
Abstract
Background:
Age is a key determinant of mortality due to diseases including HIV infection.
Methods:
A retrospective and descriptive cohort study used a computerized database to compare HIV-infected patients diagnosed in late adulthood to a group of patients diagnosed before their 49 years of age, without matching the characteristics of HIV infection. The study included patients who visited the day hospital (outpatient clinic) of the Sanou Souro Teaching Hospital of Bobo-Dioulasso, in Burkina Faso, from January 2007 to December 2011. Older adults were defined as those aged 50 years and more.
Results:
Participants in the study consisted of 2572 patients (265 older adults and 2307 young patients living with HIV. Based on Markov chain method, 32.1% of the older adults living with HIV were found to be seroconvert at 50 years or older. The median follow-up time on antiretroviral treatment (ART) was 32.7 months (range 0.03-65.4 months). Two hundred and ninety-five (11.5%) patients died, including 21.1% of older adults and 10.4% of young (P < .01). World Health Organization stage 3 or 4 and the lowest CD4 count reached <200 cells/mm3 were the factors associated with early mortality of older adults on ART.
Conclusion:
Mortality rate of older adult patients living with HIV in Burkina Faso is high. Early diagnosis, early treatment, and primary prevention of HIV infection in the older adults are the main keys that could help reduce such mortality.
Introduction
In 2025, the World will have about 2 billion older people worldwide, including 80% from developing countries. 1 Despite this significant older adults’ share of the population, HIV infection among them has long been concealed and considered as the young patients’ pathology. According to the Center for Disease Prevention and Control, older adult patients with HIV were aged 50 years or more. 2 Epidemiological data showed an increasing prevalence of HIV infection in older adults, 3 –7 as more and more patients are diagnosed after their 50 years of age, and the availability of highly active antiretroviral therapy (HAART) resulted in an increasing life expectancy among the young patients with HIV. 2,8
In Burkina Faso, almost 1 538 799 people (10.3% of the national population) were aged at least 50 years, in 2011. 9 In 2011, 14 000 patients (16% of patients living with HIV) were older adults, and this percentage is expected to reach 30% by 2040. 10,11
Aging is known to be a source of higher mortality among HIV-infected patients; older adults had 32% excess mortality compared to those aged 25 to 49 years. 12 Therefore, we aim to describe the prognostic factors for early mortality with antiretroviral treatment (ART) in Burkina Faso in older adults to establish a specific approach to treatment and improve the survival of 50 years and older people living with HIV.
Patients and Methods
Design
This was a retrospective and descriptive cohort study comparing HIV-infected older adults to a group of patients diagnosed before their 49 years of age, without matching the characteristics of HIV infection. This study was conducted at the day hospital (outpatient clinic) of the Sanou Souro University Hospital (CHU-SS) of Bobo-Dioulasso, from January 2007 to December 2011. Bobo-Dioulasso is the second largest city of Burkina Faso and located to the west of Burkina Faso. It had a total of 410 459 inhabitants in the last population census in 2006 9 and an overall prevalence of HIV infection at 3.4% in 2008. 13
Study Population
Inclusion criteria
The study participants included adult patients with positive HIV antibody (confirmed in a second sample using HIV enzyme-linked immunosorbent assay test), aged least 15 years at screening, not followed up before, not receiving ART, and treated for the first time in the day hospital of CHU-SS between January 2007 and December 2011.
Exclusion criteria
Those patients who received ART before their first visit to the day hospital were not included in the study.
Data Collection
We collected our data from a computerized database indicated in real time by physicians during medical consultations. After the initial medical examination, each patient was seen, respectively, on the 14th day, the 1st month, the 3rd month, the 6th month, and then every 6 months. At each visit, a clinical examination and laboratory tests were performed including a complete blood cell count, creatinine, fasting glucose, transaminases, and CD4 count. Other tests including viral load were performed on demand. For a given patient, HAART was started according to World Health organization (WHO)—WHO stage 3 or 4, CD4 count <350 cells/mm3, and prevention of mother to child transmission. Cotrimoxazole prophylaxis was provided to those with a CD4 count <350 cells/mm3 or AIDS-related disease in the absence of contraindications (allergy and severe anemia).
