
Abstract
Aims:
This study aimed to describe the prevalence and pattern of lipid abnormalities among antiretroviral therapy (ART)-naive HIV patients, understand if there is any relationship to virologic and immunologic status, and discuss the implications for care.
Methods:
This was a cross-sectional study in which baseline demographic, clinical, and laboratory data of all ART-naive HIV-infected individuals recruited into the adult ARV clinic, University College Hospital, Ibadan, between January and December 2006, were analyzed.
Results:
In total, 1316 ART-naive HIV-infected persons were recruited in the period. Females subjects and participants aged ≦35 years accounted for 67.1% and 57.7% of all participants, respectively. At least 1 abnormal lipid fraction was seen in 73.3% of participants. It was observed that in 11.5% participants the total cholesterol (TC) was ≧5.2 mmol/L, in 2.7% the low-density lipoprotein cholesterol (LDL)-C was >4.1 mmol/L in 56.5% the high-density lipoprotein cholesterol (HDL)-C was <1.0 mmol/L, and in 27.6% the triglyceride (TG) was >1.7 mmol/L. The TC, LDL-C, and HDL-C were all significantly positively correlated with CD4 counts and negatively correlated with viral load. On the contrary, the TG levels were negatively correlated with CD4 counts and positively correlated with viral load. Multivariate linear analysis showed a significant relationship between all the lipid parameters and viral load. CD4 counts were only significantly associated with TC.
Conclusions:
A significant burden of dyslipidemia exists among ART-naive HIV-infected persons. Low HDL-C was the most frequently observed abnormality. The abnormalities related more with viral load levels than with CD4 counts. Dyslipidemia screening should be done in ART-naive HIV-infected persons. Simple healthy lifestyle changes should be emphasized, with other care given to those with the disorder.
Keywords
Introduction
Sub-Saharan Africa remains the region of the world that is most heavily affected by HIV. In 2010, the total number of people living with the disease in the region was estimated at 22.9 million, representing about 67% of the global burden of the disease. 1 About 10.4 million of these individuals were estimated to be eligible for antiretroviral therapy (ART), with the lifesaving ART based on World Health Organization 2010 guidelines. However, with ART coverage in the region at about 49%, only about 5 million will receive the therapy. 1 In essence, about 18 million (78%) individuals living with HIV/AIDS in the region will not be on any antiretroviral (ARV) agent.
In the absence of ART, the natural course of the HIV infection is characterized by viral replication and a slow but progressive destruction of the immune system. 2 Stimulation by the proliferating HIV antigens results in the almost pathognomonic feature of progressive HIV infection, that is, chronic immune activation. 3 This is characterized by polyclonal B-cell activation; increased T-cell turnover; increased frequencies of T cells with an activated phenotype; and increased levels of the proinflammatory cytokines such as interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor-α(TNF-α)]. 3 The production of these cytokines is believed to contribute to the progression of the disease by activating HIV-1 replication and maintenance of active HIV-1 expression. 4
The profile of cytokine production described above has been known to induce insulin resistance. This induction is thought to occur through a variety of mechanisms including the ability of these cytokines to cause increased lipolysis with the release of free fatty acids and inhibition of insulin receptor substrate 1 function with sequestration of the cytosolic glucose transporter 4. 5 The manifestation of these effects includes lipid metabolism disorder. In this study, we describe the prevalence and pattern of lipid abnormalities among ART-naive HIV-infected patients, define the relationship to their virologic and immunologic status, and discuss any implications for care.
Materials and Methods
Patient Population
This was a retrospective cross-sectional review of clinical and laboratory records of patients attending the adult ARV clinic of the University College Hospital (UCH)/University of Ibadan (UI), Ibadan, Nigeria. The UCH/UI ARV clinic is one of the first-generation HIV treatment centers established by the Government of Nigeria in 2002. Patients were entered into the adult ARV clinic if they were aged 15 years or older and were HIV infected. Evidence of HIV infection was a positive enzyme-linked immunosorbent assay (ELISA) confirmed by a Western blot assay. HIV-infected pregnant women were seen in the prevention of mother-to-child transmission clinic, and their data were excluded from the review.
