
Abstract
The Centers for Disease Control and Prevention have recommended routinely testing patients (aged 13-64) for HIV since 2006. However, many physicians do not routinely test. From January 2011 to March 2012, we conducted 18 in-depth individual interviews and explored primary care physicians' perceptions of barriers and facilitators to implementing routine HIV testing in North Carolina. Physicians' comments were categorized thematically and fell into 5 groups: policy, community, practice, physician, and patient. Lack of universal reimbursement was identified as the major policy barrier. Participants believed endorsement from the United States Preventive Services Tasks Force would facilitate adoption of routine HIV testing policies. Physicians reported HIV/AIDS stigma, socially conservative communities, lack of confidentiality, and rural geography as community barriers. Physicians believed public HIV testing campaigns would legitimize testing and decrease stigma in communities. Physicians cited time constraints and competing clinical priorities as physician barriers that could be overcome by delegating testing to nursing staff. HIV test refusal, low HIV risk perception, and stigma emerged as patient barriers. Physicians recommended adoption of routine HIV testing for all patients to facilitate and destigmatize testing. Physicians continue to experience a variety of barriers when implementing routine HIV testing in primary care settings. Our findings support multilevel approaches to enhance physician routine HIV testing in primary care settings.
Introduction
The plateau in the annual number of new HIV infections over the past decade suggests that national prevention efforts to decrease new HIV infections in the United States have not fully succeeded. An estimated 16% of the 1.1 million HIV-infected individuals in the United States currently remain undiagnosed and may unknowingly transmit their infections to others. 1,2 In an effort to identify more HIV-infected individuals, the Centers for Disease Control and Prevention (CDC) in 2006 recommended that health care providers test adolescents and adults for HIV, between the age of 13 and 64 years regardless of risk factors or behaviors. 3 This recommendation is called “routine HIV testing” or “screening.” The CDC also recommended the elimination of HIV pretest counseling and “written” informed consent. Posttest counseling should be limited to individuals testing HIV positive. In response, the majority of states have now modified their HIV testing laws to be consistent with the CDC’s recommendations. 4 Despite these changes in federal and state policies, only a minority of physicians report testing their patients routinely for HIV. 5 –7
Although several studies have reviewed barriers to physician HIV testing, 8,9 few have examined barriers as experienced and perceived by physicians since states have modified their HIV testing laws. 10 Fewer still have examined barriers to routine HIV testing in the south which has been disproportionately affected by the HIV/AIDS epidemic. 11 The purpose of this study is to explore the barriers and facilitators of implementing routine HIV testing from the perspective of community primary care physicians to inform the development of new approaches to promoting routine HIV testing in the south.
Methods
We conducted 18 in-depth individual interviews with North Carolina primary care physicians to elicit their perceived barriers and facilitators to routine HIV testing. We also asked participants to complete a self-administered 1-page questionnaire assessing their awareness, agreement, and adherence to routine HIV testing recommendations. Participants were reimbursed US$200 for their time. The study was reviewed and approved by the Office of Human Research Ethics Non-Biomedical institutional review board at the University of North Carolina at Chapel Hill.
Participants
Eligible physicians for this study were primary care physicians who had completed family or internal medicine residencies, worked in community-based ambulatory care sites, and spent at least 80% of their time directly caring for patients. We excluded primary care physicians who were also HIV specialists, correctional employees, or veterans administration physicians. We excluded these physicians because of the high adoption and adherence of routine HIV testing in their practice settings. 12 –14
We used a combination of random and purposive sampling methods to recruit primary care physicians from January 2011 until March 2012. First, we randomly selected 100 family and internal medicine physicians licensed in North Carolina from the publicly available North Carolina Medical Board Licensure Database. 15 We eliminated physicians who were also subspecialists from information retrieved from both the North Carolina Medical Board and physician practice Web sites. To enhance our sample size, we recruited additional physicians referred to us by participants and our research team. All recruited physicians received a personalized introductory faxed letter describing the purpose of the study and the eligibility criteria. We followed up a week later by phone to determine potential participant’s eligibility and interest. We conducted face-to-face interviews with physicians who practiced within a 30-mile radius of Chapel Hill, North Carolina (n = 7) and telephone interviews (n = 11) with physicians who practiced further away or were unavailable during office hours. The interviews lasted approximately 60 minutes, were audiotaped, and transcribed verbatim. All but 2 interviews were conducted by the corresponding author (B.L.W.).
