
Abstract
This study investigates the differences in severity and correlates of depression symptoms among 1069 men and 267 women living with HIV in Ontario, Canada, who completed the 20-item Center for Epidemiologic Studies Depression Scale (CES-D). Women had higher CES-D scores than that of men (median [interquartile range]: 13 [5-26] versus 9 [3-20], P = .0004). More women had total CES-D scores >15 (mild-moderate depression; 44% versus 33%, P = .002) and >21 (severe depression; 31% versus 23%, P = .003). Unlike men, at age 40, women’s scores increased yearly (0.4 per increased year, P = .005). The distribution of scores differed by gender: There was no difference in the 10th percentile of depression scores, 0 (95% confidence interval [CI]: 1.0-1.0) but the 75th percentile of depression scores for women was 6 (95% CI: 2.0-10.0) points higher than that of men. Important gender differences exist in depression symptoms and in correlates of symptoms in people living with HIV.
Introduction
Clinicians have long hypothesized that certain psychological characteristics are associated with increased vulnerability to physical illness and worsening disease outcomes. 1 More recently, studies have identified a similar relationship, observing an association with depression and adverse health outcomes in individuals with and without chronic disease. 2 –4 Today, with the transformation of HIV from a subacute and fatal infection to a chronic treatable disease, 5 the psychological outcomes experienced in people living with HIV remain an important health concern for clinicians and researchers.
Depression may be the most salient of these concerns. Classified by the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition), major depressive disorder is one of the most common psychiatric diagnoses seen in people living with HIV, 6 with a prevalence ranging from 16.2% 7 to 36%. 8 Although estimates vary among published studies, previous research suggests that depression in people living with HIV is 4 to 7 times greater than that in the general population. 9 –11
Of equal importance is the impact of depression on the clinical course of HIV. Studies have shown an association between depression and faster disease progression in men 12 –14 and between depression and mortality in women. 15 In addition, some studies have shown that depression alters immune function in people living with HIV, 16 –18 independent of adherence behaviors. 19 Others, however, have found no association between depression and immune function in this population. 20,21
Although the mechanism in which depression worsens HIV disease progression is poorly defined, treatment is imperative. Double-blind placebo-controlled trials and open-label studies show that depression is treatable in the context of HIV. 22 –25 Yet depression continues to be underdiagnosed and consequently undertreated. 26 In a mixed sample of men and women living with HIV, Asch et al 26 found that fewer than half of patients with depression were recognized as depressed by their health care providers. One barrier to managing depression in patients living with HIV is inadequate screening by health care providers. 27 Few clinicians routinely ask their patients whether they are depressed, and few patients volunteer the information spontaneously. 27
Diagnosis and treatment of depression in people living with HIV is further complicated by the overlap of somatic symptoms present in both HIV and depression. 28 Clinicians are therefore left with the difficult task of determining whether the clinical presentation of lethargy, unintentional weight loss, and poor appetite are a result of depression or an underlying primary infectious process on its own. 29 In addition, depression symptoms including agitation, depressed mood, and insomnia are linked to medications commonly used in patients living with HIV. 30,31 Appropriately diagnosing depression is therefore not easy and, as recognized by the US Preventive Services Task Force Agency for Healthcare Research and Quality, requires careful consideration of a patient’s history and physical examination when suspected. 32 Understanding the unique correlates of depression in people living with HIV is therefore important for clinical care.
Demographic and clinical variables have been found to be associated with high depression symptoms in people living with HIV. Demographically, age, 33 less education, and low socioeconomic status 34 were associated with high depression symptoms. In studies with mixed-gender samples, clinical variables associated with high depression symptoms have included high HIV plasma viral load, duration of HIV infection, CD4 counts <500 cells/mm, 3 and coinfection with other serious medical illnesses including hepatitis C. 35,36 It is unclear whether the findings from these studies can be generalized to the female samples of people living with HIV since predictors of depression were examined exclusively among men or, from mixed-gender samples, with a limited discussion of gender-specific factors.