Data Analysis
Data were analyzed using Epi info 3.5.1.0 and MedCalc 11.2.0.0 software. MedCalc is statistical software for biomedical research, including ROC curve analysis, method comparison and quality control tools. All the characteristics were described using numbers and percentages for categorical variables and median and interquartile ranges (IQRs 25-75) for continuous variables. Proportions were compared using Pearson chi-square test or exact Fisher test when it was more appropriate. Student t test was used to test the equality of 2 independent sample means, and when the application conditions were not met, nonparametric Mann-Whitney test was used. The level of significance tests was set at P value <5%.
The impact of events of interest (AIDS, high blood pressure, hyperglycemia, elevated serum creatinine concentrations, lost to follow-up, and death) was assessed and compared using the Mantel-Haenszel test. 14 Survival at 6 months with ART was studied using the Kaplan-Meier method. The survival curve of the elderly patients and the young ones was compared using the log-rank test.
Logistic regression (univariate and multivariate) served to identify predictors of death in each group regardless of the time of participation in the cohort. Sociodemographic, clinical, and biological characteristics that were significantly associated with death at the 20% threshold in univariate were included in the multivariate models. Age at seroconversion was estimated by the method of Markov chain.
15
Depending on CD4 count, 91 days after screening, the age at seroconversion is estimated as follows: If CD4 count is <200: age at seroconversion = age at screening − 8 years. If CD4 count is 350-200: age at seroconversion = age at screening − 6 years. If CD4 count is 450-350: age seroconversion = age at screening − 4 years. If CD4 count is >450: age seroconversion = age at screening − 2 years.
Ethical Considerations
Oral informed consent was obtained from all study participants to seek permission to use anonymized routine clinical data in research. Ethical approval for retrospective analysis of these data was obtained from the ethics board of Burkina-Faso and Sanou Souro University Hospital.
Results
General Characteristics of the Study Population
Of the 3367 patients followed up in the service during the study period, 2572 new HIV-infected patients were managed and treated. The median follow-up time with ART was 32.7 months (range, 0.03-65.4 months), IQR (17.4-47.1 months). Overall loss to follow up was 3.3% in older adults and 5.4% in young patients (P = .25).
Prevalence of Older Adults and Cardiovascular Risk Factors
Of the 2572 patients, 265 (10.3%) were older adults. Older patients living with HIV initiating ART were more frequently male (52.5%), illiterate (57.6%), living as couples (59.6%), and leading a business activity (57%; P < .05).
The prevalence of patients with hypertension was significantly higher among older people living with HIV compared with younger ones (39.7% versus 18.6%; P < .001). There were no significant differences between the prevalence of hyperglycemia and hypercholesterolemia among older and young people living with HIV (9.3% versus 7.5%; P = .36). The prevalence of hypertriglyceridemia among older people living with HIV was significantly higher than that of young people living with HIV (36.9% versus 17.5%; P < .001).
Estimating Age at Seroconversion
Within the 3 months following the diagnosis of HIV infection, 2357 (91.6%) of the 2572 patients had reached a CD4 count. According to Markov chain method, the median age at seroconversion for all of these patients was 30 years (range, 8-76 years; IQR, 24-37 years). The median age of seroconversion for older adults (n = 265) was estimated at 47 years (range, 42-76 years; IQR 44-51 years). In the study of older adults living with HIV, 32.1% of them were found to be seroconvert at age 50 or older (n = 85 of 265).
Prognostic Factors for Early Survival with ART
At the end of follow-up, 295 (11.5%) patients died, including 55 older adults (18.6%). Dead patients included 21.1% of older adults and 10.4% of young (P < .01) ones. Univariate analysis included the following 10 features: age at screening, sex, partnership status, illiteracy, occupation, urban residence, HIV serotype, body mass index (BMI) <20 kg/m2 (at diagnosis), WHO stage 3 or 4 (at diagnosis), and lowest CD4 count reached (<200 cells/mm3, at diagnosis). In the following, we showed only the significant associations in univariate analysis.
Early survival factors with ART for all patients
During the first 6 months of following up on ART, 185 (62.7%) of the 295 deaths were reported. Of these, 36 (64.3%) death occurred among older adults and 149 (62.3%) among young people (P = .46). About 79.5% (147 of 185) death occurred in patients seen at WHO stage 3 or 4. In multivariate analysis, BMI <20 kg/m2, WHO stages 3 and 4, lowest CD4 count reached (<200 cells/mm3), and age ≥50 years were in descending order factors associated with early mortality at 6 months on ART. Table 1 and Figure 1 illustrate the factors associated with early mortality at 6 months with ART.
