
Abstract
Relationships between vitamin D, lipids, HIV infection, and HIV treatment (±antiretroviral therapy [ART]) were investigated with Women’s Interagency HIV Study data (n = 1758 middle-aged women) using multivariable regression. Sixty-three percent of women had vitamin D deficiency. Median 25-hydroxyvitamin D (25-OH vitamin D) was highest in HIV-infected + ART-treated women (17 ng/mL; P < .001) and was the same in HIV-uninfected or HIV-infected women without ART (14 ng/mL). Vitamin D levels were lower if efavirenz (EFV) was included in ART (15 versus 19 ng/mL; P < .001). The most common lipid abnormality was high triglycerides (≥200 mg/dL) in HIV-infected + ART-treated women (13% versus 7% of HIV-infected without ART and 5% of HIV-uninfected; P < .001), with a positive relationship between 25-OH vitamin D and triglycerides (95% confidence interval 0.32-1.69; P < .01). No relationships between 25-OH vitamin D and cholesterol were detected. Vitamin D deficiency is common irrespective of HIV status but influenced by HIV treatment. Similarly, vitamin D levels were positively related to triglycerides only in ART-treated HIV-infected women and unrelated to cholesterol.
Keywords
Introduction
Vitamin D is increasingly recognized as having a role in health and disease beyond its role in bone health. 1 –8 Low levels of 25-hydroxyvitamin D (25-OH vitamin D) have been associated with adverse effects on bone and mineral metabolism and cardiovascular risk factors of hypertension, obesity, diabetes, and metabolic syndrome. 9
Evidence is mounting that relatively high proportions of people have inadequate levels of vitamin D. 10 Cross-sectional population studies describe low vitamin D concentrations in children, young adults, especially African Americans, and middle-aged and elderly adults. 11 –15 The prevalence of deficiency has been estimated at approximately 36% in healthy young adults aged 18 to 29 years, 42% in African American women aged 15 to 49 years, 41% in outpatients aged 49 to 83 years, up to 57% in general medicine inpatients in the United States, and in 70% to 100% of hospitalized adults. 10 Analyses of National Health and Nutrition Examination Survey III data suggest even higher levels of insufficiency with levels <30 ng/mL in 80% to 90% of all adult African Americans, in 70% to 75% of Hispanics, and in 45% to 55% of Caucasian men and 45% to 65% of Caucasian women. 14 These population studies did not consider or report information on HIV status. Recent reports of vitamin D deficiency in HIV-infected populations have also appeared. Single centers report vitamin D deficiency in 41% to 90% of patients, with estimates varying by race, geography, and season, among other factors, including treatment with efavirenz (EFV). 16 –18 It is unclear whether vitamin D deficiency is more frequent in HIV-infected people than in comparable HIV-uninfected people or how HIV therapy influences vitamin D status.
In healthy people, variable relationships have been described between circulating 25-OH vitamin D levels and lipid levels, with reported inverse associations between vitamin D levels, triglycerides, and insulin resistance 19 –22 ; vitamin D levels and lipid subfractions 23 ; and vitamin D levels and low-density lipoprotein (LDL) cholesterol in atorvastatin-treated patients. 24 A recent report of HIV-positive women on antiretroviral therapy (ART) living in the tropics also found a significant inverse relationship between 25-OH vitamin D concentrations and total cholesterol but not LDL cholesterol. 18
We investigated the relationship of vitamin D to HIV status and HIV treatment, and lipid levels, including triglycerides, LDL cholesterol, and high-density lipoprotein (HDL) cholesterol in a nationally representative cohort of middle-aged, ethnically diverse HIV-infected and uninfected women enrolled in the Women’s Interagency HIV Study (WIHS).
Methods
Study Design
The WIHS is an ongoing long-term multicenter observational study of 3766 women who are HIV infected (further classified as on therapy or not receiving medication therapy for HIV) and women of similar age and ethnicity at risk of HIV infection. There were 2 recruitment periods, the first in 1994/1995 and the second in 2001/2002. For details on the recruitment and study demographics, see references 25 and 26. The WIHS participants have follow-up visits at 6-month intervals, which include interviewer-administered questionnaires, physical and gynecological examinations, and collection of biologic specimens (details available at http://statepiaps.jhsph.edu/wihs/. Accessed November 29, 2010). The cross-sectional study included 1760 WIHS participants whose sera were collected at visit 27 (October 1, 2007, to March 30, 2008) and stored for future analyses. Between October 2009 and January 2010, vitamin D levels were determined from the visit 27 stored sera using liquid chromatography and tandem mass spectrometry at Quest laboratories (Baltimore, Maryland; http://www.questdiagnostics.com/hcp/intguide/EndoMetab/EndoManual_AtoZ_PDFs/Vitamin_D_LCMSMS.pdf. Accessed November 23, 2010). Data were excluded for 2 participants due to laboratory errors; data from the remaining 1758 participants comprise the data set for analysis.
