
Abstract
We compared perceptions of partner HIV status to HIV test results in a cross-sectional study of sexual networks of men who have sex with men (MSM) in Atlanta. We then examined differences between black and white MSM in the predictive value of perceived partner status. We recruited men (“seeds”) using time-space venue sampling. These seeds then referred up to three partners, who could also refer partners. All participants reported sexual behavior and HIV status for recent partners and received HIV tests. For partners who enrolled, we compared laboratory diagnoses to their partner’s perception of their status. Black MSM who perceived themselves to be HIV negative were more likely than perceived-negative white MSM to have a positive partner among those they perceived to be HIV negative or whose status was unknown to them (OR=6.6). Furthermore, although frequency of unprotected anal intercourse (UAI) was similar by race, black men were more likely to have had UAI with an unknown-positive partner (OR=9.3).
Introduction
In the United States, HIV continues to disproportionately affect men who have sex with men (MSM). Despite being less than 5% of the population, 1 MSM accounted for 63% of new HIV infections and 78% of new infections among men, from 2007 to 2010. 2 In addition, racial disparities among this group are profound; young black MSM, aged 13 to 24 years, represented a majority of new HIV infections among MSM in the United States during the same period. 2 The disparity in Atlanta, Georgia, is particularly stark. HIV prevalence among black MSM in a recent cohort study was 43.4% compared with only 13.2% of white MSM. 3 Among MSM aged 18 to 24 years, prevalence was 30.1% and 5.6%, respectively. 3
Despite disparities in HIV incidence, researchers have found few behavioral differences between black and white MSM.4 –7 However, HIV-positive black MSM may be less likely to know their HIV status compared to white men,4,5,8 and serodisclosure is less common among those who have been diagnosed HIV-positive.4,9 Among men who previously tested HIV negative but who have not had a recent test, incorrect serodisclosure may also result in a greater proportion of partners of black MSM misperceiving them to be HIV negative. 8
Testing and disclosure have an impact on HIV risk. Specifically, the effectiveness of serosorting and seroadaptation, or selecting sexual partners and sexual activities or roles based on the HIV status of one’s partner, depends on accurate knowledge of each partner’s serostatus. 10 Although some researchers have cautioned against serosorting,11,12 studies and models have indicated that it can be an effective method of reducing HIV transmission compared to having unprotected anal intercourse (UAI) with men of unknown or discordant statuses.13,14 To make it a viable option for risk reduction, individuals must know their own HIV status, accurately disclose their status, and learn their partner’s status before making a decision about which sexual activities to engage in (if any), which role to take (if engaging in anal sex), and whether to use condoms. 10
Although serosorting behavior appears to be equally common among both white and black MSM, 9 findings from some studies indicate racial differences in its effectiveness in preventing HIV, with serosorting being less protective among black MSM than among white MSM.4,15 Reasons for the difference in the protective effect of serosorting may be due to different rates of HIV disclosure among white and black MSM 4 or inaccurate knowledge of HIV status.8,15 Although researchers have examined the differences in rates of testing,15 –20 serodisclosure,9,21 –23 and inaccurate serodisclosure, 8 little is known about the proportion of partners for whom perceived HIV status is incorrect, or the predictive value of perceived partner HIV status, among black and white MSM. In this article, we examine the accuracy of perceived partner HIV status at last sex among a sample of black and white MSM in Atlanta, Georgia, using HIV test results from a sexual network study.
Methods
Study Procedures
The Men’s Atlanta Networks (MAN) Project was a cross-sectional study of sexual networks among MSM in Atlanta, Georgia, that was conducted from April 2011 to March 2013. We recruited participants using a chain referral sampling method. 24 “Seed” participants referred their recent male partners, who could then enroll and refer partners, as well. This method yielded chains of up to 5 recent sex partners. Seeds were recruited using time–space venue sampling. 25 The venue sampling frame was based upon that used for the second wave of the National HIV Behavioral Surveillance System (NHBS) and another cohort study of MSM conducted by the Emory University team.3,25
Seeds were eligible if they resided in the Atlanta metropolitan area, had sex with a man in the 3 months prior to the survey, were non-Hispanic black or white, and were aged between 18 and 40 years. Each seed could refer up to 3 recent male sexual partners, defined as men with whom they had sex in the previous 12 months; preference was given to partners within the previous 6 months, if available. Referred partners were eligible if they were aged ≥18 years, lived in the Atlanta metropolitan area, and had sex with the participant who referred them; partners could be of any race and ethnicity to accurately reflect the networks of black and white MSM. This study was approved by the Emory University Institutional Review Board (00047855).