General Early Survival Prognostic Factors on ART.a
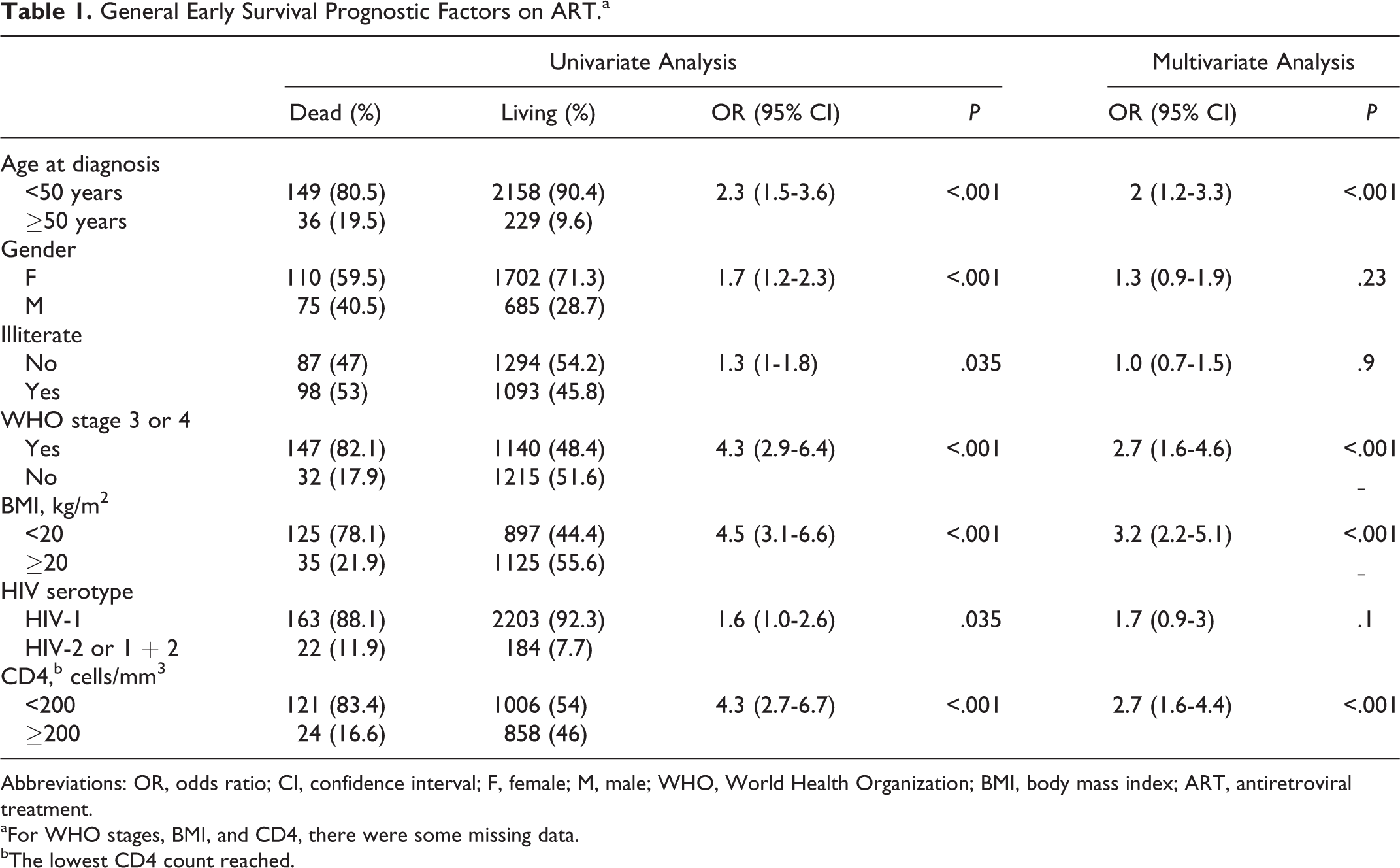
Abbreviations: OR, odds ratio; CI, confidence interval; F, female; M, male; WHO, World Health Organization; BMI, body mass index; ART, antiretroviral treatment.
aFor WHO stages, BMI, and CD4, there were some missing data.
bThe lowest CD4 count reached.