In studies examining gender-specific correlates, female gender has been identified as an important predictor to screening positive for depression. 37 In addition, associations between HIV-related stigma 38 and general psychological distress have been identified as important predictors to depression in women living with HIV. 39 Nevertheless, despite the known burden of depression among men and women living with HIV, few studies have compared gender differences in severity and correlates of symptoms.
One exception was the CRANium study, a 15-site cross-sectional study exploring differences in the prevalence of depression in male and female populations. Researchers in this study found that a higher proportion of women living with HIV than men living with HIV met the criteria for depression (17.9% versus 14.3%, P = .01). 40 Gender differences in severity of depression symptoms have also been explored, showing women living with HIV reporting more depression symptoms than that of HIV-positive men. 41,42
Our study expands previous research on gender differences in depression and HIV by assessing not only differences in prevalence and severity of depression between men and women but also nuances in severity. In addition, the study examines the potential differences in correlates of depressive symptoms between men and women living with HIV in Ontario, Canada.
Methods
Study Population and Design
The study was a cross-sectional analysis of the Ontario HIV Treatment Network Cohort Study (OCS). 43 The OCS is a multisite, clinical and population health prospective observational research study that recruited participants through primary and tertiary care sites. Data were collected from multiple sources including electronic medical records, chart abstraction, and linkages to other laboratory databases. 43 The OCS introduced an annual interviewer-administered questionnaire in October 2007, using a 20-minute core questionnaire or a 90-minute extended questionnaire that provides more extensive demographic and sociobehavioral information, including the Center for Epidemiologic Studies Depression Scale (CES-D). 43
Inclusion criteria for this analysis were that participants must (1) be HIV positive based on a positive HIV antibody test or other laboratory evidence of HIV infection; (2) have provided OCS data on gender; and (3) have completed >50% of the CES-D.
Measuring Depression
We used the CES-D, which consists of 20 items assessing the frequency of depressive symptoms over the past week. 44 Each item includes 4 response categories ranging from rarely or none of the time (less than 1 day) to most or all of the time (5-7 days) (0-3). 44 The scale reflects 6 major dimensions: (1) depressed mood; (2) feelings of guilt and worthlessness; (3) feelings of helplessness and hopelessness; (4) psychomotor retardation; (5) loss of appetite; and (6) sleep disturbance. 44 Item scores are added together after reverse coding 4 items to generate a summary score ranging from 0 to 60. 44 For the participants missing some CES-D questions, the total CES-D score was imputed by dividing the sum of all available scores by the total number of questions answered and multiplying this sum by 20. 45,46 Scores >15 were categorized as mild-moderate depressive symptoms, while scores >21 were categorized as severe depressive symptoms. We derived these cut points from those used in previous studies. 47 –50
The CES-D is not a tool for diagnosing clinical depression but can be used as a screening instrument to assess the frequency of depressive symptoms and severity in population-based research. 44 The CES-D has been used in community-based and clinical samples of individuals with various health conditions including physical or psychiatric illness and disability, including adults living with HIV. 44 This widely used instrument has been shown to have high internal consistency, test–retest reliability, and concurrent and construct validity and has been used with HIV populations. 51,52
Definition of Correlates
The primary correlate of interest was gender. Gender was defined through social, economic, political, and cultural forces and not by the distinction between biological, physical, and genetic differences. 53,54 Participants were included if they self-identified as a man or a woman. Due to a small number of participants (n = 8), those self-identifying as transgendered or intersexed were excluded from the analysis.
Survey instrument
Correlates previously defined as relevant to HIV and depression were examined. The interviewer-administered questionnaire included correlates of interest as outlined.
Demographic characteristics
Participants provided demographic information about their gender, age, race/ethnicity, birthplace, educational level, income, place of residence, employment status, and current injecting drug use.
Health variables
Information of the participants was gathered from the medical charts, indicating the year of HIV diagnosis, mode of HIV transmission (if known), and presence of coinfection with hepatitis C or hepatitis B. As well, participants’ CD4 counts and HIV viral load were recorded. Details of HIV antiretroviral therapy (ART) were also recorded, including lists of the medication names, dose, and duration of therapy.