Conceptual Framework
Based on existing theories and empirical data, we developed a novel conceptual framework of factors hypothesized to influence physicians’ routine HIV testing behaviors. This framework informed our interview guide and questionnaire. Our framework integrated key constructs from 2 existing theoretical models (1) the awareness-to-adherence model of physicians’ steps to clinical guideline compliance and (2) the information, motivation, behavioral skills (IMB) model of health behavioral change. 16 –19
The awareness-to-adherence model integrates constructs from the transtheoretical model of change, Roger’s Diffusion of Innovations Theory, and empirical studies. 16,19 According to the awareness-to-adherence model, when faced with new practice recommendations, physicians progress sequentially through 4 key cognitive and behavioral steps each of which are subject to mutable influences. Physicians first become aware of the recommendations, agree with the recommendations, adopt and correctly apply the recommendations, and adhere to the recommendations by applying it consistently. 20 Characteristics of the patient, physician, practice, guideline, dissemination, and environment can enhance or impede movement along each of these steps. This model has been successfully applied to identify physician barriers to clinical practice guideline adherence from a physician perspective for several chronic diseases. 16,21 –23
The IMB model of behavior change draws from fundamental constructs of social psychology (eg, attitudes and beliefs) known to affect behavior. Psychologists extending the IMB model to physician behavior suggest that “when providers have adequate information, motivation (attitudes, beliefs, social norms), and behavioral skills, they will integrate new behaviors into their practices.” 18(p214) We used the IMB model specifically because cognitive-affective barriers (eg, knowledge, attitudinal, and skill) were known to be associated with physician-initiated HIV testing. 8
Data Collection
Semistructured in-depth interview guide
A semistructured interview guide was developed by all authors to elicit salient barriers and facilitators to routine HIV testing. Barriers to routine HIV testing were ascertained by the question, “What currently prevents you from implementing routine HIV testing in your practice?” Facilitators to routine HIV testing were ascertained by the question “What would help or facilitate your implementation of routine HIV testing in your practice?” The interview guide consisted of additional domains that potentially influenced routine HIV testing including knowledge, attitudes, and beliefs about CDC’s routine HIV testing recommendations. We also asked participants to complete a 1-page survey on their awareness, agreement, and adherence to CDC’s routine HIV testing recommendations.
Qualitative Data Analysis
We (B.L.W. and J.W.) independently read and coded all the transcripts. The codes were based, in part, on deductive constructs from our conceptual framework. We looked for emergent codes in the transcripts and developed a final codebook. Data were coded systematically based on these deductive and emerging codes. We also looked for patterns and frequencies of codes across participants. Codes and quotations were managed using Excel. In addition to reported barriers and facilitators to routine HIV testing elicited from our interview guide questions, we classified factors that prevented or facilitated routine HIV testing as barriers and facilitators, respectively.
Quantitative Data Analysis
We used descriptive statistics to characterize the sample. All statistics were calculated using SAS statistical software, version 9.2.
Results
Demographics and Self-administered Survey Results
Of the 124 physicians who were randomly selected, 31 met our eligibility criteria and had publically available telephone/fax numbers. Twenty-five of the eligible physicians never returned our calls. Of the 6 remaining physicians, 5 agreed to participate. We were able to schedule 4 physicians for interviews. In contrast, 27 physicians were referred to us through snowball sampling by study participants or research staff. Of these referrals, 23 were eligible, of which 9 never returned our telephone calls and 14 agreed to participate and were interviewed. The majority of the 18 interviewees were family medicine physicians (n = 12) who provided primary care in urban health care settings. The participants reported seeing an average of 20 to 25 patients per day. Although all of the participants treated adult patients, some of the physicians (family medicine) treated children and adolescents. Asthma, diabetes, and hypertension were common diseases in their clinic population. Additional demographic information is provided in Table 1. Of the 18 interview participants, 15 completed the 1-page survey (Table 1). Of the 15 participants, 10 were aware of and agreed with the CDC’s routine HIV testing recommendations. However, only 2 participants reported adhering to the recommendation.
Characteristics of Physician Interview Participants and Results of Routine HIV Testing Questionnaire.
