
Abstract
We reviewed published national HIV care continua for men who have sex with men (MSM), people who inject drugs (PWID), and female sex workers (FSWs) to track progress toward the 90-90-90 target. We searched the Internet, PubMed, surveillance reports, United Nations Programme on HIV/AIDS country reports, US President’s Emergency Plan for AIDS Relief country/regional operational plans, and conference abstracts for the continua and graded them on quality. We found 12 continua for MSM, 7 for PWID, and 5 for FSW from 12 countries. HIV diagnosis, antiretroviral therapy coverage, and viral suppression varied between (1) 5% and 85%, 2% and 73%, and 1% and 72%, respectively for MSM; (2) 54% and 96%, 14% and 80%, and 8% and 68%, respectively for PWID; and (3) 27% and 63%, 8% and 16%, and 2% and 14%, respectively for FSW. Two countries, using data from national cohorts, were high quality. There are limited key population continua in the public domain. Of the few available, none have achieved 90-90-90. Improved monitoring and evaluation of key population continua is necessary to achieve the 90-90-90 target.
Keywords
Introduction
Since 2000, global efforts to scale up antiretroviral therapy (ART) have played a considerable role in halting and reversing the HIV epidemic in many settings. At the end of 2015, nearly 17 million people living with HIV (PLHIV) were on ART. 1 Recent scientific advances have demonstrated that immediate use of ART irrespective of CD4 count can reduce HIV-related morbidity, mortality, transmission, and costs. 2 -5 But for the benefits of immediate ART to be fully realized, PLHIV must optimally engage at each step along the “HIV care continua” (referred to as continua hereafter), 6 from early diagnosis to access to ART and viral suppression.
The continua have become vital tools to monitor the HIV programmatic efforts and guide future actions to achieve the 90-90-90 target by 2020 (which translate into 90% of the estimated PLHIV diagnosed, 81% of the estimated PLHIV on ART, and 73% of the estimated PLHIV virally suppressed along the continua). 7 As of 2015, only 60% of PLHIV globally had been diagnosed, ART coverage reached 46% and only 40% PLHIV were estimated to be virally suppressed. 1 There were an estimated 1.1 million AIDS-related deaths and 2.1 million new HIV infections, much higher than the target of fewer than 500 000 AIDS-related deaths and new HIV infections by 2020. 1 Achieving 90-90-90 within a short timeframe of 5 years and ending AIDS by 2030 will not be possible without addressing the HIV epidemic in key populations including men who have sex with men (MSM), people who inject drugs (PWID), sex workers, prisoners, and transgender that bear disproportionate burdens of HIV 8 -10 and account for 36% of new HIV infections. 1 In many countries, HIV care and treatment services for key populations are inadequate and of poor quality. 11,12 Discrimination, stigma, and lack of data regarding denominators are all obstacles to successful delivery of high-quality services.
Achieving 90-90-90 is vital for key populations to prevent illness, death, and transmission. Otherwise these hard-to-reach populations risk being among the 10% left behind as countries move toward achieving the 90-90-90 target for all PLHIV. To benchmark and assess progress toward the 90-90-90 target, this article reviews the published national continua for key populations (MSM, PWID, sex workers, prisoners, and transgender).
Methods
We searched the Internet, national surveillance reports, Joint United Nations Programme on HIV/AIDS (UNAIDS) country progress reports, 13 the US President’s Emergency Plan for AIDS Relief (PEPFAR) country or regional operational plans (COP/ROP) from 2016, 14 and conference presentations/abstracts for the most recent national HIV care continua, not older than 2010, for the following key populations—MSM, PWID, sex workers, prisoners, and transgender. We also searched PubMed to identify national continua for key populations. Key terms included “HIV or AIDS” and “cascade or continuum or continua or viral suppression or 90-90-90” and “key population or high-risk population or men who have sex with men or MSM or gay or people who inject drugs or PWID or injecting drug users or IDU or prisoner or sex worker or female sex worker or FSW or transgender.” We included continua that were (1) nationally representative, (2) officially reported, and (3) presented data on at least ART coverage and viral suppression. We excluded national continua that were old, missing data on ART or viral load or estimated number of a key population living with HIV, or were estimated using data from nonrepresentative research cohorts, cross-sectional studies, or respondent-driven sampling studies with varying geography and quality.
