
Abstract
Objective:
The incidence of Kaposi's sarcoma (KS) decreased dramatically after the introduction of highly active antiretroviral therapy (HAART). This study determined the ongoing incidence of and mortality from KS in HIV-infected adults from 1998–2012 in Fresno County, California. The role of virologic control and immune reconstitution was assessed.
Methods:
Incident cases were identified from the state Electronic HIV/AIDS Reporting System (EHARS), the California Cancer Registry, and hospital records of the county HIV treatment center.
Results:
From 1998–2012, the average incidence of KS was 0.51 cases per 100,000 person-years. Of the 66 cases of KS there were 20 deaths, with 85% of the mortality occurring in the first 12 months. Among patients on HAART achieving HIV RNA <400 copies/uL, but with a <50 cell/uL increase in CD4 count there was no improvement in mortality.
Conclusions:
The incidence of KS remains stable since 1998 with a 12-month mortality of 30%.
Introduction
The incidence of Kaposi's sarcoma (KS) in people living with HIV/AIDS decreased dramatically after the advent of highly active antiretroviral therapy (HAART) in 1996. 1 The incidence of KS has also continued to decrease in the HAART era. 2,3 However, KS remains the most common AIDS-defining malignancy in HIV-positive patients during the first 6 months of HAART, and the incidence persists at a lower level from 6 months to 10 years of HAART. 4 The prognosis of KS has improved greatly in the HAART era, both in resource-rich and in resource-limited settings. 5,6 However, despite the improved prognosis with the availability of HAART and chemotherapy for KS, significant mortality from KS continues. 7 In Fresno County (population 948 000), California, a persistence of presentations of severe KS with poor outcomes was anecdotally observed. This study was carried out to determine whether there were changes in the incidence of and mortality from KS in Fresno county, California, since the introduction of HAART.
Methods
Incident cases of KS in Fresno County were identified from 3 sources: the state Electronic HIV/AIDS Reporting System (EHARS), the California Cancer Registry, and from the hospital records of the Fresno County HIV clinic. KS is a reportable disease in California, and all newly diagnosed cases are supposed to be reported for inclusion in both the state EHARS database and the Cancer Registry. All cases with KS diagnosed from January 1998 through December 2012 were included. Clinical data for patients were available from the hospital medical record, and demographic, laboratory, and outcome data were available from the EHARS; data were collected through January 2013. Patients not reported as dead to the statewide EHARS were assumed to be alive at the end of the study period.
Incidence rates per 100 000 population were computed, and the percentage dying within 12 months was calculated. Differences in survival were computed using the Kaplan-Meier method, and statistical significance of the different survival curves was assessed with the log-rank method. Statistical analysis was carried out using SPSS IBM version 21. This study was approved by the Community Regional Medical Center Institutional Review Board (protocol #200317).
Results
Review of KS diagnoses from 3 independent data sources found little overlap between the EHARS and cancer registry databases, despite KS being a reportable disease to both of these entities. Of the 66 cases we identified, only 4 were present in both the state EHARS database and the hospital-based cancer registry.
In 2013, Fresno County had a population of 947 895 and 1628 reported persons living with HIV/AIDS. From 1998 to 2012, there were 66 reported cases of KS, showing an incidence of 0.51 cases per 100 000 person-years (±0.04, 95% confidence interval), with no trend toward a decrease over time (Figure 1). All the patients with KS were males. The median CD4 count at the time of KS diagnosis was 50 cells/mm3. Of the 66 cases of KS, there were 20 deaths (30% mortality) during the period of the study, with the large majority (85%) of deaths occurring in the first 12 months post KS diagnosis (Figure 2).