Data Collection
Initial clinical assessment included obtaining a medical and medication history and a complete physical examination. Initial laboratory investigation included a full blood count and blood chemistries (alanine transaminase, urea, glucose, creatinine, and a complete lipid profile). All enrolled patients were required to have sputum and chest X-ray examination for tuberculosis, baseline CD4 count (cells/mm3), and HIV-1 RNA load. A consent was obtained for data repository for future studies as approved by the institutional review board of the University of Ibadan/University College Hospital, Ibadan, Nigeria. The baseline data used for this study were those of all consenting ART-naive HIV-positive individuals recruited into the clinic between January and December 2006.
Laboratory Analysis
Fasting blood samples were collected into tubes containing potassium ethylenediaminetetraacetic acid and fluoride oxalate for the measurement of lipids and glucose, respectively. Plasma total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglycerides (TGs), and glucose estimations were done using a Roche Hitachi 902 auto-analyzer (Roche Diagnostics Co, Indianapolis, IN) and standard Roche enzymatic kits (Roche Diagnostics, Basel, Switzerland). Low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald formula (LDL—C in mmol/L = TC in mmol/L − [HDL-C in mmol/L, + TGs in mmol/L/5]. CD4 counts were measured using Partec Cyflow (Partec GmBH, Munster, Germany) and HIV-RNA viral load with Roche Amplicor HIV-1 version 1.5 (Roche Diagnostics, GmbH, Mannheim, Germany). Cholesterol goals were defined as recommended by the Infectious Disease Society of America (IDSA) and the Adult AIDS Clinical Trials Group (AACTG).
Statistical Analysis
Statistical analyses were done using Statistical Package for Social Sciences, version 17. Descriptive statistics are reported as means with standard deviation (SD) and median with interquartile range. Means were compared using the Student t test, medians were compared using the Mann-Whitney U test, while proportions were compared using the chi-square test. Spearman correlation coefficient was used to assess for associations, while multivariate linear regression was used to assess the relationships of parameters that had significant association by correlation analysis.
Results
During the period of study, a total of 1316 ART-naive HIV-infected persons were recruited into the adult ARV programme. Their general characteristics are as shown in Table 1.
General Characteristics of Participants.

Abbreviations: TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TGs, triglycerides; SD, standard deviation.
With regard to age at recruitment, 15.3%, 57.5%, and 84.4% were aged <25 years, <35 years, and <45 years, respectively. About 60% of the participants were married and 40.4% had received at least secondary school education. The frequency of reported comorbid conditions like cardiac disease, hypertension, and diabetes mellitus was 0.2%, 0.1%, and 0.2%, respectively. Male participants were older, had lower CD4 counts, and higher viral load counts at presentation.
The mean (SD) for the lipid fractions for all the participants studied were as follows: TC, 3.8 (1.2) mmol/L; LDL-C, 2.0 (1.0) mmol/L; HDL-C, 1.0 (0.5) mmol/L, and TG, 1.4 (0.7) mmol/L. Further details of the values obtained from the lipid fractions measured, by gender, are shown in Table 1. Lipid values associated with increased cardiovascular risk were seen in 73.3% of all studied participants. The proportion with TC ≧ 5.2 mmol/L was 11.5%; LDL-C > 4.1 mmol/L was 2.7%; HDL-C < 1.0 mmol/L was 56.5%; and TG > 1.7 mmol/L was 27.6% (Table 2). Significantly more females than males had TC ≧ 5.2 mmol/L (8.8% vs 2.7%; P = .012). The LDL values of >3.4 mmol/L, 4.1-<4.9 mmol/L, and >4.9 mmol/L were seen in 114 (8.4%), 28 (2.1%), and 7 (0.5%), respectively, participants of the entire participant population.
Proportion of Participants with Undesirable Lipid Concentrations.