HIV-related stigma
Stigma outcomes were measured using a revised version of the HIV Stigma Scale developed by Berger and colleagues. 55 Our study used the same revised version that was used in Loutfy MR et al study that was referenced. The Berger HIV Stigma Scale is a reliable and valid measure and has been used with a similar population of HIV-positive women. 56 The 16-item stigma questionnaire has 4 subscales: “Personalized Stigma” (enacted stigma), “Disclosure Concerns” (enacted stigma), “Negative Self-Image” (internalized stigma), and “Concern with Public Attitudes” (perceived stigma). 57 Each subscale contained 4 items on a 5-point Likert scale. Total stigma scores were calculated by summing the scores for the 4 subscales. Total HIV Stigma score ranges from 16 to 80, with higher scores indicating a higher degree of HIV-related stigma. 57
Life stressors
Life stressors were measured using the National Population Health Survey Stress Questionnaire. 58 This tool is routinely administered to the general Canadian population by Statistics Canada 59 and has been used in previous studies examining HIV populations with good internal consistency. 60 The questionnaire examines recent life stressors, chronic or ongoing problems, and early childhood adversities 58 through a total of 34 questions. The total number of stressors was computed by summing up responses of the 34 questions, with higher number of responses indicating greater number of stressors. 58
Recent life events include “acute changes that are detrimental to well-being and require a significant degree of adjustment within a short period of time.” 61 These were measured by asking 10 questions about the occurrence of negative events in the past 12 months, including physical attack, financial crisis, or job loss. Chronic or ongoing stressors refer to “life stressors that develop gradually over time and can be related to social roles or circumstances.” 61 Stressors such as activity overload, financial difficulties, relationship, or marital problems were assessed using 17 statements including “[I] am trying to take on too many things at once,” “There is too much pressure on [me] to be like other people,” and “Too much is expected of [me] by others.” Finally, childhood adversity measures the number of traumatic events that participants have been exposed to during their childhood or adolescence. 61 Participants were asked 7 questions about parental divorce, prolonged parental unemployment, frequent parental alcohol or drug use, a lengthy hospital stay (2 weeks or more), and physical abuse.
Statistical Analysis
Demographic, clinical, and social characteristics were summarized by gender using median and interquartile ranges (IQR) for continuous variables and using frequencies and proportions for categorical variables. Characteristics were compared between men and women using chi-square tests or Fisher exact tests for categorical variables and Wilcoxon rank sum tests for continuous variables.
Quantile regression models were used to examine the association between gender and the distribution of total depression scores, after adjusting for other covariates such as age, high HIV viral load, duration of HIV infection, HIV-related stigma, and education. In particular, we were interested in the effect of gender on the upper end of the CES-D distribution, as participants with these scores are most at risk for depression. The effects of gender on the 50th, 60th, and 75th percentiles were reported. Multivariable models were constructed for women and men separately as well as for women and men together. An interaction term between age and gender was included in the model since age had a different effect on depression in men than in women. Piecewise linear terms were used to model the effects of age and stigma score on depression.
Results
Study Population
Of the 1331 self-identified men and women who completed the extended questionnaire, 1327 met the inclusion criteria (267 women and 1060 men). Four participants did not meet the inclusion criteria, as 1 participant did not answer any of CES-D questions and the remaining 3 filled out less than 50% of the CES-D questions. In total, 1275 (96%) completely filled out all CES-D questions. Of the 52 participants who had less than complete data, 44 had only 1 or 2 missing items. The remaining 8 participants had at least 50% of the questions completed. The total CES-D score was imputed for people missing some CES-D questions as described earlier.
Demographic Characteristics of Study Population
Table 1 displays the demographic and clinical characteristics of the study population. Men in our study were older (47 versus 41 years old), more likely to be white (66 versus 29), and less likely to be black (10 versus 59). More men in our study were born in Canada (63% versus 29%) and gay/bisexual (81% versus 5%). Men also had a longer duration of HIV infection (12 years versus 8 years), longer duration of ART (9 versus 5 years), and were more likely to be on ART (88% versus 81%), including receiving treatment with efavirenz (EFV; 28% versus 20%).
