
Abstract
This is a retrospective cohort study of 352 newly diagnosed HIV-infected individuals in Denver, from 2005 to 2007. Utilizing data from 3 health care systems, 2 clinical trials units, and statewide Colorado HIV laboratory reporting databases, we tracked initial linkage to HIV care, retention in care, loss to follow-up, and transitions between HIV care providers. After more than 2.6 years of follow-up, 256 (73%) individuals linked to HIV care within 180 days. Of the 301 individuals who eventually linked to care, 168 (56%) had at least one 180-day gap in care, while 49 (16%) had a 360-day gap. Transitions in care were common, with 131 (37%) individuals accessing care from 2 different providers and 15% having evidence of living outside of Colorado. In this newly diagnosed HIV-infected cohort, linkage to care was slow and long-term retention in care was poor. Transitions between HIV care providers were common and may impair engagement in care over time. Out-of-state migration was frequent and may cause an underestimation of engagement in care.
Introduction
Inadequate antiretroviral (ARV) medication adherence and ARV resistance have long been considered the major barriers to the successful management of HIV infection. 1 Over the past decade, antiretroviral therapy (ART) has become more forgiving to lower levels of adherence. 2,3 New ARV agents and ARV medication classes have made ARV resistance a less common cause of HIV disease progression. 4 Today, poor engagement in HIV care is increasingly recognized as a major barrier to improved treatment outcomes in HIV-infected individuals. 5 Delayed linkage to care and inadequate retention in care are associated with HIV disease progression, new or recurrent opportunistic illnesses, and mortality. 6 –9 Poor engagement in HIV care also represents a formidable barrier to the effective implementation of “test and treat” strategies for HIV prevention. 5
In prior studies, linkage to and retention in HIV care have commonly been assessed separately, with few studies utilizing individual-level data to assess the progression from HIV diagnosis through linkage to care and subsequent retention in care. Individual-level data facilitates an analysis of transitions in HIV care between HIV providers, which may significantly contribute to poor engagement in care. Our goals were to describe engagement in HIV care and transitions in care between HIV providers in a newly diagnosed HIV-infected cohort in Denver, Colorado.
Methods
Study Population
Denver Public Health is located within Denver Health, an integrated safety net health care system serving approximately 1600 HIV-infected individuals annually. 10 In Colorado, each year, approximately 30% of new HIV diagnoses are made through Denver Health. A comprehensive effort was made to identify all newly diagnosed HIV-infected individuals within Denver Health from 2005 through 2007 utilizing sexually transmitted disease (STD) clinic HIV-testing data, outreach HIV-testing data, Denver Health clinical laboratory results, and a database maintained by our HIV linkage-to-care program at Denver Public Health.
Evidence of HIV infection required (1) a positive HIV Western blot or (2) a positive HIV antibody test in conjunction with a detectable HIV-1 viral load. Individuals with prior HIV-positive testing were excluded; they were identified via surveillance records at the Colorado Department of Public Health and Environment (CDPHE). Individuals who tested anonymously were excluded unless they provided identifying information after testing positive. Children 13 years of age or older, pregnant women, and prisoners were included. This study was approved by the Colorado Multiple institutional review board, the CDPHE institutional review board, and the US Office for Human Research Protections.
Data Abstraction and Definitions
Full medical records were reviewed at Denver Health, the Denver Metro Health (STD) clinic, the University of Colorado Hospital, the Children’s Hospital Denver, and the local sites of 2 HIV clinical trial units. In Colorado, during the study period, all CD4 counts <500 cells/mm3 and detectable HIV-1 viral loads were required to be reported to CDPHE by the performing laboratory. Despite the fact that undetectable viral loads were not reportable, most laboratories reported these results. We had access to all viral loads for 8 of 10 laboratories utilized by study participants during the study. Only 119 (5%) of the 2564 viral load results reviewed for this study came from laboratories, where undetectable viral loads were not available. HIV-specific laboratory analyses from the Veteran’s Affairs Health System and from clinical trials were not reportable to the state health department during this period.