From the continua in the public domain, we collected data on the 4 key steps in the continua—(1) estimated number of a key population living with HIV, (2) number diagnosed as HIV-positive, (3) number receiving ART, and (4) number virally suppressed or with undetectable viral load (based on the threshold criteria for viral suppression reported by the country). We also determined the methods to derive these 4 indicators and graded them as high, medium, or low quality using the following criteria (described in detail in Supplementary Appendix Table 1). For the first indicator (estimated key populations living with HIV), data from national or UNAIDS estimates or nationally representative surveys and surveillance were considered high quality. Estimates based on subnational/subpopulation data were graded medium quality, whereas estimates from modeling studies were graded low quality. Data on indicators 2 to 4 (HIV diagnosis, on ART and viral suppression) collected directly from national cohort or national program service database were accorded high quality. Medium grade was given to these indicators if they were derived from population-based surveillance or subpopulation cohorts but did not directly measure program service delivery. Viral load suppression measured from a subsample of those on ART or the suppressed samples among all laboratory samples was also graded as medium quality. Low grade was given to these indicators if they were derived from data from a nonrepresentative selection of clinics and/or hospitals or if indicator 2 (HIV diagnosis) was not calculated.
The quality of the indicators was then applied to the continua—the continua were graded as high, medium, or low quality based on the lowest indicator grade. If source and quality of 1 indicator was unknown, the continuum was graded according to the quality of remaining 3 indicators. If source and quality of 2 or more indicators was unknown, the continuum was graded as ‘unknown’. Medium- and high-quality continua were considered “satisfactory” for monitoring the response for key populations.
Results
The public domain search yielded 25 sources of key population continua (PEPFAR COP/ROP, surveillance reports, and presentations). The PubMed search located 388 studies, of which 34 studies included key population continua (Figure 1). Of these 59 sources, 27 were excluded as they were constructed using cross-sectional surveys, respondent-driven sampling, or clinical/program/cohort data that were not geographically representative. Nine others were excluded as they represented subnational continua and were also missing data on estimated number of key population living with HIV or ART coverage. From the remaining 23 sources for national key population continua, we excluded 13 that were missing data on viral suppression (n = 5), lacked estimate for a key population living with HIV (n = 5), used data from nonrepresentative research cohorts (n = 1), presented old data (n = 3), and/or were constructed using estimates from studies with varying geography and quality (n = 1) with some studies excluded for more than 1 reason (see Supplementary Appendix Table 2 for excluded studies).

Methods describing the selection process for HIV care continua for key populations. COP/ROP indicates country or regional operational plan; FSW, female sex workers; MSM, men who have sex with men; PEPFAR, The US President’s Emergency Plan for AIDS Relief; PWID; people who inject drugs.
In total, we found 12 national continua for MSM, 7 for PWID, 5 for FSWs, and none for transgender and prisoners from 12 countries published between 2010 and 2016 from 10 sources. 15 -24
Continua for MSM
According the latest continua, none of the 12 countries have achieved the 90-90-90 target for MSM while 4 countries (Denmark, France, the Netherlands, and United Kingdom) are within 20% of achieving the target for MSM. Among the estimated MSM living with HIV, HIV diagnosis, ART coverage, and viral suppression varied significantly between 5% to 85%, 2% to 73%, and 1% to 72%, respectively (Table 1).
