
Abstract
A retrospective cohort analysis was performed to describe outcomes and retention in care on antiretroviral therapy (ART) of 53 patients with severe mental illness (SMI). Diagnoses were psychosis secondary to HIV (24 patients), psychosis not otherwise specified (12), mania with or without psychosis (9), depression with psychotic features (4), and schizophrenia and bipolar mood disorder (2 each). The median baseline CD4 count was 66/mm3 and viral load was 5.4 log10 copies/mL. Thirteen (25%) patients were lost to follow-up (10 within 6 months), 3 were transferred out, and 3 died. By week 96, 29 (85%) of 34 (64%) patients still in care had a viral load <400 copies/mL and 26 (76%) a viral load <25 copies/mL. Median CD4 count increased to 307/mm3. Twenty-seven of 34 patients discontinued antipsychotic medication. Patients with SMI and advanced HIV infection responded well to ART. The first 6 months was important for retention in care.
Introduction
Mental illness is relatively common among people with HIV infection, with mood and anxiety disorders being most common. 1 Psychosis in the HIV-infected patient occurs as a primary psychiatric disorder, such as schizophrenia or schizoaffective disorder, or secondary to a general medical condition, namely the underlying HIV infection. 1 In the United States, secondary psychosis tends to occur in patients with advanced HIV and frequently HIV-associated dementia. 1 In contrast to this, secondary psychosis and mania in sub-Saharan Africa occur against a background of generally lesser degrees of dementia or none at all. 2 –4
There have been a number of reports on severe mental illness (SMI) and antiretroviral therapy (ART) outcomes with respect to drug adherence as a surrogate marker for virological suppression, 5 –11 to risk of virological failure, 12 –14 and to clinical outcomes (AIDS-defining illness and death). 15 Most of these articles have concentrated on depression or have included mixed psychiatric samples in which depression has affected a majority of the persons studied. 5,7 –10,12 –16 There have been a few specific studies detailing SMI separately from patients with depression without psychotic symptoms. 6,9,11 Among 47 patients with various diagnoses of SMI, the average adherence rate over 2 weeks measured by electronic monitoring bottle caps was 66%, with 40% having adherence rates ≥90% and 31% having adherence rates <50%. 6 Patients with SMI were significantly less likely than those with no psychiatric disorder to discontinue ART in the first 2 years of ART. 9 This was however in a sample of patients where there was combined and integrated mental health and HIV care. Patients with bipolar disorder were statistically significantly less likely to have adherence rates ≥90% by electronic medication monitoring over 30 days than a control group without bipolar disorder (48% adherent versus 91%). 11 There has been 1 study examining virologic outcomes on ART. Patients with a range of mental illnesses showed a slower rate of virologic suppression and faster rate of virologic failure than those without SMI. 13 This was considered to be due to the association of mental illness with lower antiretroviral adherence, although adherence could not be measured in the study.
We aimed to describe patients with SMI (excluding major depression without psychotic symptoms) in a routine urban HIV clinic in Soweto, South Africa, an area with high HIV seroprevalence, with respect to virologic and immunologic outcomes and retention in care.
Methods
Setting
The study was conducted at the Adult HIV Clinic at Chris Hani Baragwanath Hospital, a 2700-bed public sector university hospital which is the main hospital serving Soweto. Free ART was introduced into the public sector in South Africa in 2004 and, in the Soweto area, was initially hospital based.
Study Population and Design
A retrospective cohort analysis was performed of 53 adults with a diagnosis of SMI who had initiated ART from 2004 to 2006. The SMI had been diagnosed in hospitalized adults by an academic psychiatry unit based at the hospital. A specialist psychiatrist reviews each patient seen by a member of the unit. The diagnosis was abstracted from the medical record. Diagnoses included were, as in similar studies, from Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) axis 1 conditions, which comprised psychosis secondary to general medical condition (HIV), psychosis not otherwise specified, mania with or without psychosis and secondary to general medical condition (HIV) or not otherwise specified, depression with psychotic features, schizophrenia or schizoaffective disorder (here called schizophrenia), or bipolar mood disorder (BMD). One patient on treatment for cryptococcal meningitis, 1 patient with postpartum psychosis who was not on antipsychotic medication, and a further 11 patients with a diagnosis of “psychotic episode” had been excluded from the study. The patients were identified from a paper-based database of patients initiating ART at the adult HIV clinic. The patients were all being managed for mental illness either by psychiatric services at the hospital or by liaison psychiatric services at community clinics. Sodium valproate was the usual drug prescribed for mood stabilization, while haloperidol or risperidone was used most commonly for psychosis. For adults, CD4 count of less than 200 cells/mm3 and/or World Health Organization (WHO) stage IV disease defined ART eligibility, per national guidelines at that time. The usual starting regimen at the clinic was 2 nucleoside reverse transcriptase inhibitors, usually stavudine (d4T) and lamivudine (3TC), together with a nonnucleoside reverse transcriptase inhibitor, usually efavirenz (EFV). In a patient with psychosis, nevirapine (NVP) or lopinavir/ritonavir (LPV/r) was to be considered rather than EFV. Patients were strongly encouraged to identify a treatment supporter in their home.