Parigo curve showing factors associated with early mortality on antiretroviral treatment (ART).
Early survival factors on ART among older adults
A total of 36 older adults died, of which 30 (83.3%) occurred initially in WHO stage 3 or 4. In addition, older people living with HIV contributed to 20.4% (30 of 147) of all deaths related to WHO stages 3 and 4. WHO stage 3 or 4 and lowest CD4 count reached (<200 cells/mm3) were the factors associated with early mortality on ART among older adults (Table 2).
Early Survival Prognostic Factors on ART among Elderly Patients.a
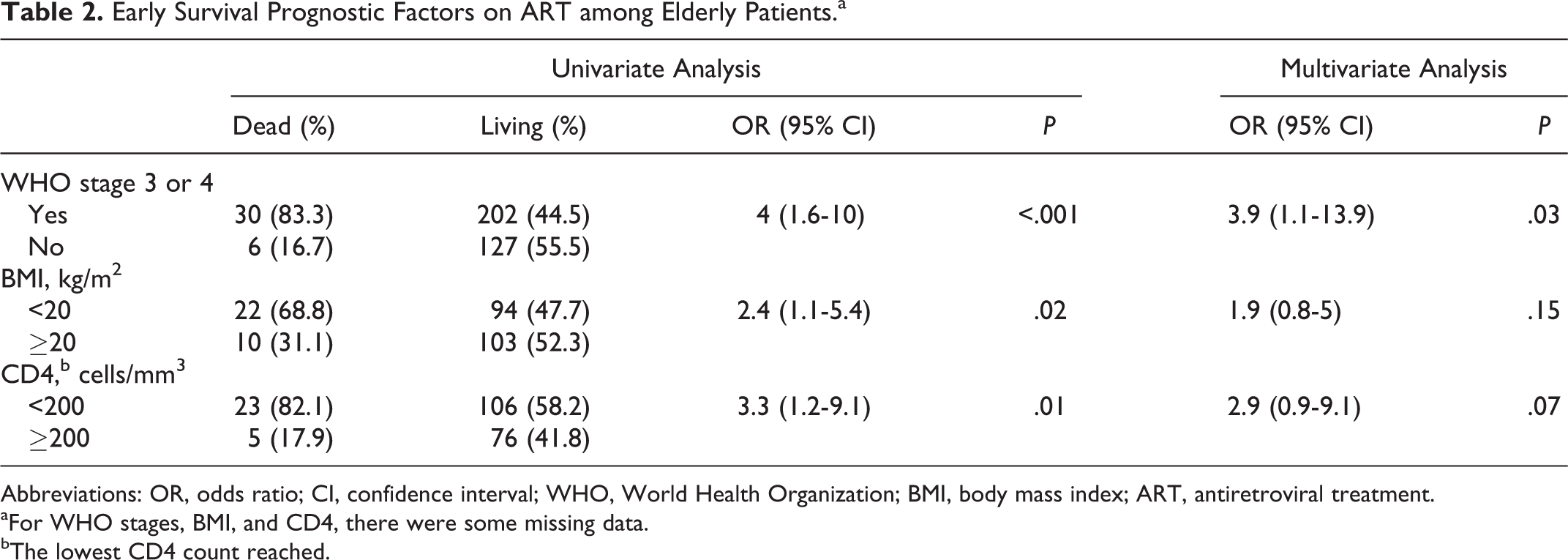
Abbreviations: OR, odds ratio; CI, confidence interval; WHO, World Health Organization; BMI, body mass index; ART, antiretroviral treatment.
aFor WHO stages, BMI, and CD4, there were some missing data.
bThe lowest CD4 count reached.
Early survival factors on ART among young patients
Among young who died due to HIV infection, 117 (77.5%) occurred initially at WHO stage 3 or 4. WHO stage 3 or 4, BMI <20 kg/m2, and lowest CD4 count reached (<200 cells/mm3) were the factors associated with early mortality on ART among young (Table 3).
Early Survival Prognostic Factors on ART among Young Patients.a

Abbreviations: OR, odds ratio; CI, confidence interval; F, female; M, male; WHO, World Health Organization; BMI, body mass index; ART, antiretroviral treatment.
aFor WHO stages, BMI, and CD4, there were some missing data.
bThe lowest CD4 count reached.