Statistical Methods
Characteristics were compared across 3 groups of WIHS participants: HIV-uninfected, HIV-infected on ART, and HIV-infected not on ART. Due to nonnormal distributions of 25-OH vitamin D and lipids, comparisons for continuous variables were made using nonparametric tests: Kruskal-Wallis (for 3 groups) and Wilcoxon (for 2 groups). Categorical variables were analyzed using Chi-square tests. Relationships between 25-OH vitamin D and triglycerides or LDL or HDL cholesterol were investigated individually using multivariate linear regression. Effects were examined both among the entire study sample and for the 3 study groups defined by HIV/ART status. Analyses comparing these groups allowed for adjustment of confounding variables unique to the HIV/ART group. Univariate (unadjusted) analyses were based on linear regression. Box plots by quartile of 25-OH vitamin D were also examined.
Confounding variables considered were body mass index (BMI), waist circumference, race, age, diabetes status, hepatitis C status, and use during the preceding 6 months of lipid-lowering drugs (LLDs) that have reported associations with 25-OH vitamin D (atorvastatin [Lipitor, Pfizer, New York, New York], 27 lovastatin [Mevacor, Merck, Sharp and Dohme, White House Station, New Jersey], 28 and rosuvastatin [Crestor, AstraZeneca, London, United Kingdom], 29 simvastatin [Zocor, Merck, Sharp and Dohme, White House Station, New Jersey] 30 ) and those without reported associations with 25-OH vitamin D (fluvastatin [Lescol, Novartis, Basel, Switzerland], pravastatin [Pravachol, Bristol-Myers Squibb, New York, New York], gemfibrozil [Lopid, Pfizer, New York, New York], fenofibrate [TriCor, Abbott and AbbVie, Abbott Park, Illinois], colestipol [Colestid, Pharmacia and Upjohn, New York, New York], cholestyramine [Questran, Par Pharmaceutical, Woodcliff Lake, New Jersey], colesevelam [Welchol, Daiichi Sankyo, Tokyo, Japan], niacin [Niaspan, Abbott and AbbVie, Abbott Park, Illinois], cerivastatin [Baycol, Bayer, Leverkusen, Germany], ezetimibe [Zetia, Merck, Sharp and Dohme, White House Station, New Jersey], vytorin [ezetimibe and simvastatin, PD-Rx Pharmaceuticals, Oklahoma City, Oklahoma], niacin XR and lovastatin [Advicor, Abbott and AbbVie, Abbott Park, Illinois], and Omega-3-acid ethyl esters [Lovaza, GlaxoSmithKline, Brentford, United Kingdom]). For the 2 HIV-infected groups, CD4 count and viral load were also included. Among HIV-infected ART-treated women, additional potential confounders included EFV during the preceding 6 months, tenofovir (TDF) during the preceding 6 months, and HIV medications taken during the preceding 6 months reported to increase cholesterol or triglycerides (US Food and Drug Administration-approved label or www.aidsinfo.nih.gov, primarily protease inhibitors, and other agents given in combination with ritonavir, RTV).
Multivariate linear regression was used for adjustment of confounders. First, we considered only those potential confounders with a univariate association (P < .1) with 25-OH vitamin D. Next, these were used as candidate variables in a stepwise model selection algorithm based on Akaike information criterion. This 2-step process was applied to each separate analysis with HDL, LDL, and triglycerides as the outcome for the whole sample and then by HIV/ART status.
To capture variability in the 2-step model selection process, the bootstrap procedure was applied to obtain confidence intervals and P values. 31 For each 10 000 bootstrapped samples, the entire 2-step process was applied. In univariate analyses, the bootstrap procedure was also applied to obtain inferences due to violations of the normality assumption based on the skewness in distributions of triglycerides, LDL, and HDL cholesterol.