Baseline Demographic, Clinical, and Social Characteristics by Gender.a

Abbreviations: CES-D, Center for Epidemiologic Studies Depression Scale; MSM, men who have sex with men; IDU, injecting drug use; ARV, antiretroviral; OCS, Ontario HIV Treatment Network Cohort Study. FT/PT, full-/part time; VL, viral load.
a Data are summarized as median and interquartile range or frequency and percentage.
b In addition to the options of white and black, the OCS questionnaire gives the following choices for race/ethnicity: Aboriginal, Latin America, Asia (China, Japan, and Korea), Southeast Asian (India, Pakistan, and Sri Lanka), Persia (Egypt, Iran, and Armenia), and other. Of the 186 participants classified as “Other” race, 56 identified as Latin American, 41 as Asian, 33 as Southeast Asian, 12 as Persian, and 44 as other. We report that 76 participants were of aboriginal descent and have grouped in the other categories.
c For participants who were never on ARV medications, years of ARV medication were set at 0.
More women in our study were from countries where HIV is endemic (59% versus 10%). As well, more women in our study were from families of household gross yearly income of Can$40K per year (67% versus 47%). Compared to 22.8% of men in the OCS sample, 66.3% of women report having children (P < .001).
Depression Scores
Compared to men, women were significantly more likely to have a higher median total CES-D scores (13 [IQR 5-26] versus 9 [IQR 3-20]), P = .0004). Also, women were significantly more likely than men to have total CES-D scores >15 (44% versus 33%, P = .002) and >21 (31% versus 23%, P = .003). In addition, total CES-D scores varied by gender. The 90th percentile and maximum CES-D scores were 32 and 57, respectively, for men and 37 and 57, respectively, for women.
Univariate Analyses for Factors Associated with High Depression Scores
In the univariate quantile regression analyses, having less education, overall stigma scores ≥50, living with a disability, having a household income <Can$40K per year, and life stressors such as recent life events, ongoing problems, and early childhood adversities were all associated with higher median CES-D scores in both men and women (Table 2). Men and women who were infected through injecting drug use and were unemployed also had higher median CES-D scores, with statistically significant associations noted among men. Among women, having children was not significantly associated with CES-D scores. Housing was also considered in the univariate analysis reported in Table 2 and was not a significant predictor of CES-D score.
Estimated Effects of Covariates on Median Total CES-D Scores from Univariate Quantile Regression Models among the Total Study Sample and by Gender.

Abbreviations: CES-D, Center for Epidemiologic Studies Depression Scale; CI, confidence interval; IDU, injecting drug use; ARV, antiretroviral; FT/PT, full time/part time.
a This is a piecewise linear term. Age assumes different slopes between ages <40 and ≥40.
b This is a piecewise linear term. Stigma score assumes different slopes between scores <50 and ≥50.
Univariate Analyses for Factors Associated with Lower Depression Scores
In both men and women, more years of ART was significantly associated with lower CES-D scores. However, in the split sample of men and women, neither duration nor current use of ART was a significant predictor of CES-D score. Among men, increasing age (older than 40 years) was associated with a decline in the total CES-D scores. In addition, in men whose ART included EFV, lower overall CES-D scores was observed.
Multivariable Analysis for Factors Associated with High Depression Scores
Table 3 displays the effects of covariates on the median CES-D in multivariate models for men, women, and men and women together. Compared to employed participants, disabled and unemployed participants had higher CES-D scores among both men and women. A piecewise linear term was used to examine the association of stigma with depression. Although increments in stigma scores <50 were not associated with increases in depression, increments in stigma scores ≥50 were significantly associated with higher median CES-D scores in women and men. Among women in our study, increases in age (older than 40 years) were associated with higher total depression scores (0.4 per increased year, P = .005) after adjusting for other correlates in the multivariate analysis (Figure 1).