HIV Care Continua for Key Populations from 12 Countries, 2010 to 2016.a
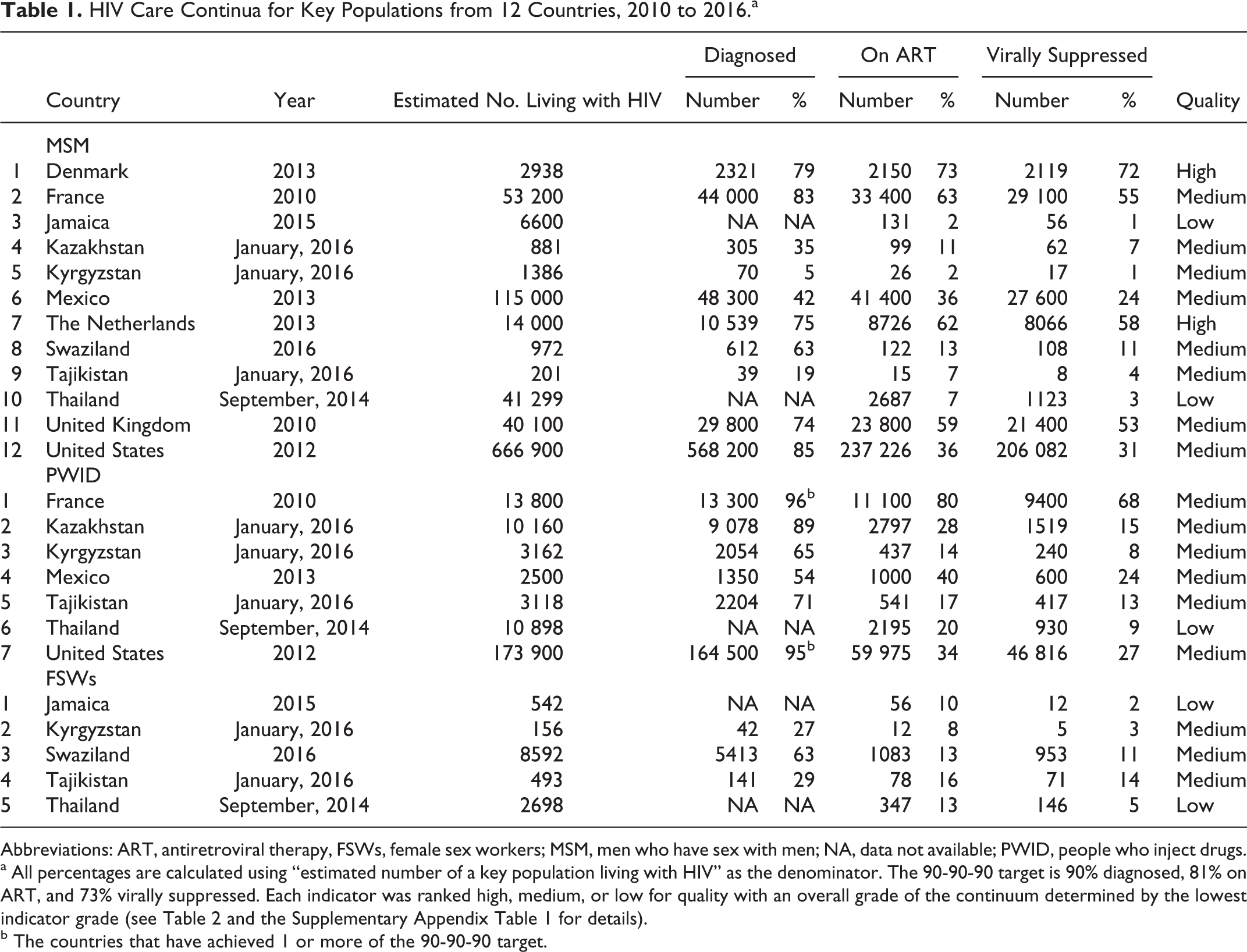
Abbreviations: ART, antiretroviral therapy, FSWs, female sex workers; MSM, men who have sex with men; NA, data not available; PWID, people who inject drugs.
a All percentages are calculated using “estimated number of a key population living with HIV” as the denominator. The 90-90-90 target is 90% diagnosed, 81% on ART, and 73% virally suppressed. Each indicator was ranked high, medium, or low for quality with an overall grade of the continuum determined by the lowest indicator grade (see Table 2 and the Supplementary Appendix Table 1 for details).
b The countries that have achieved 1 or more of the 90-90-90 target.