Few LDL or HDL data were missing at visit 27 (2%-4%), and analyses did not account for missing values. For triglycerides, 19% of participants had missing measurements. Inverse probability of missing weights was applied in regression for these missing measurements. 32 Weights were estimated with logistic regression using the covariates listed previously. For potential confounding variables, the last observation carried forward was applied.
All analyses were performed in R (R Development Core Team, 2009. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL http://www.R-project.org).
Results
Participant Data
Table 1 provides the demographic and clinical characteristics of the 1758 participants and between-group comparisons. The study participants included 507 HIV uninfected, 358 HIV infected and not receiving ART, and 893 HIV infected and receiving ART. The HIV-infected participants were older, with the HIV-infected and therapy receiving group being the oldest. The HIV-infected and therapy receiving group had a higher proportion of non-African Americans than the other 2 groups. Waist circumference and BMI were largest in the HIV-uninfected group, with the HIV-infected and medication therapy receiving group having the smallest. CD4 count was higher and viral load was lower in the therapy receiving group than that of the no therapy group.
Characteristics of the 1758 WIHS Participants by HIV/ART Status.a
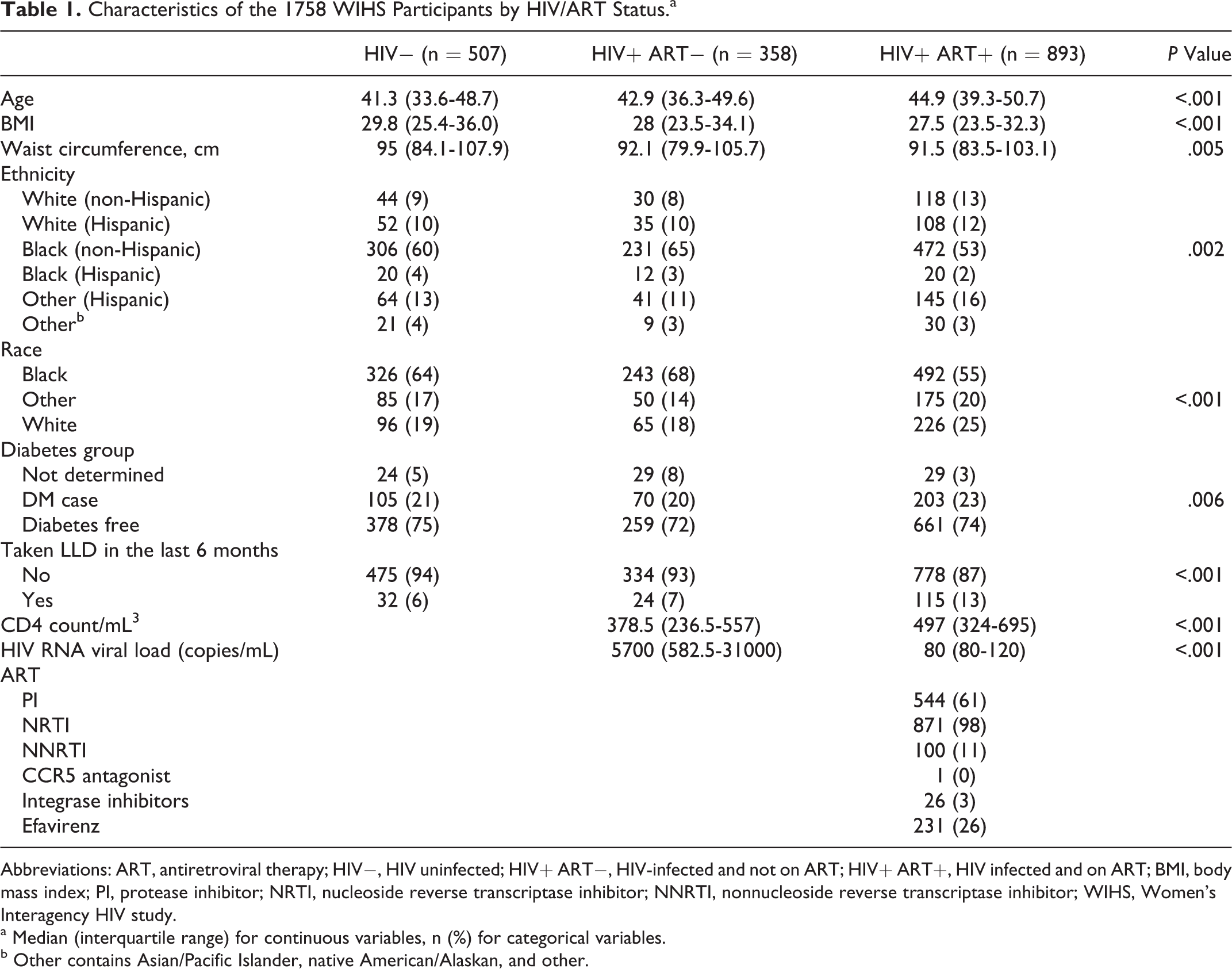
Abbreviations: ART, antiretroviral therapy; HIV−, HIV uninfected; HIV+ ART−, HIV-infected and not on ART; HIV+ ART+, HIV infected and on ART; BMI, body mass index; PI, protease inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; WIHS, Women’s Interagency HIV study.