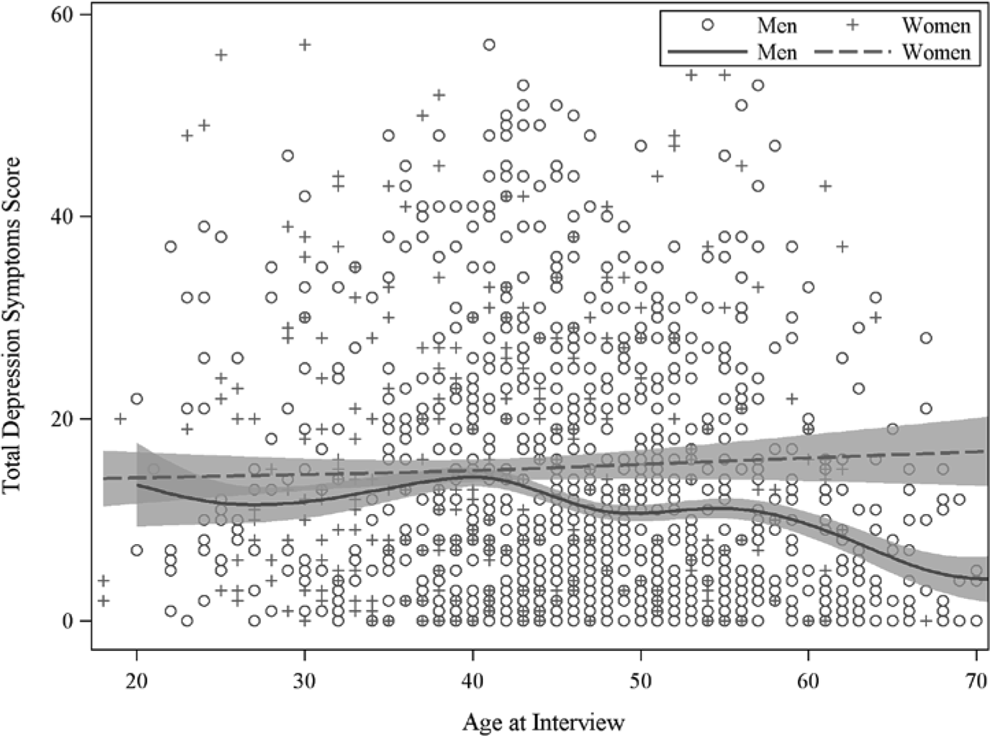
Association of Total CES-D Score with Age at Interview by Gender. The smoothed lines and 95% confidence limits were obtained from the multivariable quantile regression.
Estimated Effects of Covariates on Median Total CES-D Scores from Multivariable Quantile Regression Models among the Total Study Sample and by Gender.

Abbreviations: CES-D, Center for Epidemiologic Studies Depression Scale; IDU, injection drug use; ARV, antiretroviral; FT/PT, full time/part time; CI, confidence interval.
a This is a piecewise linear term. Age assumes different slopes between ages <40 and ≥40.
b This is a piecewise linear term. Stigma score assumes different slopes between scores <50 and ≥50.
Table 4 displays the effects of covariates on the 50th, 65th, and 75th quantiles of depression in a multivariate analysis of men and women. The interaction between age and gender, EFV use, disability, unemployment, stigma, recent life events, early childhood adversities, and ongoing problems was associated with all 3 quantiles of depression scores. Figure 2 displays the effect of several covariates on the entire distribution of CES-D, as estimated from the multivariable quantile regression model. It can be seen that covariates such as disability have a greater effect on the upper tails of the distribution than on the lower tails of the distribution.

Estimated Effects of Covariates on the distribution of Total CES-D Score from the Multivariable Quantile Regression Model. The solid line reflects the estimated effect of a covariate across the distribution of total CES-D score, i.e., the effect on the different quantiles. The shaded area represents the 95% confidence interval of the estimated coefficient. An increasing trend indicates a larger effect on the higher end of the distribution—higher quantile, higher depression score, and vice versa. A significant effect on a specific quantile is demonstrated by its confidence interval (shaded area) not containing the y = 0 line.