Follow-up spanned from the date of initial HIV diagnosis through loss to follow-up, death, or until December 31, 2009, whichever occurred first. Follow-up was censored for individuals with evidence of HIV care outside of Colorado as demonstrated by (1) a signed request for information from an out-of-state provider, (2) documentation of out-of-state HIV care in medical records, or (3) notation in the medical records of intention to leave the state followed by no further visits or laboratory data within Colorado. Linkage to care required evidence of an initial HIV clinical visit or HIV-specific laboratory analyses (HIV-RNA or CD4 count), excluding laboratory analyses performed at the time of initial HIV diagnosis and excluding visits with linkage-to-care personnel. Retention in care was successful if there were no 180-day gaps between HIV clinical visits and/or HIV-specific laboratory analyses. Sensitivity analyses explored alternative definitions of retention in care, where success was defined by an absence of 270-day or 360-day gaps in HIV care. Loss to follow-up was defined by the absence of a documented HIV clinical visit or HIV-specific laboratory during the last 180 days of follow-up in this study, July through December 2009, in noncensored individuals. Engagement in care is a term that describes the entire “in-care” spectrum including linkage to care, retention in care, and nonloss to follow-up.
Data retrieved from medical records included demographics, HIV risk factor, HIV testing data, evidence for utilization of clinical trials, evidence of incarceration, all systemwide visit data, all HIV-specific laboratory, and whether ARV medications were initiated. In addition, we reviewed all phone encounters and outside information to identify utilization of resources outside of the clinical sites in this study. The CDPHE data were reviewed for the date of HIV diagnosis and HIV-specific laboratory results.
Data Analysis
Basic descriptive statistics were utilized to describe the population as well as to explore linkage to care, retention in care, and transitions in care between clinical care sites. Kaplan-Meier analysis was performed to assess the median time to initial linkage to HIV care. Individuals were censored in this analysis at the end of follow-up or if they died prior to initial linkage to care. For loss to follow-up analyses, we explored the impact of our definition of loss to follow-up (no visit in the last 6-month period) by assessing reengagement in HIV care for individuals deemed lost to follow-up at earlier time periods than at the end of the study. We utilized the chi-square test to evaluate the association between overall engagement in care and receipt of HIV care from more than 1 provider/location. All analyses were performed using SAS statistical software version 9.2 (SAS Institute Inc, Cary, North Carolina).
Results
From 2005 through 2007, approximately 40 000 HIV antibody tests were performed through Denver Health. A total of 613 individuals tested positive for HIV-1 antibodies, and 521 had confirmed HIV infection (Figure 1). Of these individuals, 154 (30%) had evidence of prior HIV antibody positivity and were excluded. Of the 42 anonymous testers, 15 (36%) did not provide identifying information after learning of their HIV-positive result and were excluded. This left 352 newly diagnosed HIV-1-infected individuals in this study, 300 (85%) of whom had contact with the Denver Public Health linkage-to-care program. These 352 individuals comprised 29% of the 1201 new HIV diagnoses in Colorado from 2005 through 2007.