a Median (interquartile range) for continuous variables, n (%) for categorical variables.
b Other contains Asian/Pacific Islander, native American/Alaskan, and other.
Vitamin D Data
Overall, 63% of WIHS participants had vitamin D deficiency (<20 ng/mL 25-OH vitamin D), 24% had insufficient vitamin D (20-30 ng/nL), and 13% had vitamin D replete (>30 ng/mL). We examined the vitamin D status irrespective of the presence or absence of HIV infection and whether HIV-infected women received treatment. Total serum 25-OH vitamin D was highest in the HIV-infected ART-treated group (median 17, interquartile range 11-26 ng/mL) compared to the untreated HIV-infected group (median 14, interquartile range 9-21 ng/mL) and the HIV-uninfected group (median 14, interquartile range 9-20 ng/mL; P < .001). The percentage of women with vitamin D replete or sufficient levels (30+ ng/mL) was also highest, and the percentage of women with vitamin D deficiency (25-OH vitamin D <20 ng/mL) was lowest in the HIV-infected ART-treated group. In contrast, the distribution of vitamin D deficiency, insufficiency, and sufficiency were the same in the HIV-uninfected and HIV-infected but untreated groups (Figure 1).

Distribution of 25-hydroxyvitamin D by HIV and HIV treatment status. ART indicates antiretroviral therapy; HIV−, HIV uninfected; HIV+ ART−, HIV-infected and not on ART; HIV+ ART+, HIV-infected and on ART.
Lipid Data
Table 2 presents the lipid data. Elevated triglycerides were the most common lipid abnormality. High triglycerides (>200 mg/dL) were seen in 25% overall, with twice as many of the HIV-infected ART-treated women with high triglycerides compared to the other groups. Median LDL cholesterol was also highest in the HIV-infected women receiving ART compared to HIV-uninfected or HIV-infected and untreated women. The proportion with high-LDL cholesterols, however, was the same for the 3 WIHS groups, possibly confounded by the higher use of lipid-lowering medications in the HIV-infected ART-treated women. HIV-infected ART-treated women with high triglycerides had the highest use of LLDs (32%) but the use of lipid-lowering medications was low overall. Of the participants with high-LDL cholesterol, only 17% reported having taken an LLD in the preceding 6 months. Median-HDL cholesterol was low in all groups, lowest in the untreated HIV-infected group, followed by the HIV-infected ART-treated group.
Lipid Data by HIV, HIV Treatment, and LLD Status.a

Abbreviations: ART, antiretroviral therapy; HIV−, HIV uninfected; HIV+ ART−, HIV infected and not on ART; HIV+ ART+, HIV infected and on ART; LDL, low-density lipoprotein; HDL, high-density lipoprotein; LLD, lipid-lowering drug.
a Normal, borderline high, high LDL, and triglyceride levels were based on the National Cholesterol Education Program guidelines found at http://www.nhlbi.nih.gov/health/public/heart/chol/wyntk.pdf. Accessed December 01, 2010.
b Data are median (interquartile range) for continuous variables and n with percentages in parentheses for categorical variables.