Continua for PWID
Only 2 countries (France and United States) of 7 have achieved the first 90 target for PWID (ie, >90% PWID living with HIV diagnosed), whereas no country has achieved the second or the third 90 target according to their latest continua. France, with ART coverage of 80% and viral suppression of 68% among PWID in 2010, has likely achieved 90-90-90 already. Among the estimated PWID living with HIV, HIV diagnosis, ART coverage, and viral suppression varied between 54% and 96%, 14% and 80%, and 8% and 68%, respectively.
Continua for FSW
None of the 5 countries have achieved or are close to achieving the 90-90-90 target for FSW. Among the estimated FSW living with HIV, HIV diagnosis, ART coverage, and viral suppression were low and varied between 27% and 63%, 8% and 16%, and 2% and 14%, respectively.
Among the different key population groups, progress toward the 90-90-90 target for FSWs was the poorest. HIV diagnosis, ART coverage, and viral suppression for MSM and PWID in European countries (Denmark, the Netherlands, United Kingdom, and France) were comparatively higher and they are likely to achieve 90-90-90 for MSM and PWID well before 2020. The rates of HIV diagnosis were high (>85%) in Kazakhstan (for PWID) and United States (for MSM and PWID); however, access to ART and viral suppression were relatively low (<40% and <35%, respectively).
Continua from 2 countries (Denmark and the Netherlands) used data from national cohorts, which include all people diagnosed with HIV, to determine the number diagnosed, on ART, and with viral suppression and were ranked as high quality (Table 2). Continua for key populations from 8 countries were of medium quality. Of these, 5 countries were using program data for number of key populations diagnosed and/or on ART but used viral load suppression estimates to calculate the number of PLHIV on ART with viral suppression. Three countries with medium quality did not rely on program data for ART coverage—France used large cohort data, representing 50% of key population in care, to bootstrap estimates for national continua for key populations, and United Kingdom and United States used estimates from their surveillance systems. Continua from two countries (Jamaica and Thailand) lacked data on number of key population living with HIV diagnosed and were graded low quality.
Methods for Calculating the 4 Key Steps in the HIV Care Continua for Key Populations in 12 Countries.a
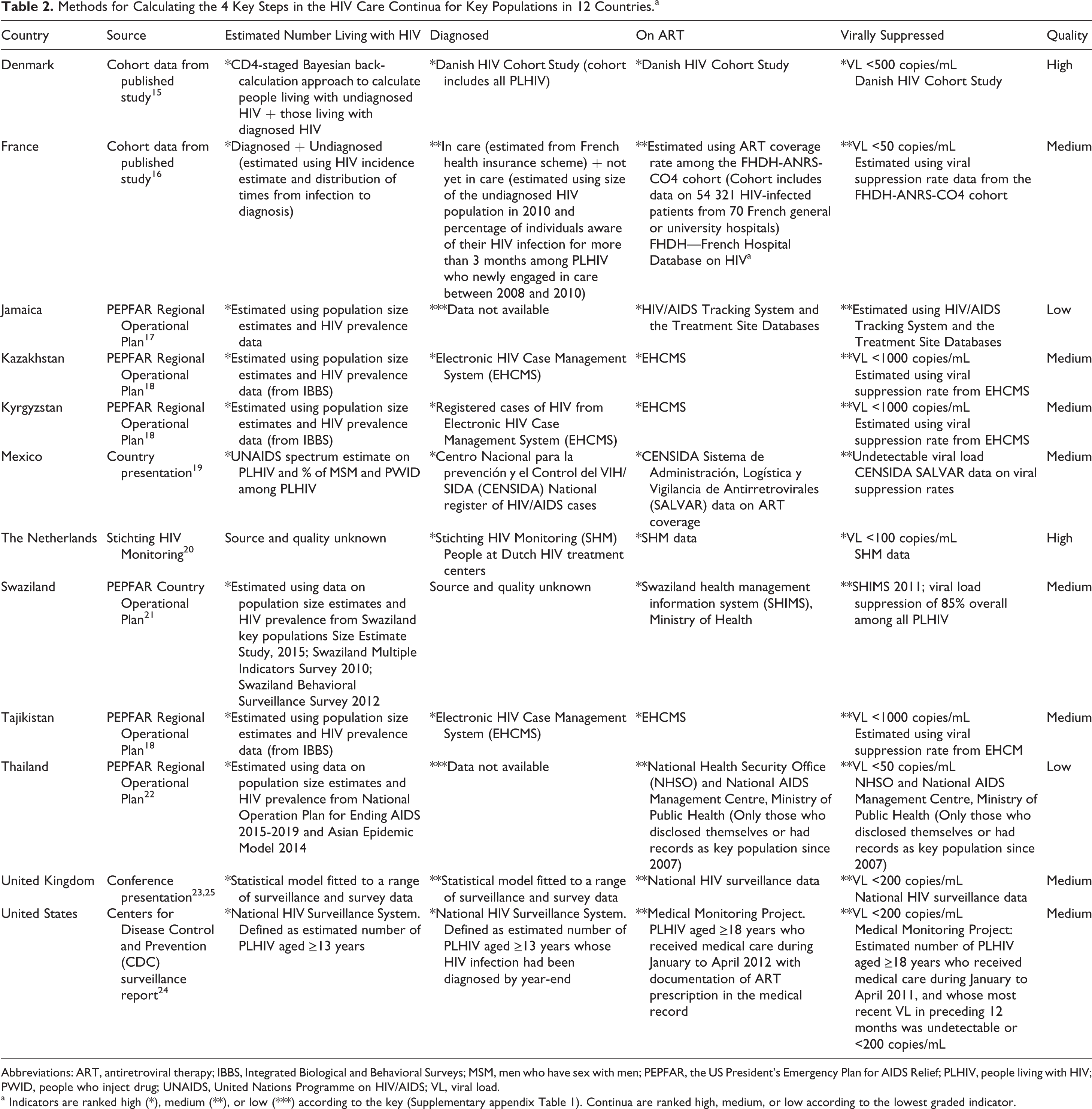