Abbreviations: TC, total cholesterol; TGs, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Table 3 shows the correlations between the metabolic parameters (lipids fractions and fasting plasma glucose) and certain patient clinical characteristics. There was a significantly positive association between weight at diagnosis and CD4 counts (Spearman score was 0.404 and P < .01) and a significant negative association with RNA viral load (Spearman score was −2.92 and P <.001). Multivariate linear regression, with age and weight in the model, is also reported in Table 4.
Correlations between Metabolic Parameters and Certain Patient Characteristics.

Abbreviations: TC, total cholesterol; TGs, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Values are Spearman ρ.
bSignificant at P < .01.
Multivariate Linear Regression between Metabolic Parameters and Certain Patient Characteristics.
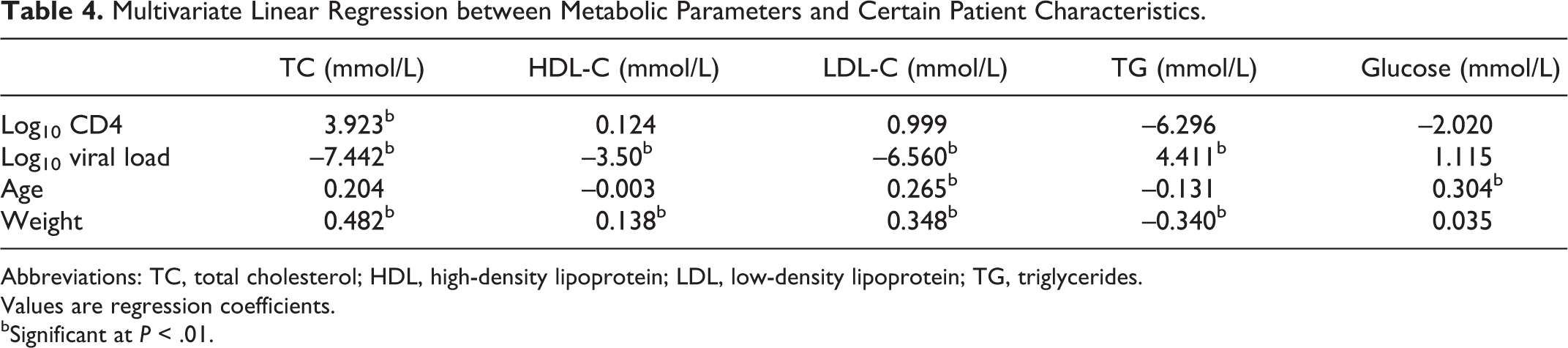
Abbreviations: TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides.
Values are regression coefficients.
bSignificant at P < .01.
Discussion
In 2001, the Adult Treatment Panel III of the National Cholesterol Education Program of the United States issued an evidence-based set of guidelines on cholesterol management. 6 In 2003, the IDSA and the AACTG recommended the use of these guidelines for the evaluation and treatment of HIV-infected persons. 7 Using these guidelines, we found that almost 3 out of every 4 ART-naive HIV-infected individuals in our clinic had at least 1 abnormal lipid fraction consistent with the increased atherogenic risk. This is similar to the findings in Jos (Nigeria), Southern Ethiopia, and rural South India. 8 –10 These findings, in concert with other described HIV-related disturbances of vascular compliance and endothelial dysfunction, may portend increased cardiovascular risk to those infected with HIV. 11
According to the above-mentioned guidelines, LDL-C levels should be the primary determinant of any intervention, therapeutic lifestyle changes (TLC), or drug therapy. The LDL-C goal, for a particular person, is modified by the number of categorical risk factors for coronary heart disease. In the absence of many of these risk factors (0-1), the LDL-C level for intervention is ≧4.1 mmol/L for TLC and ≧4.9 mmol/L for drug therapy. LDL-C values such as these were seen in only 2.7% and 0.2% of the study population, respectively. Our findings agree with the observations of Riddler et al 12 among 50 male seroconverts before ART initiation. Two percent of their study population had LDL-C values ≧4.1 mmol/L. Although it is reassuring, especially in a resource-constrained environment, that most of patients with dyslipidemia will require only TLCs initially, it is important that the few who require pharmacologic intervention are granted access to LDL-C- lowering therapy. The recognition of these groups is further underscored by the tendency of some ARV drugs to cause further increases in LDL-C levels. Such drugs include zidovudine (ZDV), tenofovir (TDF), nevirapine (NVP), and efavirenz (EFV), which are among the recommended first-line agents in this region. 11,13
The most common abnormal lipid parameter in this study was an HDL-C level <1.0 mmol/L, which was observed in 56.5% of the participants. This is in agreement with other studies with similar levels of HDL-C observed in 63.7% to 73.3% of their ART-naive population. 8,9,12 With HDL-C < 1.0 mmol/L being a recognized categorical risk factor for increased risk for an adverse cardiovascular event, the implication is that over half of our participants have at least one risk factor that can modify the LDL-C values to be used as a target for therapy. The presence of another risk factor will drop the intervention trigger value for LDL-C to 3.4 mmol/L. This range of LDL-C values were observed in 8.4% (111) of our population. Daniyam and Iroezindu reported a value of 5.7% among their group of 106 ARV-naive HIV-infected patients in Jos, Nigeria. 