Vitamin D and Lipid Relationships
No relationships were detected between 25-OH vitamin D and cholesterol concentrations, while a significant positive relationship between vitamin D levels and triglycerides was detected. Statistical results for relationship analyses of vitamin D and lipids (adjusted and unadjusted estimates and 95% confidence intervals) are provided in Table 3. Considering all WIHS participants, a positive association between 25-OH vitamin D and triglycerides was detected in the multivariate adjusted analysis, and each nanogram per milliliter increase in 25-OH vitamin D was associated with 0.76 mg/dL increase in triglycerides (P < .01; Table 3 ). Further examining this relationship by HIV and ART treatment status, a significant association was detected between vitamin D and triglycerides in the HIV-infected and receiving medication therapy group (adjusted estimate was 1.53; P < .01). Box plots of triglycerides by quartile of vitamin D by HIV and ART therapy status are presented in Figure 2 to further illustrate this relationship.

Box plots of triglycerides by quartile of vitamin D by HIV/medication therapy status. (A) HIV uninfected, (B) HIV infected and not on ART, and (C) HIV infected and on ART. ART indicates antiretroviral therapy.
Relationships Between Circulating 25-Hydroxyvitamin D and Triglycerides, LDL, and HDL Cholesterol.a,b

Abbreviations: ART, antiretroviral therapy; HIV−, HIV uninfected; HIV+ ART−, HIV infected and not on ART; HIV+ ART+, HIV infected and on ART; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
a Data in parentheses are 95% confidence intervals.
b Adjusted estimates are adjusted for confounding variables using multivariable regression.
c P value < .001.
d P value < .01.
e Adjusted for BMI, race, age, taken lipid-lowering drug in the last 6 months, hepatitis C status, waist circumference, and HIV/therapy status.
f Adjusted for BMI, race, age, waist circumference, taken a lipid-lowering drug in the last 6 months known to increase vitamin D levels, CD4 count, taken an NNRTI in the last 6 months, and, taken a PI in the last 6 months.
g P value < .05.
Multivariate adjusted and unadjusted estimates of the effects of vitamin D on LDL were positive in direction but did not reach significance (P = .08 and P = .19, respectively). Similarly, both adjusted and unadjusted estimates of the effects of vitamin D on HDL were positive but did not reach significance (P = .13 and P = .09, respectively).
Vitamin D and EFV
The reported association between EFV and 25-OH vitamin D 33 was investigated, and the median 25-OH vitamin D level in HIV-infected women taking EFV was 15 (interquartile range 10-24 ng/mL) compared to 19 (interquartile range 12-28 ng/mL) in HIV-infected women receiving ART that did not include EFV (P < .001).
Discussion
There is a rapidly evolving literature regarding the role of vitamin D in health and disease. With increased attention focused on vitamin D in both the media and scientific literature, widespread measurement of circulating 25-OH vitamin D concentrations has occurred. It appears that significant fractions, if not the majority of middle-aged and older adults living in western industrialized nations or far north of the equator, have levels of circulating 25-OH vitamin D that are considered inadequate. Recognized factors associated with lower 25-OH vitamin D concentrations include older age, female sex, low sun exposure, dark skin, genetic disorders of the vitamin D receptor, higher BMI, gastrointestinal absorption disorders, and liver or renal disease. 1,7,10,15,34
Vitamin D status is being addressed in HIV-infected patients, in part due to the recognition of increased incidence of osteoporosis during chronic treatment of HIV. 35 –39 Low levels of vitamin D have been reported in 41% to 90% of HIV-infected patients. 16 –18 This incidence appears to be higher than the expected rate of about 40% found in middle-aged men and women in US population studies but similar to the rates in older people or hospitalized patients or those of African American and Hispanic ethnicity. 7,10 No report, however, has compared the relative frequency of low vitamin D status in HIV-infected women in relationship to treatment status or to age- and ethnicity-matched people without HIV with similar risk of HIV infection.
As previously reported, 63% of WIHS participants had vitamin D deficiency, with vitamin D deficiency more frequent in the HIV-infected than in HIV-uninfected women, 40 with traditional vitamin D deficiency risk factors of older age, African American or Hispanic ethnicity, and higher BMI detected in these groups. 33 The current investigation expands on these analyses by considering the frequency of vitamin D inadequacy states both by HIV infection status and by HIV treatment status. Vitamin D concentrations were highest in the HIV-infected ART-treated women, despite their higher age. Unexpectedly, there were no differences in prevalence of deficient, insufficient, or vitamin D replete status in the HIV-uninfected women and HIV-infected women not receiving medication therapy. These data may be confounded slightly by small differences in proportions of African Americans and Hispanics in the groups, nonetheless, it appears that HIV infection alone does not appreciably increase the prevalence of vitamin D deficiency and that vitamin D deficiency was present in the overwhelming majority of these middle-aged women of diverse ethnicity.