Measures
Following informed, written consent, participants received tests for HIV, gonorrhea, chlamydia, and syphilis, and they completed a self-administered computer questionnaire. The survey questions included demographic information and dyadic data collection that assessed sexual behavior and partner characteristics for up to 10 sexual partners from the 12 months prior to enrollment. Individuals also reported their perceived HIV status prior to receiving their rapid HIV test result, and HIV tests were administered regardless of self-reported HIV status.
Participants provided the age, race/ethnicity, and perceived HIV status of each partner, if known. They also reported details about their last sexual encounter with the partner, including whether they had anal sex, and, if so, their anal sex roles and whether condoms were used. Questions about last sex also included whether it was in the context of group sex and if alcohol or drugs were used. The computer-assisted survey was implemented in SurveyGizmo v.2.6.
Participants also provided names and other descriptors of partners. During a referral session with the study counselor in which select survey responses were reviewed, participants referred eligible partners to the study from the pool of sexual partners described in the survey. Referred partners were contacted by the participant himself, and by study staff if desired, to assess interest in participation. Thus, participants’ dyadic survey data were able to be directly linked to the study data of referred partners who later enrolled. For enrolled partners, we were able to link a subset of their dyadic survey data back to the participants who referred them, using probabilistic name matching with LinkPlus 26 and manual review. Using detailed partner and participant data (e.g. name, phone number, age, and e-mail address), LinkPlus produced a list of potential pairs and the probability that they were the same person. We reviewed each match and made our final determination based on how well the characteristics and information for each person in the pair agreed. These linked dyadic responses formed the basis of our analysis of perceived and actual partner HIV statuses.
Statistical Analyses
We compared demographic characteristics of white and black participants using frequencies and chi-square tests or, in cases where the expected cell counts were <5, Fisher exact tests. We then focused on the set of reported partnerships where both members were enrolled as part of the chain referral, for which linked dyadic data were thus available.