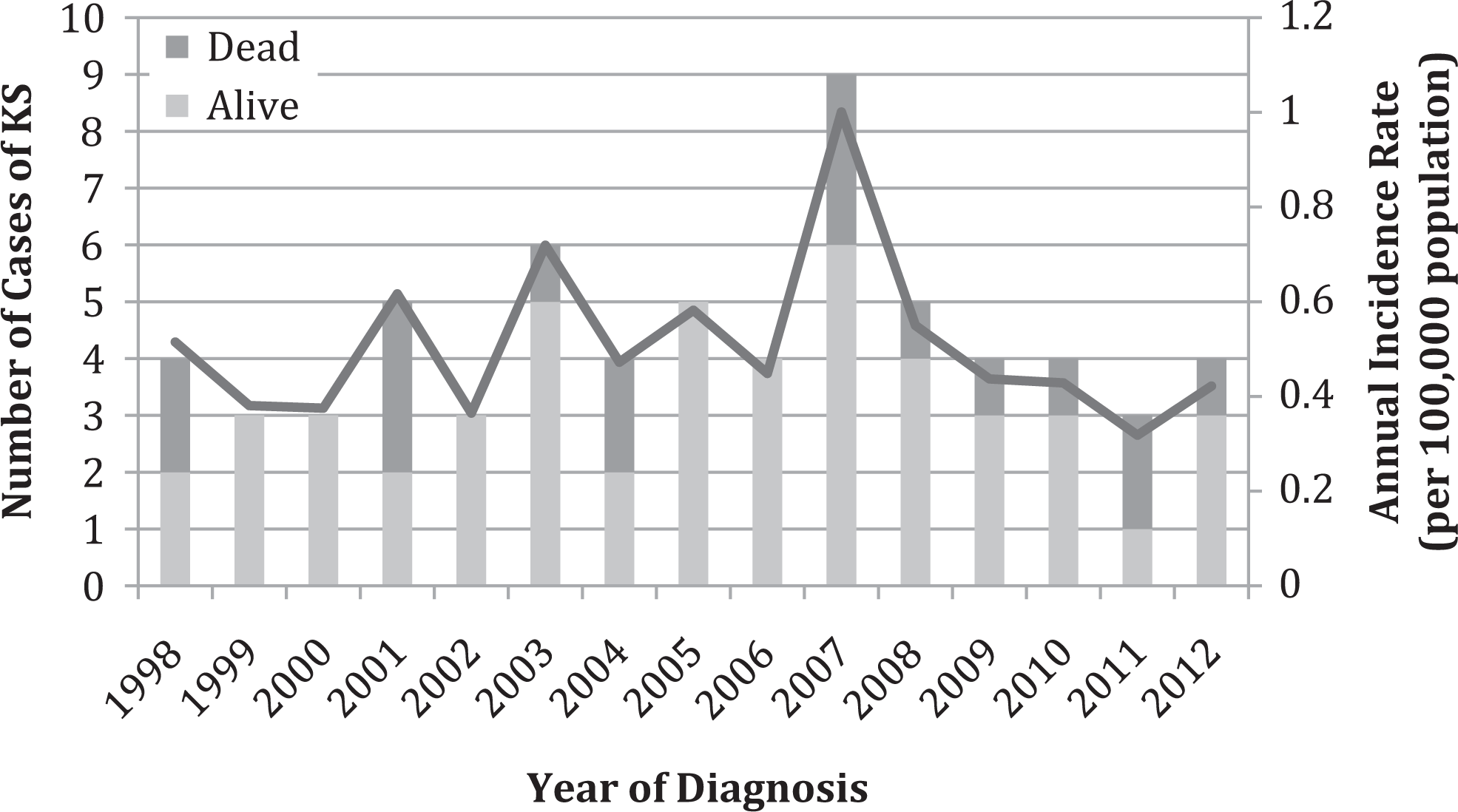
Incidence of Kaposi sarcoma (KS) and the 12-month mortality, Fresno County, 1998-2012.

Survival of patients with Kaposi sarcoma (KS) based on HIV viral load (VL) and change in CD4 count. *P < .05 compared with HIV VL <400 ΔCD4> 50 by log-rank test.
