
Abstract
Background:
We sought to measure resident physician knowledge of HIV epidemiology and screening guidelines, attitudes toward testing, testing practices, and barriers and facilitators to routine testing.
Methods:
Resident physicians in internal medicine, pediatrics, obstetrics and gynecology, and emergency medicine were surveyed.
Results:
Overall response rate was 63% (162 of 259). Half knew details of the HIV screening guidelines, but few follow these recommendations. Less than one-third reported always or usually performing routine testing. A significant proportion reported only sometimes or never screening patients with risk factors. This was despite a strong belief that HIV screening improves patient care and public health. The most common barriers to testing were competing priorities and forgetting to order the test. Elimination of written consent and electronic reminders was identified as facilitators to routine testing. Although an institutional policy assigns responsibility for test notification and linkage of HIV-positive patients to care to the HIV care program, only 29% were aware of this.
Conclusions:
Few resident physicians routinely screen for HIV infection and some don’t test patients with risk factors. While competing priorities remain a significant barrier, elimination of written consent form and electronic reminders has facilitated testing. Increasing the awareness of policies regarding test notification and linkage to care may improve screening.
Introduction
At the end of 2009, the Centers for Disease Control and Prevention (CDC) estimated that in the United States, 1 148 200 individuals older than 13 years of age were living with HIV infection, with 18.1% of these individuals undiagnosed. 1 It is estimated that an additional 50 000 individuals become newly infected each year. 1 Delays in diagnosis lead to increased probability of disease transmission. Individuals unaware of their diagnosis are 3.5 times more likely to transmit HIV sexually than those who are aware and are responsible for over half of the new infections acquired via sexual transmission. 2 Earlier diagnosis has significant benefits at both the individual and the societal level. Once a diagnosis is established, antiretroviral therapy (ART) has been found to significantly extend AIDS-free survival and decrease overall mortality. 3 All these reinforce the value and benefit of appropriate screening and timely diagnosis.
In 2006, the CDC released revised guidelines regarding HIV testing in order to promote increased HIV screening, foster earlier detection, and connect those infected to appropriate care. It is now recommended that everyone between the ages of 13 and 64 undergo routine, voluntary HIV testing in all health care settings, unless they opt out. For those at high risk of infection, screening should be performed annually. Separate written consent and prevention counseling should not be required as a part of screening. 4 Expansion of routine HIV screening regardless of risk has increased engagement in HIV treatment and has been associated with decreases in community viral load (VL) and HIV transmission. 5 This is in line with the recent data that suggest that effective highly active ART (HAART) decreases transmission by 96%. 6 Multiple influential organizations including the American College of Physicians, the American Medical Association, and, more recently, the US Preventive Services Task Force) have endorsed the CDC’s recommendations, but provider uptake of the guidelines has been slow. Even legislation has not influenced routine screening rates in the general population as it did for pregnant women. Yehuda and colleagues recently reported that over 90% of eligible patients admitted to a major hospital in New York City were not offered testing by resident physicians even though the state law demands this. 7
Resident physicians are in contact with a high volume of patients in a variety of health care settings and are thus key providers for screening and diagnosis. House staff are trained about screening and health maintenance for many chronic medical illnesses, such as hypertension, hyperlipidemia, colon, cervical, and breast cancer. There are limited data regarding HIV-related knowledge, testing behaviors, and beliefs among residents. Jain et al studied 450 internal medicine (IM) residents in New York City in 2007 and found that only 32.6% were aware of the updated guidelines. The majority used a risk-based screening approach as opposed to routine testing, and over half stated they would order more tests if oral consent was available. 8 The works of Mohajer et al and Phillips et al again underscored the substandard knowledge of screening guidelines and practices among residents. 9,10
Given the pivotal role resident trainees play in implementing the CDC guidelines for routine HIV testing, we performed a cross-sectional survey of IM, emergency medicine (EM), obstetrics and gynecology (OBGYN), and pediatric resident trainees in order to characterize their HIV screening knowledge, attitudes, and behaviors as well as the perceived barriers and facilitators to routine testing.