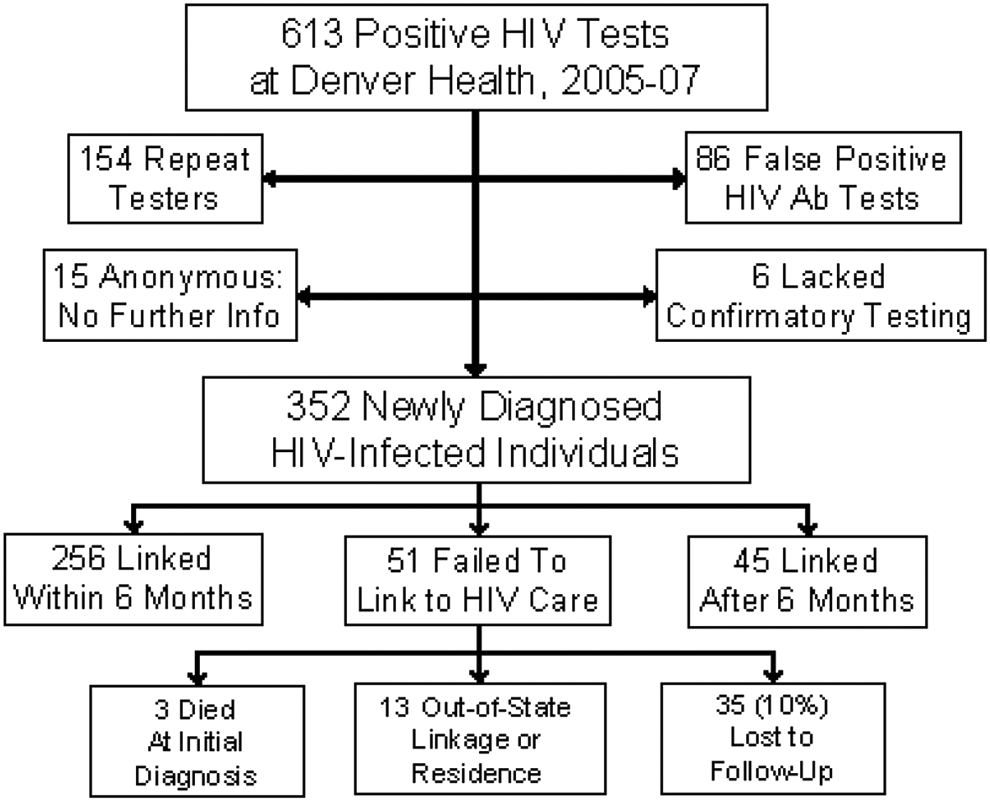
Study flow diagram depicting the disposition of 613 individuals who tested positive for HIV antibody (Ab) at Denver Health and Hospital Authority, between 2005 and 2007.
Table 1 shows the baseline data on the included cohort. The median age was 34 years (interquartile range [IQR] 27-42), 8% were women, 50% were white, 30% Hispanic, and 15% black. HIV acquisition risks included 74% men who have sex with men (MSM), 12% heterosexual, 6% MSM with injection drug use (IDU), and 5% IDU alone. Median baseline CD4 count was 409 cells/mm3 (IQR 239-592 cells/mm3), and median baseline HIV-RNA level was 4.6 log10 copies/mL (IQR 3.8-5.0 log10 copies/mL). Median duration of follow-up was 2.6 years (IQR 1.0-3.6 years).
Population Characteristics of 352 Newly Diagnosed HIV-Infected Individuals at Denver Health and Hospital Authority, Between 2005 and 2007.

Abbreviations: MSM, men who have sex with men; IDU, injection drug use.
a Median (interquartile range).
Location of HIV testing included 142 (40%) individuals who tested positive in the STD clinic, 74 (21%) through bathhouse outreach testing, 30 (9%) through outpatient medical or subspecialty clinics, 30 (9%) during inpatient hospitalization, 28 (8%) at a dedicated HIV counseling and testing site, 23 (7%) through the Denver Health emergency room or urgent care clinic, 18 (5%) through nonbathhouse outreach testing, and 7 (2%) through jail testing.
Linkage to Care
Linkage to care within Colorado was documented in 301 (86%) individuals (Figure 1) who linked to 23 different HIV providers. Of the 301 linked individuals, 228 (76%) initiated care within a clinical site included in this study; 164 (54%) received all of their follow-up HIV care within an included site. Overall, 231 (66%) of the 352 individuals linked to initial HIV care within 90 days and 256 (73%) linked to care within 180 days of HIV diagnosis. In all, 51 (14%) individuals did not link to HIV care in Colorado including 3 who died during a hospital stay that included their initial HIV diagnosis and 13 individuals who were either out-of-state residents (n = 3), self-reported out-of state linkage (n = 3), or had a signed request for medical information from out of state (n = 7). Excluding these 16 individuals, we were able to document linkage to HIV care for 301 (90%) of the 336 care-eligible individuals (69% within 90 days and 76% within 180 days). In Kaplan-Meier analysis (censoring at the end of follow-up and for individuals who died before initial linkage), the median time to initial linkage was 39 days (IQR 19-144 days; Figure 2).