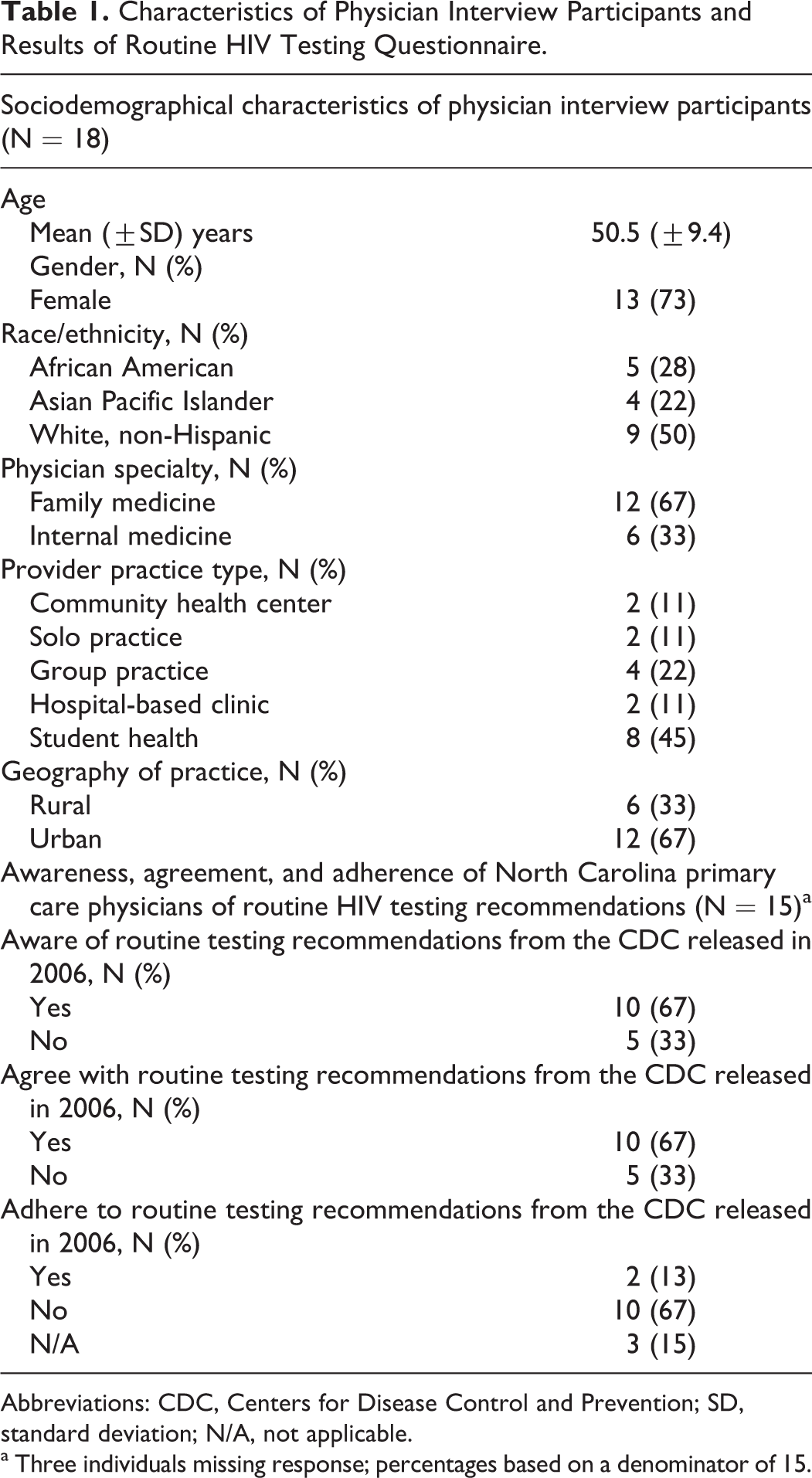
Abbreviations: CDC, Centers for Disease Control and Prevention; SD, standard deviation; N/A, not applicable.
a Three individuals missing response; percentages based on a denominator of 15.
Findings from Semistructured Interview
Physician participants described 21 barriers and 32 facilitators of routine HIV testing. We classified these barriers and facilitators according to their occurrence at 5 different levels of influence on routine HIV testing: policy, community, practice, individual provider, and patient (see Table 2). There were no differences in the types of barriers or facilitators reported between participants recruited randomly versus snowballing. Some of the barriers and facilitators with selected quotes from participants are as follows.