Procedures
Data were collected from clinic and laboratory records until the patients had been on ART for 96 weeks or were no longer in care at the clinic. A standardized data collection form was used. Baseline information comprised age, sex, WHO stage, baseline CD4 count and viral load, ART initiation date and regimen choice, and psychiatric diagnosis. Indicators for progress on ART included sequential CD4 and viral load results at 24, 48, and 96 weeks (or closest available result), hospitalizations for psychiatric or medical reasons, ART drug toxicity, and any drug changes. Virologic suppression was defined as a viral load <400 copies/mL but <25 copies/mL was also reported. Outcome was assessed by death, loss to follow-up, transfer out, or retention in care with or without virologic suppression.
Research Approval
The study was approved by the Human Research Ethics Committee, University of the Witwatersrand, Johannesburg (Protocol M050221).
Results
The baseline characteristics and events on ART of the 53 patients are presented in Table 1. Twenty (38%) patients initiated ART with CD4 count <50/mm3 and 66% were in WHO stages 3 or 4. The commonest diagnosis was psychosis in 36 (68%) patients. It was psychosis secondary to general medical condition, namely, HIV infection in 24 (45%) patients and psychosis not otherwise specified in 12 (23%) patients. The next most frequent condition was mania in 9 (17%) patients, in 3 of whom it was considered secondary to HIV and in 6 not otherwise specified. Two patients each had schizophrenia or BMD. Zidovudine (ZDV) and 3TC were prescribed for 6 patients, all with psychosis, and d4T with 3TC for the other 47 patients. The third drug initially prescribed was EFV in 35 patients (25 with psychosis, 6 with mania, 2 with depression and psychotic features, and 1 each with BMD and schizophrenia). Nevirapine was given to 16 patients (10 with psychosis, 2 with mania and 2 with depression with psychotic features, and 1 each with BMD and schizophrenia). Lopinavir/ritonavir was the third drug prescribed for 1 patient each with psychosis and with mania. Four patients on EFV subsequently switched to NVP or LPV/r, 2 relatively early and 2 late. One patient with BMD was switched at week 2 by his clinician who recognized a possible error, and a second patient with mania was substituted after 4 months when hospitalized with recurrence of mania. The other 2 were switched late in the second year as requested by their psychiatrist, and neither had deteriorated mentally and both still required antipsychotic medication. A number of other patients were left on EFV in consultation with their psychiatrists since there had not been any deterioration in their mental health over time. Poor compliance was based on patient report and physician notes. One of the 9 patients with poor compliance to ART also interrupted ART. Three of the 6 patients who interrupted did so because of symptomatic hyperlactatemia, and/or a mitochondrial toxicity due to d4T.
Baseline Characteristics, Treatment Events, and Outcome of 53 Patients on ART and with Serious Mental Illness (SMI) Followed to 96 Weeks.

Abbreviations: WHO, World Health Organization; ART, antiretroviral therapy.
Thirteen patients were lost to follow-up: 3 in months 0 to 3, 7 in months 4 to 6, 2 in months 7 to 12, and 1 in the second year. For patients still attending the clinic after 6 months on ART, 3 (8%) of 37 patients were subsequently lost to follow-up. Eight of the 10 patients who were lost to follow-up and who, while still on the program, had follow-up blood tests had virologic suppression. Of those lost early to follow-up, 1 patient did not return after initiation of ART, 1 withdrew at week 2, and 1 had ART withheld by his mother from week 2. The third drug in those lost to follow-up was EFV in 8 patients, NVP in 4 patients, and LPV/r in 1 patient. The outcomes for patients by psychiatric diagnosis are shown in Table 2.
Outcome by Psychiatric Diagnosis for 53 Patients with Severe Mental Illness.