A more novel aspect of our investigation was examining the relationship between vitamin D and lipids in relation to HIV status and HIV therapy. Low 25-OH vitamin D levels have been associated with the cardiovascular risk factors for hypertension, obesity, diabetes, and metabolic syndrome. 9 Higher rates of myocardial infarction in men have been related to lower levels of vitamin D in the Health Professionals Follow-up Study, 41 and lower levels of vitamin D and vitamin D precursor have been related to all-cause and cardiovascular mortality in men and women evaluated for cardiovascular disease. 42 In the Framingham Offspring study, participants with vitamin D deficiency and hypertension were about twice as likely as people without hypertension and vitamin D deficiency to have a cardiovascular event during the study. 43 Serum vitamin D levels have also been inversely correlated with the degree of coronary artery calcification 44 and with the prevalence of peripheral artery disease, hypertension, diabetes, obesity, and high serum triglyceride levels. 14,45 Levels of 25-OH vitamin D have also been reported to be lower in elderly patients with stroke than in controls. 46 These data have led some to hypothesize that vitamin D supplementation can decrease cardiovascular morbidity and mortality, with a large randomized double-blind study underway to test this hypothesis (www.vitalstudy.org).
With the introduction of ART, HIV infection has become a chronic disease. Atherosclerosis has been recognized at an earlier age in chronic HIV-infected men undergoing treatment than in uninfected men. 47,48 A number of potential underlying mechanisms that include chronic inflammation likely contribute to the early atherosclerosis but lipid abnormalities that accompany treatment of HIV infection with ART may be considered a cardiovascular disease risk equivalent. 49 We have reported that supplemental vitamin D lowered LDL cholesterol in patients with varying degrees of inadequate vitamin D status and lipid abnormalities, suggesting a relationship between vitamin D and cholesterol levels. 24 The concept that vitamin D affects lipid concentrations is also supported by data on seasonal variations in lipid levels, with total and LDL cholesterol, triglycerides, and lipoprotein A highest in the winter when sun exposure is usually lowest. Variable relationships between vitamin D concentrations and lipid concentrations have been described but no clear conclusion appears to exist, 21,50 –52 but one cross-sectional investigation in HIV-infected women in the tropics suggested an inverse relationship between vitamin D and total cholesterol concentrations. 18
We, thus, hypothesized that there would be an inverse relationship between vitamin D levels and cholesterol and triglyceride levels. After correcting for other factors known to affect lipid status, no relationships were detected between LDL cholesterol or HDL cholesterol and vitamin D concentrations. The only significant relationship detected was a positive relationship between triglyceride and vitamin D concentrations (ie, higher triglyceride concentrations at higher vitamin D concentrations). When this relationship was further analyzed with consideration of HIV and HIV treatment status, it was confined to the HIV-infected participants receiving ART. Our study did not address potential mechanisms by which HIV treatment could increase triglycerides, but others have suggested that increases in weight, lipids, and triglycerides reflect a positive treatment effect; while pharmacologic data suggest that a number of medications used in ART produce increases in cholesterol or triglycerides, independent of HIV status. Our analyses were stratified by disease status within the HIV-infected and HIV treatment groups and suggest the treatment regimens as the probable strongest factor influencing triglycerides. The conclusions differ from those recently reported in which a negative relationship was detected between total cholesterol (LDL and HDL cholesterol) and 25-OH vitamin D concentrations in HIV-infected ART-treated women in Brazil. 18 It should be noted that on average 25-OH vitamin D levels were higher in the Brazilian women, and vitamin D deficiency (25-OH vitamin D <20 ng/mL) was present in 13% compared to 63% of HIV-infected ART-treated women in WIHS and 41% in Brazil had levels <30 ng/mL compared to about 87% in our sample. Antiretroviral therapy regimens differed slightly with somewhat lower use of protease inhibitors in the Brazilian sample, but data suggest that environmental factors such as sunshine and not HIV infection are more likely responsible for the marked differences in circulating 25-OH vitamin D. Unfortunately, neither study directly examined sunshine exposure. It should be noted that in the Brazilian cohort, a negative relationship was detected for total cholesterol and vitamin D but no relationship was detected for vitamin D and LDL or HDL cholesterol. The relationships between vitamin D and LDL and HDL cholesterol were negative in direction. Although lower LDL cholesterol may reduce cardiovascular risk, lower HDL cholesterol is considered a cardiovascular risk factor. Therefore, interpreting the trend for total cholesterol does not seem clinically relevant. We examined LDL and HDL cholesterol trends individually to allow evaluation in the context of cardiovascular risk.