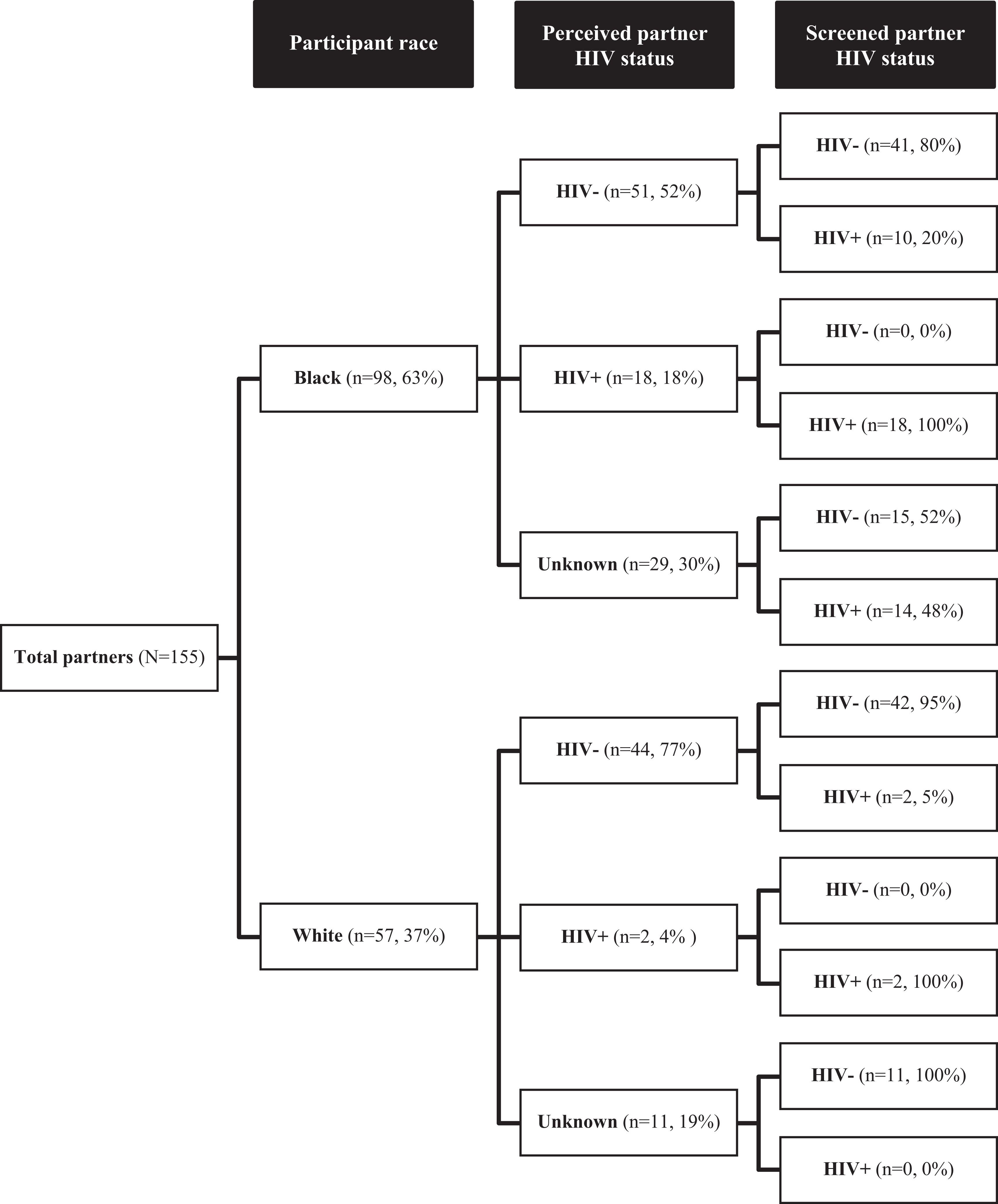
We computed the joint distribution of participant-perceived and actual partner HIV statuses separately for black and white participants. We depicted this distribution using a tree diagram that first shows perceived HIV status and within each perceived status, the actual HIV statuses per HIV screening-depicted differences in perceived and laboratory-diagnosed partner HIV status.
We compared the odds of having an HIV-positive partner among black and white MSM, using odds ratios (ORs) and 95% confidence intervals (CIs), further stratifying by perceptions of partner’s HIV status (HIV negative, HIV positive, and HIV unknown) and whether they engaged in UAI at last sex.
Finally, we summarized the characteristics of participants, partners, and dyads, in which the partner’s HIV-positive serostatus was unknown to the participant, either because he was perceived to be HIV negative or his status was not disclosed. To focus this analysis on partnership with HIV transmission risk, we restricted the participant sample to those who perceived themselves to be HIV negative at the start of the study. Characteristics included age and screened HIV status of participant; age, perceived HIV status, and race and ethnicity of the partners; and whether they discuss HIV status, whether the partner was main or casual, whether they lived together, whether they planned to have sex again, whether they met online or off-line, and whether they used a condom at last sex. We then compared the proportion of participant-unknown partner seropositivity, participant characteristics, partner characteristics, and characteristics of the dyad using chi-square analyses or Fisher exact tests in the same manner described above. Data were analyzed using SAS v9.3. 27
Results
There were racial differences in proportions of every demographic criterion (Table 1). Black participants were younger; more likely to identify as bisexual; more likely to have less than a college education and a lower annual income; and more likely to perceive themselves to be, and be diagnosed, HIV positive than white participants.
MAN Project Participant Characteristics, by Race.a

Abbreviations: GED, general equivalency diploma; MAN, Men’s Atlanta Networks.
aN = 142.