Kaplan-Meier curve representing time to initial linkage to HIV care for 352 newly diagnosed HIV-infected individuals at Denver Health and Hospital Authority, between 2005 and 2007.
Retention in Care
Overall, 168 (56%) of the 301 individuals who linked to HIV care had at least one 180-day gap in care. Of these 168 individuals with at least 1 gap in care, 101 (60%) had a single 180-day or longer gap in HIV care, 46 (27%) had two 180-day gaps in care, and 21 (13%) had 3 or more 180-day gaps in care. We defined cyclical engagement in care as occurring in individuals with more than 1 gap in care. By this definition, 67 (22%) of the 301 individuals who linked to care had cyclical engagement in HIV care. In sensitivity analyses, utilizing alternative definitions for retention in care, we found that 89 (30%) of the 301 individuals who linked to care had at least 1 gap in care lasting 270 days or more, and 49 (16%) had at least 1 gap in care lasting 360 days or more.
Loss to Follow-Up
Loss to follow-up analyses included all individuals, not just those who linked to HIV care. Over the last 6 months of 2009, 196 (56%) of 352 individuals were in care, 106 (30%) were lost to follow-up, 39 (11%) had evidence of out-of-state care or residence, and 11 (3%) had died. It was very likely that losses to follow-up included a significant number of individuals captured during a gap in care over the final 6 months of follow-up. In order to evaluate this, we assessed reengagement in care for individuals who appeared to be lost to follow-up during earlier time periods. For example, 53 individuals in this cohort had no HIV visits or laboratory analyses during the last 6 months of 2007. In 2008, 26 (49%) of these 53 individuals received HIV care in Colorado, and by the end of 2009, 33 (62%) had evidence of HIV care. Similarly, 78 individuals in this cohort had no evidence of HIV care during the last 6 months of 2008. In 2009, 41 (53%) of these 78 individuals accessed HIV care in Colorado.
Engagement in Care
Engagement in care describes the spectrum of involvement in HIV care including timely linkage to care, full retention in care, and nonloss to follow-up. Overall, 58 (16%) of 352 newly diagnosed HIV-infected individuals linked to care within 180 days of initial HIV diagnosis, had no 180-day gaps in HIV care, and were not lost to follow-up during the last 6 months of 2009. Excluding the 50 individuals who were known to leave the state or died during follow-up, 19% of the 302 “in-state” individuals were successful at all stages of engagement in care as defined. In a sensitivity analysis, changing our retention and loss to follow-up criteria to include successful retention as not having any gap in HIV care longer than 360 days and being seen in the last year of follow-up (2009), 143 (47%) of 302 “in-state” individuals were successful.
To evaluate engagement in HIV care over time, we determined the proportion of individuals with evidence of HIV care (visits or laboratory) in sequential 6-month time periods beginning with the date of HIV diagnosis. Over sequential 6-month time periods, retention in care declined over time, and 46% of the individuals had evidence of HIV care after 42 to 48 months of follow-up (Figure 3A). In an analysis that censored individuals who died or moved out of state (Figure 3B), at 48 months of follow-up 54% of individuals had evidence of HIV care over the prior 6 months, 10% never linked to care, and 36% failed to be retained in care.

Percentage of patients engaged in HIV care during 6-month intervals after initial HIV diagnosis for 352 newly diagnosed HIV-infected individuals in Denver between 2005 and 2007. A, Includes individuals who died and individuals with medical record evidence of no longer residing in Colorado. B, Censors individuals who died and individuals with evidence of no longer residing in Colorado. In-care status was determined during each time period and was not dependent on success at prior time periods.