Estimated Effects of Covariates on 50th, 65th, and 75th Quantiles of Total CES-D Scores from Multivariable Quantile Regression Models.

Abbreviations: CES-D, Center for Epidemiologic Studies Depression Scale; CI, confidence interval; IDU, injecting drug use; ARV, antiretroviral; FT/PT, full time/part time.
a This is a piecewise linear term. Age assumes different slopes between ages <40 and ≥40.
b This is a piecewise linear term. Stigma score assumes different slopes between scores <50 and ≥50.
Discussion
Based on CES-D scores, more than a third of our sample of women living with HIV reported high depressive symptoms in comparison to men. This high rate of depressive symptoms in women living with HIV is consistent with earlier studies, where a higher prevalence 39 and severity of depressive symptoms 62 –65 have been shown in women as compared to men living with HIV. Our study extends these findings by showing gender differences also in the distribution of total CES-D scores. Using multivariable analysis, our study showed that women experienced more severe depressive symptoms and, further, that differences between men's and women's total CES-D scores increased for those with higher scores. These findings have important treatment implications in the context of recent literature that conceptualizes depression and treatment along a spectrum of increasing severity of symptoms, varying from nonspecific depressive symptoms, minor depression, to major depression. 66 –68 For women living with HIV, this may broaden indications for treatments based on symptoms. More research is therefore needed to address the clinical significance and treatment implications for the presence of higher depressive symptoms in a particular patient population.
Our study also showed that age ≥40 might impact the symptoms of depression differently in women than in men living with HIV. Once adjusting for other correlates, women ≥40 years of age showed increased median depression scores while men ≥40 years of age showed decreased CES-D scores in both models. These findings have significant implications for depression screening and treatment plans in people living with HIV. Clinicians and health care providers should be aware that women living with HIV who are aged ≥40 might be at higher risk for greater depression severity.
Men currently on ART showed lower overall depression scores. In a previous mixed-gender study, structured clinical interviews were conducted in a study of 152 men and women living with HIV assessing depression, anxiety, and substance use disorders. 69 In this study, the use of ART was associated with lower prevalence of any psychiatric disorder including depression. In our study, CES-D scores for women showed no overall change with the use of ART. Notably, however, since the number of women included in our study is significantly fewer than the sampled men, this finding may be a power issue. Further research is therefore needed to better understand these differences.
Another important finding in our study is in showing that certain correlates of depression predict high levels of depression in both men and women living with HIV. Having less education, living with a disability, having low family income, having high overall stigma scores, and having a higher number of stressors were significantly associated with higher depression scores in both male and female participants. In addition, higher stigma scores were correlated with a higher total CES-D score in both men and women. In previous studies, stigma has been shown to correlate with depression in people living with HIV. 67 Our study extends these findings by showing that stigma is correlated with depression symptoms in both men and women living with HIV. Thus, interventions for victims of HIV-related stigma including stress management interventions 70 should be aimed at both men and women living with HIV.
Our study examined the effects of covariates on the 50th, 65th, and 75th quantiles of depression in men and women. Increases in depression per year of age are seen in women in the upper quantiles. In addition, disability, unemployment, and ongoing problems also have larger effects on the 65th and 75th quantiles than on the 50th quantile in both men and women. It has been previously demonstrated that age, 33 disability 71 , unemployment 71 and ongoing problems 71 are important correlates to depression in men and women living with HIV. However, the effects of these covariates on patients with high depressive symptoms have not been examined. Future studies should examine these covariates as important factors that may worsen depressive symptoms in individuals who at the onset have high depressive symptoms.
Limitations to Our Study
Less clear is the association between mental health and suboptimal HIV treatment. Women in our study were less likely than men to be on ART, despite more women in our study having CD4 counts <200 cells/mm3. Shortcomings in HIV treatment experienced by women living with HIV have been associated with several variables including low socioeconomic class. 72 Further research is needed to better understand the relationship between suboptimal treatment and depression.