Perceptions of Barriers and Facilitators to Routine HIV Testing among North Carolina Primary Care Physicians.a

Abbreviations: CDC, Centers for Disease Control and Prevention; STD, sexually transmitted disease.
a N = 18.
Policy-Level Barriers and Facilitators to Routine HIV Testing
Barriers: The most widely perceived barrier (mentioned by 13 of 15 interviewees) to implementing routine HIV testing in primary care settings was perceived lack of third-party reimbursement. A rural male family medicine physician explains: Insurance coverage that would be a big issue. I mean if it’s not covered by insurance then I don’t think it’s going to happen.
Facilitators: Participants also identified factors they felt would facilitate routine HIV testing, many of which would require changes to existing policies. Factors identified included universal third-party reimbursement, elimination of the requirement for written consent, streamlining HIV pre- and posttest counseling, and requiring physicians to conduct routine HIV testing. In addition, some spoke of the challenges of keeping up with the literature to make informed decisions regarding testing. They believed that recommendations from trusted, unbiased authorities such as the US Preventive Services Task Force (USPSTF) could potentially facilitate routine HIV testing. A male rural family medicine physician explains: … I depend on groups like the AAFP [American Academy of Family Practice] and the Public Health Service [United States Preventive Services Task Force] because the Task Force, they have a fairly, in my opinion a fairly balanced group of folks that look at these things.
Community-Level Barriers and Facilitators to Routine HIV Testing
Barriers: Primary care physicians described several community barriers to HIV testing. These were social stigma associated with HIV, the conservative nature of some communities, and the lack of privacy available in small rural towns. A rural female family medicine physician remarks: … I think there is a perception around here that suggesting [they should get a test] means that they have been nasty, dirty, done something that they shouldn’t have done.
Another family medicine physician commented that HIV testing in rural communities was a little “touchy because of the connotations involved with it” especially in socially conservative communities.
A female rural family medicine physician explained how the perceived lack of confidentiality in rural communities could hinder HIV testing. Because we are in a rural area and people know people, you know there's a lot of fear in, “Oh, if I get tested and people find out …,” then there's this fear associated with being known because everybody knows everybody and everybody is related to everybody here.
Facilitators: Participants believed that public HIV campaigns would facilitate routine HIV testing by increasing community awareness and “legitimizing” the routine HIV testing policy. An urban female family medicine physician explains. So if they have a campaign and everybody has heard about it, when you ask the question it legitimizes the question and they can respond really easy.
In addition, interviewees felt that the use of a team effort (consisting of the government, the media, and subspecialists) would facilitate patient acceptance of routine HIV testing. A female urban family medicine physician explains. So I think it’s a team effort. The primary care doctors can definitely help implement something, but we have to have a plan. We just can’t do it on our own.
Provider-Level Barriers and Facilitators to Routine HIV Testing
Barriers: Physician participants reported multiple factors interfered with providers implementing routine HIV testing: lack of habit of testing, underestimating patients’ risks, lack of awareness of HIV as a problem, discomfort communicating about HIV testing, and concerns of cost-effectiveness of HIV testing. A male rural family medicine physician explains. I guess my philosophy in any kind of screening is I want to see proof … I have to prioritize my time very much. And to me PSA [test for prostate cancer] is way at the bottom of that priority list, and I kind of feel like that’s where HIV is right now in this.
Other participants reported HIV risk misperceptions as barriers. A female rural family medicine physician comments: Because there are some people who have this idea of, oh yeah, there are people who have so-called “class,” who can't get anything.… I'm like, that doesn't mean they can't get HIV.
Facilitators: Facilitators included patient requests, USPSTF A-level recommendation, and physician HIV education. Several participants stated that educating primary care physicians on the rationale behind routine HIV testing would facilitate testing. An urban female internal medicine physician stated: Show me the numbers and show me data as to why I should do it on every patient.
Perceived Patient Barriers and Facilitators to Routine HIV Testing
Barriers: Participants believed that fear of needles, HIV testing costs, and patient refusal are all barriers to routine HIV testing for patients. Participants also reported that stigma and perception of low risk were also barriers. An urban female family medicine physician reflected: I think stigma is part of it. People still have a perception of stigma with HIV and also the seriousness of the diagnosis. And then I guess not understanding who is at risk, who is not at risk, or misperceptions about who is at risk and who is not at risk.