Transitions in HIV Care
Of the 352 included individuals, receipt of HIV care from more than 1 HIV provider was common, occurring in 131 (37%) individuals. In all, 76 (22%) individuals accessed HIV care at ≥2 clinical sites within Colorado, 20 (6%) accessed care at a clinical site and while incarcerated, 17 (5%) accessed care at a clinical site and through a clinical trial, 14 (4%) accessed HIV care both inside and outside of Colorado, and 4 (1%) had more complicated patterns of HIV care over time. Overall, incarceration was evident in 45 (13%) individuals although more than half of these individuals had no laboratory evidence of accessing HIV care while incarcerated. Time spent living out of state (with or without evidence of HIV care) was apparent in 54 (15%) individuals; 6 of these individuals were outside of the United States. There was no association between overall engagement in care and receipt of care from multiple locations.
Discussion
Adequate engagement in HIV care is vital to achieve optimal HIV treatment outcomes. Here we describe the spectrum of engagement in care for a well-defined, newly diagnosed HIV-infected cohort utilizing clinical data and state laboratory reporting databases. We found that 86% of the cohort established initial HIV care in Colorado; however, only 73% of the overall cohort linked to care within 180 days. Once in care, gaps in care were common, with 56% of the individuals having at least one 180-day gap in HIV care and 16% (1 in 6 individuals) having at least one 360-day gap in care. Overall engagement in care was poor when defined as linking to care within 180 days and having no 180-day or longer gaps in HIV care until the end of follow-up. Utilizing this definition, only 19% of the uncensored individuals were successful. However, 47% were deemed successful when defining successful engagement as having no gaps in care greater than 360 days in duration. Care patterns for 37% of the cohort were complex as demonstrated by accessing HIV care from at least 2 providers over a median of just 2.6 years of follow-up.
The national HIV/AIDS strategy proposes that 85% of the newly diagnosed HIV-infected individuals be linked to HIV care within 3 months of diagnosis. 11 Variable initial linkage rates from 60% to 70% were described in the early literature. 12,13 Over time, rates of linkage appear to have improved. Seventy-eight percent of individuals in the intervention arm of the Antiretroviral Treatment and Access Study (ARTAS) linked within 6 months of enrollment. 12 In New York City, utilizing HIV laboratory reporting data, Torian and colleagues found that only 64% linked within 3 months; however, 83% linked within 2 to 4 years of diagnosis—most of whom linked in the first year. 14 A study in Seattle/King County demonstrated 88% linkage within 3 months. 15 The linkage-to-care program at Denver Health was developed utilizing the ARTAS model, and our rates of linkage have been similar; 85% of this cohort met with our linkage-to-care personnel. A strength of our study is the availability of individual-level follow-up and outcome data for a large proportion of included individuals who accessed care at an included clinical site. After adjusting for individuals who died or were reasonably believed to be out of state, we had evidence of linkage for 90% of the newly diagnosed individuals.
Despite the fact that initial linkage was demonstrated in a high percentage of individuals, retention in continuous care was uncommon. Utilizing 180 days to define a gap in care, more than half of the individuals who linked to care had poor retention. In addition, 1 in 3 individuals had at least one 270-day gap in HIV care, and 1 in 6 individuals had at least one 360-day gap in care. Similar poor rates of retention in HIV care have been documented in other studies. 16 –18 We defined retention using a gap-in-care approach by measuring time between HIV care visits and/or HIV-specific laboratory analyses. We did not utilize the more detailed criteria set forth by the US Health Resources and Services Administration, having 2 or more outpatient visits at least 3 months apart during a 12-month period, because we did not have visit data for all individuals. At least 1 study has shown that these 2 measures are similar. 19
Poor retention in care is associated with unfavorable treatment outcomes. Early analyses demonstrated increased mortality in individuals with poor retention. 7,8 Recently, a large cohort study confirmed these results. 20 Others have shown that poor retention in care is associated with an increased risk of virologic failure, immunologic failure, and progression of HIV disease. 6,9,21 –23 We demonstrated poor retention in the majority of individuals. This finding leads to concern about the long-term health of HIV-infected populations. However, national HIV mortality data and clinical experience suggest that most HIV-infected individuals do well. One potential reason for this apparent discordance is that available research underestimates engagement in care. Our study supports this hypothesis. Analyses from single institutions, lack of full reporting of laboratory data to state databases, and patient migration and transitions in care, all can lead to underestimation of engagement in care. We demonstrated that these last factors, migration and transitions in care, are common, and further research is necessary to understand the implications of these findings on estimates of engagement in care as well as on clinical outcomes in HIV care.