Since the OCS is a voluntary study of HIV-positive individuals engaged in care, there is potential for selection bias as the participants in the OCS may differ from the general population of men and women living with HIV in Ontario. Also, the high proportion of men who have sex with men in the male subsample (80%) limits the study. Although this is somewhat representative of HIV care in major city centers in Ontario, there are limitations in comparing a largely gay male subsample with a largely heterosexual female subsample. Future studies with a larger proportion of heterosexual men should conduct similar analyses to see whether the differences found in the present study are also found when comparing heterosexual men to heterosexual women, as gay men report higher rates of major depression than their heterosexual counterparts. 72,73
Additionally, it is possible that participants in the OCS experience lower levels of depression than those who did not participate. The study was also not able to capture the experiences of transgender people living with HIV due to the small number enrolled within the OCS. The significance of depression and gender among diverse racial populations was also not explored.
Conclusion
Recognizing the unique correlates of depression in people living with HIV is imperative to develop adequate screening protocols that are targeted to diagnose and treat people living with HIV at risk for depression. The present study found that severe depressive symptoms were more prevalent in women than men living with HIV. Age ≥40 was associated with more severe depression symptoms in women. Among men and women, having less education, overall stigma scores ≥50, living with a disability, having a household income <Can$40K per year, and life stressors were associated with higher median CES-D scores. Our findings may assist clinicians in screening for depression in high-risk women and men living with HIV. These include women of age >40 as well as men who are less educated or with disability. Also, understanding the differences in correlates of depression between men and women may assist clinicians in accurately diagnosing it. In addition, it further suggests a need for depression screening measures that recognize gender differences in the risk factors for depression.
Footnotes
Acknowledgments
We gratefully acknowledge all of the people living with HIV who volunteered to participate in the OHTN Cohort Study and the work and support of the past and present members of the OCS Governance Committee: Adrian Betts, Anita C. Benoit, Les Bowman, Tracey Conway, Patrick Cupido (Chair), Tony Di Pede, Brian Finch, Michael J. Hamilton, Brian Huskins, Rick Kennedy, Ken King, Nathan Lachowsky, Joanne Lindsay, Shari Margolese, John McTavish, Colleen Price, Lori Stoltz, Darien Taylor, Rosie Thein, and Drs. Ahmed Bayoumi, Evan Collins, Curtis Cooper, Clemon George, Troy Grennan, Claire Kendall, and Greg Robinson. We also acknowledge the Public Health Laboratories, Public Health Ontario, for supporting record linkage with the HIV viral load database. The opinions, results, and conclusions are those of the authors and no endorsement by the Ontario HIV Treatment Network or Public Health Ontario is intended or should be inferred.
Authors’ Note
The OHTN Cohort Study team consists of Dr Sean B. Rourke (Principal Investigator, University of Toronto and OHTN), Dr Ann N. Burchell (Co-Principal Investigator, OHTN), Dr Sandra Gardner (OHTN), Dr Sergio Rueda (OHTN), Dr Ahmed Bayoumi and Dr Kevin Gough, St. Michael’s Hospital; Dr Jeffrey Cohen, Windsor Regional Hospital; Dr Curtis Cooper, Ottawa General Hospital; Dr Don Kilby, University of Ottawa Health Services; Dr Mona Loutfy and Dr Fred Crouzat, Maple Leaf Medical Clinic; Dr Anita Rachlis and Dr Nicole Mittmann, Sunnybrook Health Sciences Centre; Dr Janet Raboud and Dr Irving Salit, Toronto General Hospital; Dr Edward Ralph, St. Joseph’s Health Care; Dr Roger Sandre, Sudbury Regional Hospital; McMaster University Medical Centre; and Dr Wendy Wobeser, Hotel Dieu Hospital. We thank all the interviewers, data collectors, research associates and coordinators, nurses, and physicians who provide support for data collection and extraction. The authors wish to thank the OHTN staff and their teams for data management and IT support (Mark Fisher, Director, IT), and study coordinators (Kevin Challacombe, OCS Data & Brooke Ellis, OCS Research). Two investigators (TAH and JMR) are funded by an OHTN Career Scientist Award.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The OHTN Cohort Study is supported by the Ontario Ministry of Health and Long-Term Care.