Abbreviations: ART, antiretroviral therapy; IBBS, Integrated Biological and Behavioral Surveys; MSM, men who have sex with men; PEPFAR, the US President’s Emergency Plan for AIDS Relief; PLHIV, people living with HIV; PWID, people who inject drug; UNAIDS, United Nations Programme on HIV/AIDS; VL, viral load.
a Indicators are ranked high (*), medium (**), or low (***) according to the key (Supplementary appendix Table 1). Continua are ranked high, medium, or low according to the lowest graded indicator.
Discussion
The HIV response for key populations, including MSM, FSW, PWID, prisoners, and transgender, will play a central role in ending the AIDS epidemic by 2030. Although overall diagnosis, treatment, and sustained viral suppression are now estimated to be moving toward 90-90-90 in many settings, it is not clear whether highly marginalized communities are benefiting from this expansion of HIV services. 25 Thus, it is important to systematically collect, analyze, and publically disseminate HIV-related data on the continua for key populations. Such data will not only help benchmark the current efforts but also drive decisions and investments in the future to optimize program efficiency and sustainability for communities that have traditionally been neglected. Despite a comprehensive search for national continua for key population, we found continua for MSM, PWID, and/or FSW from only 12 high- and middle-income countries primarily in Western Europe and North America, and we found 1 continua (Swaziland) from sub-Saharan Africa that bears the brunt of the HIV epidemic. Continua for these key populations from low-income countries or for prisoners and transgender were not available.
Even though considerable efforts and investments have been made to improve monitoring and evaluation (M&E), epidemiological data on key populations are still insufficient. In many settings, stigma, discrimination, and punitive laws discourage health authorities, providers, and the community from collecting and disclosing information. Already marginalized and vulnerable communities lack the trust necessary to report same-sex behaviors, drug use, or involvement in sex work. The stigma and lack of trust compromise the successful implementation of HIV programs including M&E of progress toward 90-90-90. Specifically, the UNAIDS Global AIDS Response Progress Reporting 26 does not collect and report data on the programmatic indicators disaggregated by key populations. From our review of public domain information, it appears that most countries mirror this “don’t ask, don’t tell” approach to monitoring access to HIV diagnosis and treatment among key populations.