However, several participants remarked that male gender was also a barrier to routine HIV testing. A female urban internal medicine physician explained: Getting-married males, in the last, like, four months I’ve had a couple of them. I thought they wanted it and they said no. Then they left and didn’t get it drawn.
A female urban family medicine physician remarked that men, especially at high risk, were more likely than women to refuse testing: … it seems like we have more men will turn it down than women. Women are ready to… I want to know, I want to know. Guys are more likely to have a reason not to get tested, especially if they are at high risk.
Facilitators: Several patient factors were perceived to facilitate routine HIV testing. These factors included patient request, adoption of routine testing for all patients, programs to increase patient’s acceptance, patient education, and counseling. However, the most salient facilitator was patient request. In fact, none of the respondents reported ever refusing a patient’s request for HIV testing even if they felt HIV infection was unlikely. For example, a female urban internal medicine physician recalls agreeing to test an anxious patient although she felt that HIV testing was not indicated: A patient already had an HIV test by somebody else, like two weeks ago or something like that. So sometimes you just have to do these things. She said, I know I am ridiculous, and I’m going to see a counselor [about her anxiety that she may be HIV positive despite testing HIV negative], but I just want it anyway. Refuse? I never refuse. I tell them it’s not reasonable, like this girl. And then I talk with them until I know that they just want it, and then I go with the request.
Practice-Level Barriers and Facilitators to Routine HIV Testing
Barriers: Physicians reported many practice barriers to routinizing HIV testing including practice policies not consistent with CDC’s recommendations, different locations for HIV testing and primary care, and small practices not up to date on recommendations. However, most common were competing clinical priorities and lack of time. A male rural family medicine physician commenting on competing clinical priorities remarked: we have patients who come in with really bad stuff, and taking the time out to do an HIV testing, which again is not really a huge thing on the agenda, … HIV kind of falls way, way down on the list do it.
Lack of time was universally identified as a barrier to routine HIV testing and preventive services in general. A female urban internal medicine physician comments: So I think time is a huge barrier. And I read an article recently that said to be the perfect family physician, you have to basically work 24 hours a day just to get the basics done. It’s just overwhelming. So I think that’s part of the issue is too much going on and too little time to spend with them.
An urban female family medicine physician explains how oral HIV tests increase physician time: I think it’s more a barrier for us to do the OraQuick here. I would rather do the blood test. Let them get the blood draw[n], let them leave. With the OraQuick I have to … bring the patient to my office [and wait for and interpret the test results] between [seeing] my other patients. For us OraQuick is more a barrier even though it’s cheaper than the blood test.
Facilitators included use of oral HIV tests, testing during initial/wellness visits, and routinizing testing into the clinical work flow, including HIV testing as part of a sexually transmitted disease panel and delegating testing to nurses. A female rural family medicine physician participant who has successfully implemented routine HIV testing in her practice describes the process of nurse initiated testing: The nurses have been put in charge of asking the patients even before I go into the room, do they want to be screened for HIV. And they can actually put in the lab order without me having to put in anything. And if a patient refuses, they actually document that in the patient's notes as well.
However, some physicians expressed concerns that some nurses may perform these duties better than others. Another rural female family medicine physician commented: You don't want a nurse telling somebody one thing, and somebody else telling them something else.
Discussion
Our primary care physician participants reported not routinely testing for HIV. They reported similar barriers found in prior studies on implementing routine HIV testing in primary care settings. 24,25 These barriers and facilitators occurred at the policy, community, practice, physician, and patient levels. Using our research findings and the empirical literature, 21 we explore subsequently how potential facilitators of routine HIV testing can be used to address the major barriers at each of these 5 levels, to move physicians along the path from awareness to adherence.
Policy
Our participants identified state policies requiring “written” HIV informed consent and pretest counseling as current barriers, despite the elimination of both requirements from North Carolina Health Law in 2007. 26,27 Our participants recommended continuing medical education programs to increase policy awareness. However, the recent USPSTF A-level recommendation for routine HIV screening may be an even greater facilitator to move physicians from awareness to adherence. Recommendations from trusted authorities have been associated with physician agreement. 21 Further, A-level endorsements from the task force may facilitate adoption and adherence. Under the Affordable Care Act, private health insurers will be required to cover A-level or B-level endorsed USPSTF recommendations.