In the tree diagram of perceptions and true HIV statuses of male sexual partners of black and white men (Figure 1), the first branch represents the percentage of all partners who were partners of black and white men in our sample; the second shows the percentage of partners of black and white men who were perceived by participants to be HIV negative, HIV positive, or whose status was unknown; and the third shows the percentage of partners of each perceived status that were screened as HIV negative or HIV positive when they enrolled in the study. While the predictive value of perceiving a partner to be HIV positive was 100% for both black men (Table 2) and white men (Table 3), the predictive value of perceiving a partner to be HIV negative or not knowing his HIV status was 96% for white men (Table 3) and only 70% for black men (Table 2).
Perceived and laboratory diagnosed HIV status of enrolled partners of black and white participants in the MAN Project (N = 142 participants; N = 155 enrolled partners).
Perceived and Laboratory Diagnosed Partner HIV Status and Predictive Value among Black Participants in the MAN Project.a

Abbreviation: MAN, Men’s Atlanta Networks.
aN = 83 participants; N = 98 partners.
Perceived and Laboratory Diagnosed Partner HIV Status and Predictive Value among White Participants in the MAN Project.a
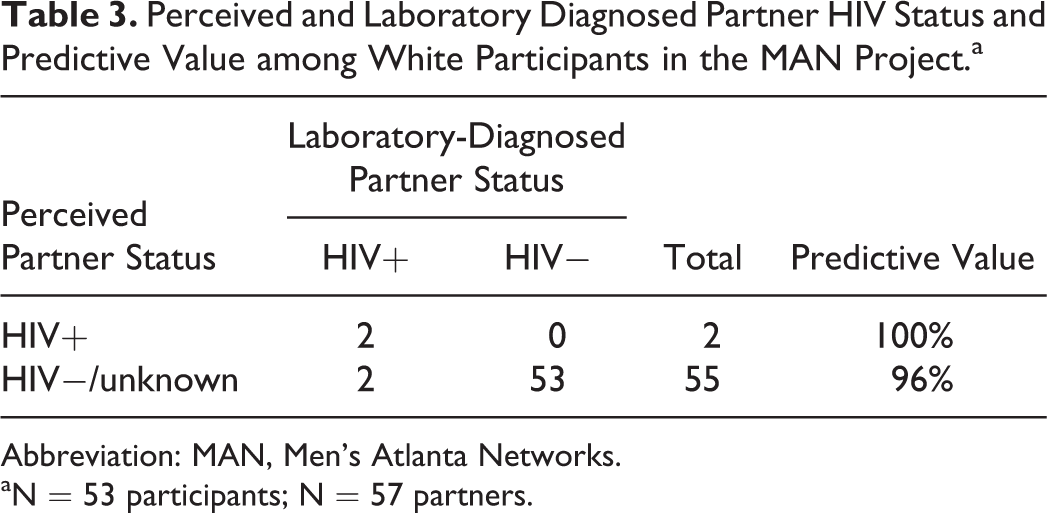
Abbreviation: MAN, Men’s Atlanta Networks.
aN = 53 participants; N = 57 partners.
Perceived knowledge of partner serostatus was not significantly different by race (OR: 1.8, 95% CI: 0.8-3.9). Prevalence of HIV among partners was 41% for black men and 6% for white men (OR: 9.9, 95% CI: 3.3-29.6). When we restricted our sample to men who reported being HIV negative at baseline, 22% of the partners of black men and 5% of the partners of white men were HIV positive (OR: = 4.8, 95% CI: 1.3-17.6). Further, among partners whom men perceived to be HIV negative or whose status was unknown to them, partner HIV prevalence was 21% for black men and 4% for White men (OR = 6.6, 95% CI: 1.4-30.9).
Regarding HIV risk behavior, odds of UAI at last sex among black and white participants who perceived themselves to be HIV-negative did not differ (OR: 0.6, 95% CI: 0.3-1.3). In addition, no HIV-negative men had UAI at last sex with someone who they perceived to be HIV positive, and, among partners with whom participants had UAI at last sex, the odds of having an HIV-unknown partner did not differ by race (OR: 2.1, 95% CI: 0.7-7.0). However, 25% of the UAI partners of self-perceived HIV-negative black participants were unknown to be HIV positive, compared to only 3% of UAI partners of HIV-negative white participants (OR: 9.3, 95% CI: 1.1-81.8; Table 4).