Although the number of available key population continua is limited, none of the countries in our review have achieved the 90-90-90 target for any key populations. There are differences in the progress toward the target among countries and different key population groups. Overall, rates of HIV diagnosis, ART coverage, and viral suppression are relatively higher for MSM and PWID compared to FSW. European countries (France, the Netherlands, Denmark, and United Kingdom) are reporting more than 53% viral suppression rates for MSM and PWID and will achieve 90-90-90 for them before 2020. It is unlikely that most of the countries without publically available national continua for key populations have achieved 90-90-90 for them since none of the countries (except Sweden) have achieved 90-90-90 for all PLHIV. 25 Stigma, discrimination, violence, and criminalization of same-sex relations, sex work, and drug use often disrupt access to and retention in HIV services, leading to suboptimal outcomes along the continua. 27 -29 Also, besides the 33 countries that recommend “test and treat” for all PLHIV in line with the World Health Organization 2015 guidelines, 30 only 10 other countries have specifically recommended fast-tracking key populations for immediate ART irrespective of CD4 count. 31
The countries that have continua for key populations use different methods to calculate the outcomes along the continua. Thus, caution is required while interpreting the results and comparing the 90-90-90 estimates across countries. Of the 12 countries, only 2 countries had high-quality data from national cohorts, which include all people diagnosed with HIV, to determine 90-90-90 for key populations. For estimating the number of key population living with HIV, most countries depended on modeled key population size estimates from UNAIDS Spectrum and HIV prevalence data among key populations from Integrated Biological and Behavioral Surveys, which are usually not nationally representative. Estimating the number diagnosed is the most challenging for countries—while some do not present data on this indicator, others rely on aggregate data on HIV tests done, modeling, or surveys. The majority used national program data to report on the number on ART and viral suppression rate among all laboratory samples to estimate number on ART with viral suppression. Countries need to prioritize national cohort databases to track progress toward 90-90-90 and should use the current methods to approximate HIV diagnosis, ART coverage, and viral suppression among the key populations in the interim.
This review has some limitations. We only included the most recent published national care continua for key populations in the public domain. We did not contact the health authorities or researchers for missing/updated continua or construct them using data from different published sources. Despite a comprehensive search methodology, we might have missed some continua or more detailed methodology used to construct them. Also, this study only looks at the most recently published continua and does not track the progress toward 90-90-90 over time. Some of the continua are as old as from 2010. Since then, the HIV-related policies, laws, and investments have changed in many countries. Finally, this study did not review the numerous subnational surveillance reports for continua for key populations from states/provinces and cities or present stratified care continua for key populations (ie, by age or ethnicity or disease such as tuberculosis or hepatitis C). Such data will better highlight the heterogeneity of the HIV epidemic within countries and communities.
Conclusion
Even though a few countries are close to achieving the 90-90-90 target for select key populations, data in the public domain are limited and much needs to be done to achieve the target in countries with a high HIV burden and limited resources. HIV care programs specifically tailored for key populations, which include community-based HIV testing and immediate access to ART and viral load monitoring, need to be scaled-up in partnership with civil society organizations. This will not be possible without addressing the social and legal barriers impeding access to care for key populations. Additionally, more and better quality data on key populations are needed in the public domain to promote accountability and data-driven programs. Countries and organizations working with key populations need to strengthen their current M&E systems so that more real-time, local, and disaggregated programmatic data can be collected, and continua can be standardized across countries. Investment in population-based surveys, targeted surveys in areas with high HIV prevalence among key populations, case-based reporting, and unique identification codes can help countries construct more reliable continua for key populations. 32 Community engagement will be critical in both design and implementation of M&E activities to ensure a human rights framework is followed, and that both communities and health authorities can own the data and work together to improve access to diagnosis and treatment.
Footnotes
Authors’ Note
The findings and conclusions in this study are those of the authors and do not necessarily represent the views of IAPAC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.