Community
HIV/AIDS-associated stigma was cited as a major community barrier, particularly by rural physicians. They recommended HIV testing campaigns to introduce the concept of routine HIV testing to the broader community. Physicians believed that this approach would decrease HIV/AIDS stigma and increase community HIV testing acceptance.
Patients
Our participants believed that patient barriers, such as patient refusal, can affect physician adoption and adherence to routine HIV testing. However, studies show that most patients are receptive to HIV testing when recommended by their physician. 8,28 In fact, a recent survey of physicians’ and their patients’ attitudes about HIV testing concluded that “there continues to be a major disconnect between individual patients’ willingness to be tested for HIV and doctors’ perception of this willingness. This disconnect continues to lead to less testing than patients perceive as appropriate.” 28(p421) Educating physicians about this disconnect may enhance physician adherence. 8 In addition as recommended by our participants, educating patients about HIV risk may enhance physician–patient communication about HIV testing.
Practice
Our findings show that time constraints and competing clinical priorities are major practice-level barriers influencing the adoption of and adherence to routine HIV testing. Our findings are consistent with those of other studies showing these barriers in clinical practice. 8,24,29 In fact, rapid HIV testing, an intervention to facilitate HIV testing, was a barrier because of the increase in physician time involved with test interpretation during the clinic visit. As suggested in this study’s findings, screening during wellness visits and delegating HIV testing to nursing and office staff may overcome barriers posed by time constraints and competing clinical priorities. Nurse-initiated HIV testing has been associated with greater receipt of HIV testing than physician-initiated testing in Veterans Affair primary care settings. 30 Participants in our study also advocated creating systems to integrate HIV testing into the clinical work flow. Clinical reminders and prompts have increased adherence to guidelines in ambulatory care settings. 31 –33
Physicians
Our participants perceive that other North Carolina primary care physicians lack awareness of HIV testing recommendations and community HIV prevalence. They also believed that primary care physicians were unaware of the cost-effectiveness of routine HIV testing. Our participants recommended educational interventions to address these problems. However, interventions that combine social marketing, provider feedback, and provider activation may be even more effective than education alone at enhancing provider adherence to routine HIV testing. 34,35
Limitations
Our study sample was small and mostly nonrandom, so it may not be generalizable to primary care physicians in North Carolina or the United States. In addition, our different interview methods (face to face versus telephone) may have elicited different results. 36 However, our study has a number of strengths. First, this is one of the few studies to elicit perceived barriers and facilitators to routine HIV testing among primary care physicians in the southeastern United States. Second, the sample was comprised of a highly diverse group of primary care physicians with respect to race, ethnicity, gender, and practice geography. Our study is also one of the few studies on physician barriers to prevention activities at the beginning of the implementation of the Patient Protection and Affordable Care Act (ACA). In states that participate in the ACA, private and public health insurers will be required to pay for preventive services at no additional cost sharing for patients.
Conclusions
In summary, current HIV-related policies, community stigma, practice financial environment, physician attitudes, and patient acceptance continue to be the most salient barriers for primary care physicians. Our participants recommended financial policy changes (universal reimbursement) to address the practice financial testing barriers and HIV education programs to change physician attitudes and patient acceptance. Our participants also endorsed community HIV testing campaigns to decrease HIV stigma. Our physicians believed that delegation of HIV testing to nurses would improve implementation in primary care settings. Our findings support multilevel approaches integrating several initiatives (eg, social marketing, policy changes, and clinic reminders) to addressing these multiple barriers. 35,37
Footnotes
Acknowledgments
We would like to thank our participants for their time and comments. We would like to thank Megan Katsaounis, Dr Pamela Love, and the Durham Academy of Medicine for assistance with participant recruitment. We would like to thank Drs Carlton Moore and Srilatha Edupuganti for providing early feedback on the interview guide. We would like to thank Mr Paul Mihas and the UNC Odum Institute for Social Sciences for their assistance with qualitative analysis.
Authors’ Note
For prior presentations: Why don’t NC Physicians Screen for HIV? Development of an Intervention to change physician behavior. Young HIV investigator symposium. Center for Aids Research, University of North Carolina School of Medicine, Chapel Hill, North Carolina. November 30, 2013.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was supported by a