Number and Percentage of Unknown-positive Partners of Participants Who Reported Being HIV Negative at Baselineb in the MAN Project, by Participant Race and Select Characteristics.c

Abbreviations: MAN, Men’s Atlanta Networks; N/A, not applicable; UAI, unprotected anal intercourse.
aN = 114.
bN = 98.
cTotals represent the number of partners among black or white participants in the category. Percentages are based on the number of those partners who were diagnosed HIV positive. P values are based on chi-square tests or, when any expected cell counts were less than 5, Fisher exact tests.
dParticipants were tested as part of the study. Although the table is restricted to men who perceived themselves to be HIV negative or who did not know their HIV status at baseline, these categories represent their screened HIV status.
Black and white participants were different in the number and percentage of partners who were diagnosed with HIV among those who were perceived to be either HIV negative or whose status was unknown to the participant (Table 4). All of the black men who were unaware that they were HIV-positive also had partners who were HIV positive. Among the 13 unknown-positive partners of black men, 7 (54%) were unaware of their status. However, both of the unknown-positive partners of white men were aware of their status.
At the dyad level, black participants who perceived themselves to be HIV-negative or who did not know their HIV status had a statistically significantly higher percentage of HIV-positive partners among those with whom they discussed HIV status (P = .034), among their casual partners (P = .015), among partners they planned to have sex with again (P = .029), and among partners whom they met off-line (0.006) compared with white participants who did not perceive themselves to be HIV positive (Table 4). The percentage of HIV-positive partners among main partners who were perceived to be HIV negative or whose status was unknown was not significant or was the percentage among participants’ cohabitating partners.
Discussion
This analysis is unique because we have both participants’ perceptions of partners’ HIV statuses and their partners’ HIV screening results. We found that black men had higher odds of having an HIV-positive partner than white men, including among men they perceived to be HIV negative or whose HIV status they did not know. Among black participants who self-reported being HIV negative, approximately 20% of partners whom they believed to be HIV negative or whose HIV status was unknown were HIV positive compared to only 4% of the partners of white men. All partners who were perceived to be HIV positive were confirmed to be HIV positive by laboratory testing. Thus, regardless of their perception of their partner’s status, black men were more likely to have an HIV-positive partner than white men.
Our findings are consistent with previous studies that found greater HIV prevalence,3,28 more unknown HIV seropositivity, 4 and more inaccurate serodisclosure 8 among black MSM. HIV prevalence in our sample was greater among black MSM; 43% of black participants and 7% of white participants in our sample were screened HIV positive. Of the HIV-positive black men, 32% were unaware of their HIV status prior to their diagnosis, while all HIV-positive white men were previously aware. Similarly, half of HIV-positive partners of black MSM were unaware of their positive status. This is consistent with the study of Wei et al, 9 which found greater rates of undiagnosed HIV-positive status among black MSM, and that of MacKellar et al, which found more incorrect serodisclosure among the partners of black MSM due to infrequent testing. 8
The higher prevalence of undiagnosed seropositivity among black participants and partners lends support to the hypothesis of Golden et al 15 that less knowledge of HIV status, combined with race-assortative sexual mixing, may explain why serosorting is not protective for black men. Racial differences in the accuracy of perceived partner status existed even when participants had discussed HIV status with their partners, which suggests that there are racial differences in either partners’ knowledge of their own status, partner disclosure, or communication style between participants and partners. Knowing a partner’s status was more effective than being unsure; however, there were relatively fewer HIV-positive partners among those whom Black participants perceived to be HIV negative compared with those whose HIV status was unknown. Furthermore, all men who perceived their partners to be HIV positive were accurate.