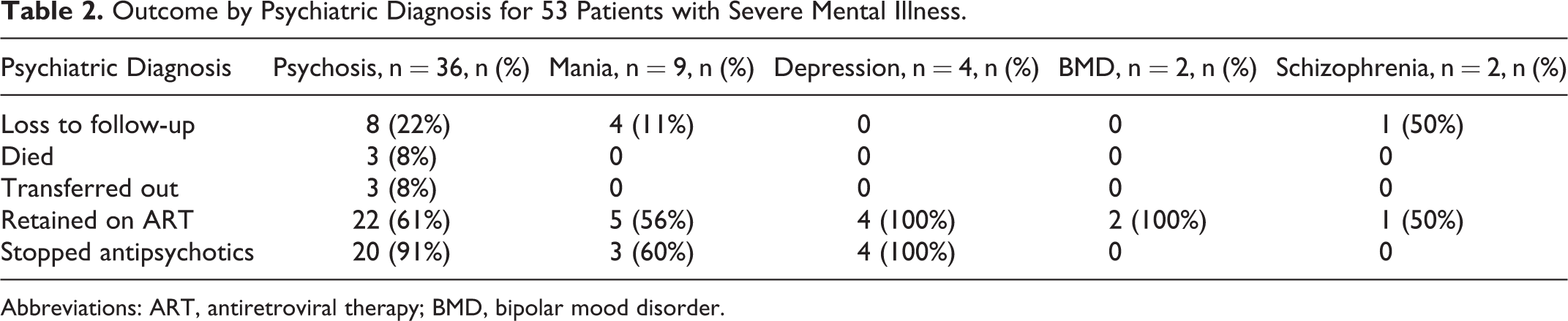
Abbreviations: ART, antiretroviral therapy; BMD, bipolar mood disorder.
The 3 deaths occurred in the first 6 weeks, 2 due to disseminated tuberculosis and 1 due to Mycobacterium avium complex bacteremia.
By week 96, 34 (64%) patients were retained on ART at the clinic. These comprised 22 (61%) with secondary psychosis, 5 (56%) with secondary mania, 2 with BMD, 1 with schizophrenia, and all 4 with depression with psychotic features. Seven (21%) of these 34 patients were still on antipsychotic medication and 1 was on an antidepressant (Table 2). The documentation of the time of cessation of psychotropics in the patients was generally poor, but all seemed to have remained on psychiatric treatment for at least 6 months. Similarly, it was generally unclear whether there had been self-withdrawal by patients or whether it had been in consultation with the psychiatric service. All such patients were considered to be apsychotic at subsequent HIV clinic visits, and none were known to have reinstituted psychotropic medication.
By week 96, virological suppression (a viral load <400 copies/mL) was found in 85% of patients retained on treatment and 55% of the original cohort (Table 3). Four patients were switched to second-line drugs due to virological failure and their virologic outcomes are included in the table.
Proportion of Patients with Viral Load (VL) Suppression at Weeks 24, 48, and 96.

The median CD4 count increased steadily from 66/mm3 at baseline to 307/mm3 by week 96, an increase of 241/mm3 (Table 4). After 2 years on treatment, 4 (7%) patients had attained a normal CD4 count >500/mm3.
Median CD4 Counts/mm3 at Baseline and after 24, 48, and 96 Weeks.

Discussion
In this study, patients with SMI showed very good immunological and virological responses, which were similar to those in community settings in South Africa and the United States. Virological suppression (<400 copies/mL) of 85% of patients at 2 years of ART was similar to that in unselected public sector adult cohorts in South Africa, namely 70% in Khayelitsha, Cape Town and 72% (who had suppressed and not had a viral rebound) in Johannesburg. 17,18 The 76% who had virologic suppression (<25 copies/mL) was equivalent to the 60% to 72% of women, by race and ethnicity, in the United States, who ever achieved a viral load ≤80 copies/mL. 12 The 12-month results were similar to the 12-month suppression (<400 copies/mL) of 80% of patients in Baltimore, USA. 19 The results were superior to those in patients with mental illness (predominantly depression) in a US military cohort who had virologic suppression (<400 copies/mL) of 69% at 12 months and 38% at 24 months. 14 The reporting of virologic suppression in the mental health literature is frequently not direct, as in this study, but rather examines risks for failure against various control populations, and is in consequence not directly comparable to this study. People with mental illness on ART had inferior outcomes in 3 such studies 12 –14 but not in another. 8
The majority of patients lost to follow-up in this Soweto cohort were lost in the first 6 months of ART. In Uganda, continuous retention in care at 12 months was 47% among those with SMI including depression compared to 65% for those without SMI. After 6 months in care, SMI had no further effect on interruption to care. 20 The rates of retention of patients with SMI in Soweto were equivalent to those in Uganda in patients without mental illness.