Of the 66 patients diagnosed with KS, 41 achieved an HIV viral load (VL) of <400 copies/mL. For this group on successful HAART, the mortality was significantly lower, but still significant with 7 (17%) of 41 patients dying (Figure 2). Two of these patients on successful HAART died of cardiac arrest after their KS was in remission. However, the other 5 deaths of patients on successful HAART were due to complications of KS. These five patients had a median decrease of 34 cells/mm3 in CD4 count, in contrast to a median increase of 281 CD4 cells/mm3 in those on HAART that survived.
Discussion
An initial surprising finding of this study was the lack of overlap between the California state EHARS and California Cancer Registry databases to which KS diagnoses are reportable. As KS reporting is mandated for both databases, there should have been a complete overlap of cases in the 2 databases. However, only 4 of 66 cases had been reported to both databases (presumably due to physician noncompliance with paper-based reporting requirements). Data collection from three separate databases greatly strengthened completeness for the present study. The incompleteness of relying on a single database is worth bearing in mind for future studies.
One limitation to our study was the lack of clinical data for patients cared for outside our institution. However, our institution is the largest HIV service provider in Fresno County, caring for more than 900 HIV-infected patients. In Fresno County, there are a reported 1628 persons with HIV infection, however, many of these are not in care and then enter our clinical program only if ill. Thus, it was not surprising that of the 66 patients with KS, 43 were at our medical center, and hence, detailed clinical data were available. The death of patients with AIDS-associated KS, however, is often multifactorial due to other opportunistic infections and comorbidities, rather than related to progressive KS alone. 8 For this reason, we used all-cause mortality as our end point.
Although lack of clinical data for some patients affected our ability to assess treatment course and precise cause of death, our assessment of mortality was accurate based on the state EHARS database, which is notified of all deaths of HIV-infected persons throughout the state of California. Thus, even if patients were lost to follow-up in Fresno County during the study period, if the patient remained within California, our mortality data remain correct. Thus even if patients were lost to follow-up in Fresno county during the study period, if they remained within California, our mortality data remain correct. If patients moved out of state and their death was not reported to California, the mortality rates in this report would be underestimated.
The persistence of KS in our area likely represents continued late diagnosis of HIV infection after the occurrence of significant immunosuppression. It would be of interest to compare the incidence of other opportunistic infections over the same time period to see whether other markers of late diagnosis of HIV infection show a similarly stable incidence as seen here for KS. Another possibility to explain the persisting incidence of KS would be the changing prevalence of risk factors for HIV infection in our area, for example, a higher prevalence of men who have sex with men, in whom human herpes virus 8 is more prevalent, would be expected to increase KS incidence. Such a change in risk factor in our patient population could lead to an improvement in the earlier diagnosis of HIV infection or improved access to treatment.
Of particular interest in this study was the outcome of KS in those who showed virological response to antiretroviral therapy (ART). It is not surprising to note that those who did not respond to ART did poorly, as these patients are similar to those of the pre-HAART era. However, even for patients who showed successful virologic control with HAART, but in whom there was less than 50 cells/mm3 increase in CD4 count, the outcome of KS was similar to those who had no virologic improvement (50% versus 55% mortality).
The clinical benefit of achieving virologic control prior to improvement in CD4 count is unclear from studies on other opportunistic infections. With cytomegalovirus (CMV) retinal infection, despite virologic control, immunologic improvement is required for prevention of progression of CMV disease. 9 For Pneumocystis pneumonia, however, cohort studies have shown a markedly lower incidence once virologic control is achieved, even prior to the improvement in CD4 count. 10 The results from our study suggest that for KS, no improvement in outcome is seen for those patients with <50 cells/mm3 increase in CD4 count.
Conclusion
The incidence of KS in Fresno County has shown no decline in the 14-year time period between 1998 and 2012. The overall 12-month mortality in patients diagnosed with KS from 1998 to 2012 was 30%. For patients with KS who were on successful HAART with virologic control (HIV VL < 400 copies/mL) having a >50 cells/mm3 increase in CD4 count, the 12-month mortality was 6%; for those with a <50 cells/mm3 increase in CD4, the 12-month mortality was 50%.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.