Discussion
Our study has some limitations associated with retrospective studies, such as a large proportion of missing data and the number of lost to follow up cases, especially among untreated patients. The median age at seroconversion was 30 years in general and 47 years in the elderly patients. One-third of the elderly patients in our study were more than 50 years at seroconversion. The age at seroconversion is a predictor of mortality. Indeed, Collaborative Group on AIDS Incubation and HIV Survival meta-analysis estimated that among individuals aged 15 to 54 years at seroconversion, the risks of death and acquired immunodeficiency syndrome increased on average by 50% and 33% per decade, respectively. 16 According to other studies, seroconversion in their later years (≥50 years) is in itself a poor prognostic factor of progression to AIDS and death. 17,18 Thus, death rate 5 years after seroconversion for patients infected at the age of 50 is about 125% higher than those infected at age 30 at the same time after seroconversion. 17
Mortality on ART was high during the first 6 months of treatment. Indeed, more than half of the deaths occur during this period. 19 –21 Mortality factors like low BMI, advanced immunosuppression, female gender, and the number of opportunistic infections are usually described in literature. 20 –24 Among the above-mentioned factors, our study also highlighted the role of BMI <20 kg/m2, WHO stage 3 or 4, and lowest CD4 count reached (<200 cells/mm3).
Most of the people living with HIV diagnosed at WHO stage 3 or 4 (82.1%) died within the first 6 months on ART. Death risk associated with these stages was higher among elderly compared with young people living with HIV (3.5 versus 2.5). Age appears increasing as a determinant of early mortality on ART. 12,17,25 –28 Adjusted Weibull analysis I indicated that elderly age status was importantly associated (adjusted hazard ratio 1.23, 95% confidence interval 1.08-1.42) with mortality, when controlling for sex, baseline CD4 count, and year of therapy initiation. 27 In Spain, for example, mortality among newly managed people living with HIV after 50 years would be 3 times higher than that of young people living with HIV, despite ART. 29
Several factors may explain the high mortality among older people living with HIV. Epidemiologically, the elderly patients are not considered by the medical profession nor considered by themselves as being at risk of HIV infection, so that the diagnosis is made too late. 17,30 In addition, at the pathophysiological level, the production of interleukin 7 decreases with age. 31,32 This cytokine is involved in the proliferation of thymus cells, differentiation and maturation of B and T lymphocytes, and restoration of peripheral T lymphocytes in the people living with HIV. 33 Moreover, with aging, thymic involution causes a decrease in the production of T-naive cells, and this thymic alteration makes immune restoration during HAART. 34 –36
Thus, the elderly patients often have a low CD4 count at diagnosis, 37,38 a high viral load, and are often symptomatic. 39 –41 In addition, weight loss, tiredness, and visual and cognitive disorders are often wrongly perceived as associated with normal aging, 42 while being signs of potentially lethal comorbidities.
Finally, in our study, the prevalence of cardiovascular risk factors was higher in elderly patients compared with young patients. In general, the prevalence of cardiovascular risk factors is higher in HIV-infected patients than in the general older population, explaining the high incidence of cardiovascular diseases and especially cancer, providing a high mortality in this population. 43
Early diagnosis in adults from 40 years and primary prevention especially among the elderly patients should significantly reduce the prevalence of HIV infection in this group and therefore associated mortality. Early ART initiation and improving clinical care of older adults are required to reduce high early mortality and enhance immunologic recovery, particularly in the initial phases of ART. 12
In our study, the older people living with HIV receiving ART, from the initial prognostic factors, only WHO stages 3 and 4 and lowest CD4 count reached (<200 cells/mm3) were associated in multivariate analysis with death at 6 months (OR = 3.9, 1.1-13.9; P = .03). According to our results, a study in Spain with the same initial prognosis factors, only AIDS stage was associated with mortality in older people living with HIV on ART, with 3 times higher risk of death. 29
In older people living with HIV, preventing the onset of WHO stage 3 or 4 through the early detection of HIV infection and early initiation of ART could be an effective way for a short-term better survival of these patients.
Conclusion
Aging is recognized as a major cause of mortality in several pathologies, and HIV infection is not an exception to this phenomenon. Mortality rate among older people living with HIV in Burkina Faso is high. Aging and advanced immunosuppression are prognostic factors of mortality during the first 6 months on ART in this population. Early diagnosis, early treatment, and primary prevention of HIV infection in the elderly patients are the main keys that could help reduce such mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.