10 However, they had excluded individuals with diabetes and those who were obese from their study. An HDL-C value of <1.0 mmol/L should prompt a screen for any of the other categorical risk factors, such as cigarette smoking, hypertension or antihypertensive medication usage, family history of premature coronary heart disease, and age (men ≥45 years; women ≥55 years), and intervention for dyslipidemia guided appropriately, with regard to LDL-C value to be used to initiate any additional intervention.
We demonstrated a relationship between immunologic (CD4) and virologic (viral load) status of the participants and their lipid parameters as shown in Tables 3 and 4. The summation of the correlation studies is that the levels of all cholesterol-containing fractions decrease with increasing severity of disease while the TG levels increase. This is consistent with the previously reported studies 12,14,15 and is consistent with dyslipidemia seen in chronic inflammatory conditions and associated with the development of insulin resistance. 16 With multivariate linear regression, viral load retained the same significant relationship with all the lipid parameters, while CD4 count was only significantly associated with TC. Weight and age were also included in the regression model. The sustained relationship between viral load and lipid parameters is also suggested by the findings of El-Sadr et al. 17 This probably reflects a direct relationship between viral replication and chronic inflammation and, as a consequence, insulin resistance. The most common cause of T-cell activation and inflammation in HIV infection is antigenic stimulation by the replicating virus. 18 The continuous viral replication induces strong T-cell responses, especially CD8. It is estimated that up to 20% of circulating CD8 can be HIV specific in untreated chronically infected patients. The CD4 cells are present at a lower magnitude. 19
The introduction of ART is associated with higher levels of TC, LDL-C, and HDL-C compared to the ART-naive state. 9 This has been suggested as a return to pre-infection blood lipid levels. However, with the duration from seroconversion to eligibility for ART, reportedly ranging from 3.3 to 10 years in low-income countries, 20 and the current ART coverage levels, measures to manage dyslipidemia among ART-naive individuals are important. The recommendation is that nondrug therapies, dietary and exercise intervention, be instituted first. With regard to improving HDL-C concentrations, aggregate evidence from literature review indicates that physical activity is accompanied by 5% to 30% increase in HDL-C. 6 A systematic review also suggested that prescribing specific diets, especially with omega 3 supplementation, provides adequate intervention to increasing HDL-C concentration in individuals with HIV/AIDS. 21 Smoking cessation, where relevant, should also be encouraged, as this also results in some increase in HDL-C concentration. 6 Lifestyle changes should be encouraged, through targeted health talks among all individuals with HIV/AIDS to improve the overall cardiovascular well-being.
In conclusion, we have demonstrated a significant burden of dyslipidemia and by implication insulin resistance in our ART-naive HIV-infected population. This can be a portent for future cardiovascular events. Dyslipidemia in ART-naive HIV-infected patients should be evaluated with a full lipid profile, and simple healthy lifestyle changes should be emphasized concurrent with other care given to this group of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.