Although perceiving a partner to be HIV negative may reduce the chance of having an HIV-positive partner for black MSM over not knowing his status, the effectiveness of serosorting as a risk reduction strategy among this group is still questionable. Golden et al 15 found that serosorting was an effective risk reduction strategy for white men but not for black men. The effectiveness of serosorting may be minimal if one is less likely to use condoms with partners who are perceived to be HIV negative. If we compare only UAI behavior, however, the results from another sexual networks study are consistent with our findings. The investigators of Brothers y Hermanos found that, among Latino and black MSM, having UAI with only HIV-negative men versus not restricting UAI to only HIV-negative men was associated with reduced odds of seroconversion, although 4% of serosorters still tested positive. 29 Similarly, in our study, although men did not engage in UAI with men they knew to be HIV positive, the percentage of HIV-positive partners, among those who were believed by participants to be HIV negative, was still high enough to warrant caution; regardless of the partner’s true HIV serostatus, men who perceived their partners to be HIV negative engaged in UAI the same proportion of the time, which is riskier for black MSM because of their higher prevalence of HIV-positive partners.
Our study has several limitations due to its network design. First, since our data include reflexive reports, or enrolled individuals who report about each other, the data are correlated. Second, given that there are chains of participants, two individuals might report information about the same third individual, in which case their reports and their partner’s status would also be correlated. In this case, individuals who discussed their HIV statuses before having sex would both be more likely to accurately report their statuses, but those who did not discuss HIV status before sex would both be unlikely to report knowing the other’s HIV status. Similarly, two men who were both told an incorrect HIV status by the same man would both be incorrect. Regardless, these reflect true misperceptions among our sample and were not seen as a threat to the validity of our findings.
The way that men were recruited to the MAN Project may also bias the results. Given that individuals referred their partners, it may be that the partners who enrolled in the study were more familiar with one another than the partners who did not. This may result in a greater proportion of main partners or a greater degree of closeness between the men in our sample and their sexual partners. However, even if this is the case, then the findings regarding proportions of incorrect serostatus perceptions may be higher in a general sample than what we observed.
Finally, our subsamples of white and black participants differed on every demographic characteristic, some of which may have confounded the association between race and the accuracy of perceived partner status. Due to our small sample size, we were not able to conduct analyses to adjust for these factors. Future studies designed specifically to study serostatus disclosure and accuracy of perceptions should adjust for cofactors such as age and education.
Our findings are both intuitive and alarming. Among black participants, approximately half of the HIV-positive partners whom they perceived to be HIV negative and half of the partners whose HIV status they did not know were aware of their HIV-positive status at the time of diagnosis. Future studies should examine how men discuss HIV status and how this influences their belief in their partners’ serodisclosures. Wei et al 9 found that Asian and black men reported being “completely confident” in their partner’s HIV status at lower rates compared with men of other races and ethnicities, and that black and Latino men had the highest percentages of men who were unsure of their own HIV status. Black men also reported that they were not confident at all in 18% of partnerships, the highest of any racial/ethnic group. 9
Our data suggest that increasing HIV testing and serodiscussion between black MSM and their partners may reduce disparities in HIV incidence between black and white MSM. Approximately half of the perceived-negative or unknown-status partners of black MSM who were HIV-positive did not know their status. Because of this, even serodiscussion was not as effective in improving perceptions of HIV status among black participants as it was among white participants. Although data suggest that men who avoid disclosing do not necessarily reduce HIV transmission risk behaviors, Golden et al 30 found that HIV-negative men were more likely to use condoms with men whom they knew to be HIV positive. Furthermore, men who discover that they are HIV positive may adapt their behavior to avoid onward transmission of HIV. 31
Although testing might reduce disparities to an extent, half of the perceived-negative or unknown-status partners of black MSM knew their HIV status, which suggests that changes must be made to current HIV serodiscussion practices among black MSM and their partners, by starting the discussion, promoting accurate serodisclosure among HIV-positive men, or improving clarity when discussing HIV status. Bird and colleagues 21 found that HIV-positive black men were less likely than white men to disclose HIV status to HIV-negative, HIV-unknown, and other HIV-positive partners, but that HIV-positive black men who did disclose were less likely to engage in UAI with HIV-negative and unknown-status men. 21 Incorrect beliefs about partner’s HIV status have implications for gaps in HIV testing as well. If men do not believe that they have been at risk for HIV infection, they may be less likely to test. This pattern may then be self-perpetuating.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Eunice Kennedy Shriver National Institute for Child Health and Human Development R01HD067111, National Institute of Mental Health R01MH085600, and NIH P30AI050409 – the Emory Center for AIDS Research.