Cardiovascular and metabolic effects of antiretroviral agents have been reviewed. 49,53 To summarize, increases in triglycerides and to a lesser extent cholesterol have been associated with the protease inhibitors RTV, amprenavir (APV), lopinavir (LPV), tipranavir, fos-amprenavir (FPV), nelfinavir (NFV), indinavir (IDV), saquinavir (SQV) with atazanavir (ATV), and darunavir having lesser to no effects. Effects of other classes of antiretroviral agents are more variable. The nonnucleoside reverse transcriptase inhibitor (NNRTI) EFV can also raise blood lipid levels. Antiretroviral drugs with less impact on lipids include the NNRTIs etravirine and nevirapine (NVP), the CCR5 antagonist maraviroc, and the integrase inhibitor raltegravir. In our WIHS sample, protease inhibitors were used in 61% of HIV-infected ART-treated participants. Nonnucleoside reverse transcriptase inhibitors were used in 98% of HIV-infected ART-treated patients, and NNRTIs were administered to 26% of HIV-infected ART-treated patients. The use of NNRTI was low (11%) and that of integrase inhibitors rare (3%). The sample size and combined use of multiple agents precluded attempts to identify effects of individual agents or regimens on lipids in our analyses.
Lipid abnormalities were observed for triglycerides in 10% of WIHS participants with fasting triglycerides of 150 to 199 mg/dL and 10% with levels ≥200 mg/dL. Borderline high-LDL cholesterol (130-159 mg/dL) was present in 12%, and high LDL cholesterol (≥160 mg/dL) was present in 4%. Most of these women did not report taking LLDs. The lack of relationships between vitamin D and LDL and HDL cholesterol and the positive direction of the relationship between vitamin D concentrations and triglycerides suggest that correction of vitamin D inadequacy states in HIV-infected patients will not improve lipid abnormalities and other approaches should be considered.
There are limitations to our data and analyses. Single time point cross-sectional analyses were performed, and the data may not reflect within-individual relationships. Our considerations of lipid and triglyceride levels did not include dietary information. Statistical adjustments may not have completely accounted for confounding factors. Finally, the data do not address the effects of the correction of vitamin D inadequacy states. Nonetheless, the data convincingly demonstrate that vitamin D deficiency is common in middle-aged women with HIV infection or at risk for HIV infection, that treatment of HIV will not correct vitamin D inadequacy, and that correction of vitamin D inadequacy is not likely to correct the lipid abnormalities that accompany HIV treatment.
In conclusion, vitamin D deficiency is common in middle-aged women with HIV infection or at risk for HIV infection, high triglycerides are the most common lipid abnormality in HIV-infected women treated with ART, and triglycerides were positively associated with vitamin D levels. Relationships between vitamin D and cholesterol were not detected. There is a continued need to address vitamin D inadequacy states, ART metabolic effects, and the management of lipid disorders in people infected with HIV.
Footnotes
Acknowledgments
For this study, data were collected by the Women's Interagency HIV Study (WIHS) Collaborative Study Group with centers (Principal Investigators) at New York City/Bronx Consortium (Kathryn Anastos); Brooklyn, New York (Howard Minkoff); Washington, DC Metropolitan Consortium (Mary Young); The Connie Wofsy Study Consortium of Northern California (Ruth Greenblatt); Los Angeles County/Southern California Consortium (Alexandra Levine); Chicago Consortium (Mardge Cohen); Data Coordinating Center (Stephen Gange). The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The WIHS is funded by the National Institute of Allergy and Infectious Diseases (UO1-AI-35004, UO1-AI-31834, UO1-AI-34994, UO1-AI-34989, UO1-AI-34993, and UO1-AI-42590) and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (UO1-HD-32632). The study is cofunded by the National Cancer Institute, the National Institute on Drug Abuse, and the National Institute on Deafness and Other Communication Disorders. Funding is also provided by the National Center for Research Resources (UCSF-CTSI Grant Number UL1 RR024131). Funding also provided by RO1 AG 15982 and funds from the Jewish Home, San Francisco.