). The relationships between renal dysfunction and inpatient ART initiation was no longer statistically significant after controlling for hospitalization duration (Table 2).
Adjusted Odds Ratios Comparing Patient Characteristics with Inpatient ARV Drug Initiation.

Abbreviations: ART, antiretroviral therapy; CI, confidence interval.
aAdjusted for renal dysfunction.
bAdjusted for admitting service.
cAdjusted for hospitalization duration.
Over half of study patients linked to care within 3 months of discharge (54%), and median time to be seen in an HIV outpatient clinic for the entire cohort was about a month (38 days, IQR: 17-91; Table 3). There was a trend toward shorter time to linkage to care for those persons who started ART in the hospital compared to those who started ART outpatient, but this was not statistically significant. Antiretroviral therapy was ultimately initiated in 60 (74%) persons within 1 year of hospitalization, with 48 days (IQR: 20-87) of median time to ART from diagnosis. Persons who were initiated on ART in the hospital were started on ART sooner than persons who were initiated on ART outpatient (median 8 days versus 56 days, respectively, P <.001) and trended toward faster viral suppression (median 53 days versus 77 days, respectively, P = .7). Eighty percent of persons who started ART in the hospital achieved viral suppression at 12 months, compared to 56% of persons who started ART outpatient, but this was not statistically significant (P = .2).
Linkage to Care and Viral Suppression for AIDS Patients Diagnosed at Grady Memorial Hospital, by Inpatient ARV Drug Initiation.
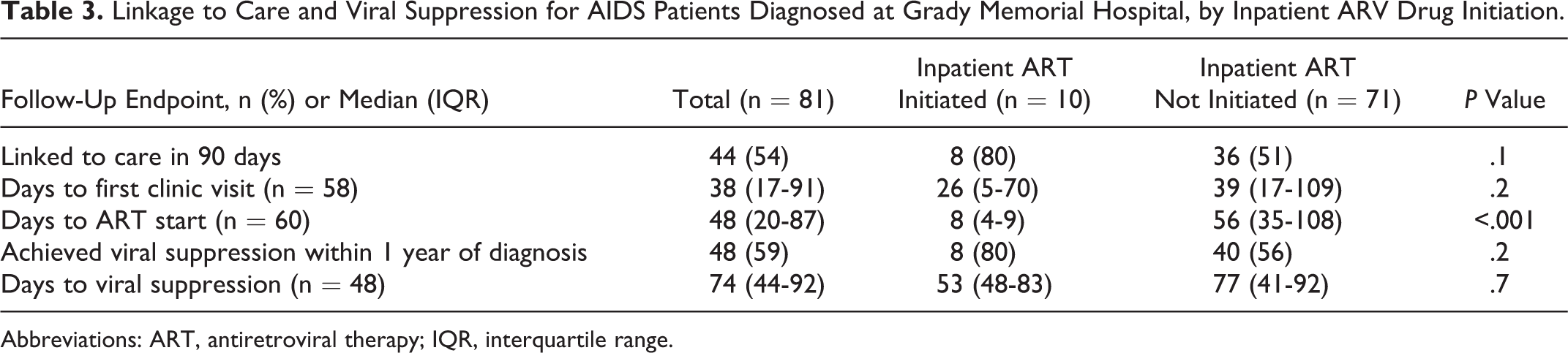
Abbreviations: ART, antiretroviral therapy; IQR, interquartile range.
Discussion
In this cohort of patients with AIDS at diagnosis, predominantly US born uninsured black men presented with multiple comorbidities. Initiation of ART at the time of AIDS diagnosis during hospitalization was infrequent, even when patients had no medical contraindication to starting therapy. The current literature includes only a few studies providing estimates of time to ART, 14 –16 and we are not aware of any US studies providing estimates of the proportion of HIV-infected persons, specifically diagnosed in a hospital setting who are initiated on ART prior to discharge.
The time to ART initiation for our overall cohort was 1.5 months, less than time to ART for HIV-infected persons with and without AIDS cited in other studies, 5 but greater than the target goal of less than 2 weeks to improve morbidity and mortality. Reasons for shorter time to ART initiation in our study sample may include the fact that outpatient referral from Grady Hospital is streamlined to a well-organized large Ryan White–funded clinic that is in close geographic proximity to GMH, and the clinic has a volume of HIV-positive patients cared for primarily by academic HIV providers who may be more likely than providers to implement guidelines recommending earlier ART initiation in other settings.
We suspected that coexisting renal dysfunction might be a reason that inpatients were not started on ART, given that tenofovir (TDF) is contraindicated in the setting of renal dysfunction and is a component of most first-line ARV regimens. Instead, we found a higher prevalence of kidney injury at admission for those started on ART prior to discharge than those not started on ART prior to discharge (50% versus 20%, P < .05), which on chart review appeared both related to the diagnoses of HIV-associated nephropathy motivating earlier ART initiation, and the fact that persons with kidney injury tended to stay in the hospital longer, until improvement and/or resolution of kidney injury was documented. Our analyses showed the relationship between kidney function and inpatient ART initiation was no longer statistically significant after adjusting for hospital duration.
We show that shorter hospital stay and admission to a medicine service was associated with lower odds of an HIV-positive patient starting on ART in the hospital, including after adjustment for renal function. These data suggest there may be an opportunity for guidance and/or resources to inpatient medicine providers to start ART during shorter hospital stays. Antiretroviral therapy initiation during longer hospital stays suggest that medicine providers may take a few days to think about starting ART in the hospital, seeing it as a “backburner issue,” may take time to identify a payer source for ART for insured patients, or only use ART as a “last resort” for critically ill patients in an attempt to facilitate discharge.
Identification of a payer source is also needed to ensure continuation of therapy after hospital discharge, and although both federally funded Ryan White programs and pharmaceutical assistance programs enable this, it may take time to ensure access in the hospital. Given that most of our patients were uninsured, it was difficult to characterize the lack of insurance as a reason for deferral of ART initiation at the time of diagnosis. Interestingly, of 20 insured patients in our study, less than a quarter were started on ART prior to discharge, suggesting that insurance status alone is not a primary factor in the decision to withhold ART in the hospital. A recent study of provider acceptance of early ART in the United States showed that 97% of providers disagree with a patients’ inability to pay for ART as a reason for deferring early ART, but physicians may be unaware of payer source options available to uninsured patients living with HIV/AIDS and/or their role in facilitating this process. 17
We identified trends toward faster linkage to care and viral suppression for patients started on ART in the hospital compared to their counterparts starting ART in the outpatient setting; these differences were not statistically significant but should be further evaluated in a larger study with a higher prevalence of inpatient ART initiation. Given that hospitals may be quick to recognize the costs of longer hospitalizations, these ought to be weighed against morbidity and mortality benefits for HIV-positive patients. Our study was limited by small sample size, retrospective nature, higher likelihood of type I error, and the fact that we did not capture patient willingness to start therapy. Furthermore, a future time to ART initiation Cox regression analysis would allow evaluation of additional time-varying covariates during hospitalization.
Prospective randomized control trials of systematic interventions that may facilitate inpatient ART initiation at the time of diagnosis are needed to characterize a causal, rather than associative, relationship and to justify potential large-scale policy interventions that could help us realize the mortality benefits for HIV-positive patients discovered in ACTG 5164.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.