At baseline, patients had advanced HIV infection with low CD4 counts as was expected with ART guidelines in South Africa at the time. The median CD4 count after 2 years on ART was similar to the 323/mm3 in a Cape Town community cohort and the estimated mean CD4 of 372/mm3 in a general clinic in Johannesburg. 17,18
A fairly large proportion of patients were lost to follow-up, some of whom may have died, given the low starting CD4 counts. For some patients who were lost to follow-up, discontinuation of ART may well have occurred and may have been related to the underlying psychosis. However, a number of community clinics became accredited ART sites during the course of the study, and patients may have obtained ART care at the same clinic as provided their mental health care. Care was fragmented for patients in the study as they needed to go to a separate clinic for mental health care. Yet for those retained in care in this study, treatment was highly successful. There are initiatives to integrate mental health care and ART. This can be done within a psychiatric service if the capacity and staffing exist 21 or in an HIV clinic where health care workers can be trained to provide adequate mental health care, in terms of diagnosis and treatment, for common conditions such as depression and anxiety. Psychosis and mania, however, would justifiably require specialist psychiatric care if available.
Efavirenz, a nonnucleoside reverse transcriptase inhibitor, is associated with a characteristic constellation of neuropsychiatric adverse events, including insomnia, vivid dreams, and dizziness, usually transiently in the first month of treatment. 22 –24 There is a paucity of conclusive evidence that EFV causes severe mental health problems. 22 –24 There have been a number of reports of psychosis or mania (after an overdose) developing in patients without SMI in a temporal relationship to starting ART with EFV. 22,25 –33 High serum levels of EFV related to genetic factors have been implicated in the development of psychosis, 27,29,30 but this has not been borne out in longitudinal studies. 22 –24,34 Other antiretroviral drugs, including ZDV, abacavir (ABC), and NVP, have also been implicated in the development of psychosis by temporal association. 22 We were surprised to find that EFV had been so commonly used in this cohort of patients with SMI, because there was a clear policy to avoid its use if there were alternatives. In only 1 patient, who was hospitalized for mania at 4 months, was there a possibility of EFV being implicated in psychiatric deterioration, but the episode of mania may have been part of the natural history of the condition. Patients on EFV were not more likely than those on NVP to be lost to follow-up, and none of those lost patients was subsequently hospitalized at the study hospital, which suggests that those patients were unlikely to have had severe mental deterioration related to EFV use. Efavirenz use seemed to have been safe and not associated with mental health deterioration in this cohort of patients with a predominant diagnosis of psychosis related to HIV infection. A register of the use of EFV in psychotic patients may help to elucidate this further.
The majority of patients retained in care had discontinued antipsychotic medication by the end of the study period, suggesting that successful ART may have enabled patients with psychosis or mania secondary to HIV infection to recover after they had been stabilized on psychiatric medication. There is a paucity of literature concerning this and experience from other centers needs to be compared. The fact that advanced HIV-associated dementia does not seem to be common in association with secondary psychosis and mania related to HIV infection in sub-Saharan Africa may hinder direct comparisons with patients from other continents. There was no difference in retention for patients with secondary psychosis or secondary mania. The 2 patients with mania who remained on antipsychotic medication may have had BMD. Both of the patients with BMD and 1 of 2 with schizophrenia were retained in care.
There are a number of limitations to this study. The study sample was relatively small and it was a retrospective study. The patients’ mental health care providers and the HIV clinic physicians were not in direct contact about many of the patients. The diagnoses available in the HIV clinic records were abstracted from the patients’ self-retained clinical notes, so there may have been misclassification, although all patients had been assessed by a psychiatrist and were on psychiatric medication at ART initiation. All patients had been investigated for opportunistic infections which could have mimicked psychosis. We excluded patients who were likely to have had delirium. At the neuropsychiatric HIV clinic which has subsequently been established at the same hospital, where mental health care and HIV care are integrated, 59% of mental illness diagnoses were considered secondary to HIV infection. 21 Referral bias may have meant that the patients in the study were not representative of all persons with SMI and HIV infection who were eligible for ART.
In conclusion, patients with SMI responded well to ART in a routine clinic setting and, by the end of 2 years, many of those with psychosis related to HIV infection had discontinued antipsychotic medication. This finding requires confirmation in other similar cohorts. Every effort should be made to manage patients with the help of mental health professionals, and to trace patients who miss appointments, especially in the first 6 months of ART. Efavirenz seemed safe from a mental health standpoint in this cohort with SMI but needs further study. Despite the small sample size, the setting of the study in a sub-Saharan city with a high HIV seroprevalence makes these observations of importance for comparison in other geographic areas.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.