Engagement in HIV care is a dynamic process. Individuals commonly appear lost to follow-up when using cross-sectional evaluations of receipt of HIV care. However, over time we showed that 49% to 62% of individuals who appear lost to follow-up have evidence of re-engagement in HIV care within 1 to 2 years. These individuals were caught in a gap in HIV care of variable duration. Additionally, 1 in 3 individuals had evidence of HIV care from more than 1 medical provider, 1 in 5 had cyclical engagement in HIV care, 1 in 6 had evidence of incarceration, and 1 in 7 had evidence of out-of-state care or residence. These complex patterns of HIV care transitions need to be understood further in order to develop mechanisms to promote seamless migrations through HIV care systems within a region or state as well as between states. Studies of engagement in HIV care, which utilize national-level data will be essential to fully understand the care patterns of individuals living with HIV infection.
This study has several important limitations. During this study, not all CD4 counts and HIV-RNA levels were reportable in Colorado. This probably did not affect the linkage data to a great extent since most newly diagnosed individuals have a detectable viral load. Furthermore, we had full clinical data on more than half of the patients, and most laboratories reported undetectable viral loads during the study period. Having access to laboratory values from 2 clinical trial groups helped minimize the impact of this data gap in reporting databases. The contribution of not having laboratory values from the Veterans Administration (VA) Hospital system cannot be determined although it is likely small, as the Denver VA cares for only about 5% of HIV-infected individuals in the Denver metropolitan area. For all of these reasons, it is likely that we have underestimated engagement in care; the full extent of this underestimation is unknown.
Other limitations include that our population was homogeneous in gender and HIV acquisition risk factor with a predominance of MSM. Data from a large US-based study showed that male gender and MSM risk factor were associated with higher rates of retention in HIV care than in comparator populations. 24 Our population was diagnosed with a relatively high median CD4 count compared to other studies; individuals with higher CD4 counts are less likely to adequately engage in HIV care. 19,25 –27 Secular trends likely affected our retention estimates. During the period of this study, standard practices in HIV care began to shift to allow individuals with demonstrated excellent adherence, long-term viral suppression, and adequate immune function to have visits as infrequently as every 6 months. 28 Another limitation was that loss to follow-up in this study was a static descriptor of complex engagement in care patterns over time. However, because we were able to utilize statewide data from Colorado, rather than data from a single or a few institutions, our estimates of engagement in care are likely to be as good as or better than many prior estimates. Finally, we are in the process of expanding this cohort and increasing the duration of follow-up in order to assess the last stage of the engagement cascade—achievement of an undetectable HIV-1 viral load.
In conclusion, we found relatively slow rates of linkage to initial HIV care, falling far short of the goals of the national HIV/AIDS strategy. 11 After initial linkage, retention in care appeared poor over time, loss to follow-up was common, and transitions in HIV care were frequent and may represent an understudied component of poor engagement in HIV care over time. Recognition of the importance of adherence to ART to the success of HIV care has gained widespread acceptance over the past decade. Today, acknowledgment of the importance of engagement in HIV care is necessary to maintain the health of HIV-infected populations. In addition, it is likely that high levels of engagement in care will be required to give “test and treat” strategies for HIV prevention their greatest opportunity to decrease HIV incidence in the future.
Footnotes
Authors’ Note
These data were presented at the 5th International Conference on HIV Treatment Adherence, May 23-25, 2010, Miami, FL, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by the National Institute of Allergy and Infectious Diseases K01 AI067063 (EG) andP01 AI55356 (EC) as well as through UL1 TR00015 and UM1 A069450.