Methods
Environment
In the city of Chicago, over 21 000 people are known to be living with a diagnosis of HIV, and the prevalence rate of 761 per 100 000 is nearly 3 times the national rate. 11 The University of Chicago Medicine (UCM) is a tertiary care center on the South Side of Chicago where the prevalence rates of HIV are even higher. The institution has received funding from the Chicago Department of Public Health for expanded HIV testing in disproportionately affected populations in health care settings. In order to facilitate improved screening, our urban facility removed the requirement for written consent, implemented electronic reminders for HIV testing, and developed a formal linkage to care program. In fact, the institutional policy now assigns the responsibility for HIV test notification and linkage to care to the HIV care program. An experienced social worker reviews a weekly report of the patients who were tested for HIV and the results of that testing. The social worker performs test notification and schedules a clinic visit with an experienced HIV care provider at the time of notification. Additionally, an educational campaign that presents the case for routine screening and highlights the institution’s formal linkage to care program has been developed and rolled out. All aspects of the HIV testing and linkage to care program have been the subject of hospital-wide electronic notification, the same system for disseminating new information about other policies and procedures within the medical center.
Study Sample and Data Collection
We administered a paper questionnaire to IM, EM, OBGYN, and pediatric residents at the UCM, an urban academic medical center, and to IM residents at Mercy Hospital, a community hospital affiliated with the University of Chicago. All questionnaires were administered in person between February 24 and May 1, 2012. Individual pager numbers were collected on the cover sheet of each questionnaire in order to track who had and had not completed the questionnaire, but the cover sheet was separated from the results prior to data entry and analysis in order to ensure confidentiality and anonymity. Participation was voluntary and most questionnaires were completed prior to educational conferences. Those residents who did not attend the educational conference at which the questionnaire was administered were paged and given the opportunity to complete the questionnaire in person at a later date. This study was approved by the Institutional Review Boards at both the UCM and Mercy Hospital.
Survey Instrument
The survey consisted of 30 closed-ended questions divided into seven sections: HIV epidemiology knowledge, HIV screening knowledge, HIV testing behaviors, barriers and facilitators to screening, HIV testing beliefs, public health reporting, and partner notification. Demographics included age, gender, primary specialty, and postgraduate year (PGY). Survey items were adapted from previous literature about provider barriers to HIV testing as well as other surveys. 8,12 –14 The questionnaire was pilot tested among potentially eligible participants and modified accordingly.
Knowledge related to HIV was assessed by having respondents identify the most common mode of HIV transmission in the United States, the prevalence of HIV in Chicago, the percentage of HIV-infected people unaware of their diagnosis, and the effect of ART on heterosexual transmission of HIV. Knowledge of the most recent CDC HIV testing recommendations was assessed by asking about the familiarity with opt-out screening, the upper age limit for routine screening, and the frequency of testing in high-risk patients. Knowledge regarding the follow-up of test results, public health reporting, and partner notification was also assessed.
HIV testing practices were assessed by asking respondents how often they offered HIV tests to outpatient, inpatient, and emergency room patients (a) without risk factors for HIV, (b) with at least one risk factor for HIV, and (c) who are pregnant (never/sometimes/usually/always). Respondents were also asked to quantify how many patients they had screened for HIV in the clinic, hospital, and emergency room in the month prior to completing the questionnaire.
The presence of patient-level, physician-level, and structural barriers and facilitators to HIV screening was assessed based on a list that was created after the review of the literature as well as input from physicians and potentially eligible respondents.
Attitudes and beliefs regarding routine HIV screening were assessed by asking respondents to state whether they agreed strongly, agreed somewhat, disagreed strongly, or disagreed somewhat with the following statements: (a) routine HIV screening will improve public health in my community, (b) routine HIV screening will benefit my patients, (c) routine HIV screening will negatively affect my ability to meet the other needs of my patients, (d) routine HIV screening is an admirable goal but is an unreasonable burden for most physicians and health care centers, and (e) routine HIV screening is not a judicious use of funding and health care resources.
Statistical Analysis
Basic descriptive statistics were calculated for all survey questions. Response proportions were compared using the continuity corrected χ2 tests at the level of 5% significance. Med-Peds physicians were combined with physicians in IM for the purpose of the analysis. Separate analysis was conducted to determine the relationship between HIV testing behaviors and demographics and knowledge and attitudes. In order to perform this analysis, γ correlation coefficients were used to correlate ordinal testing behavior responses (always and usually were considered a positive response and sometimes or never were considered a negative response) with binary indicators of correct response to specific questions of interest. For each question, respondents who indicated that the question was “not applicable” were excluded from calculation of that γ correlation coefficient. Logistic regression models were used to correlate HIV testing behaviors (always/usually versus sometimes/never) with respondent demographics (age, year of training, and specialty), HIV-related knowledge (total number of correct responses), and attitudes toward routine screening (total number of positive responses). STATA v11 (StataCorp LP, College Station, Texas) was used to complete all statistical analysis.
Results
Two hundred and five trainees responded, yielding an overall response rate of 67% (205 of 307). Fifty percent of respondents were female, 38.24% of respondents were in the first PGY (PGY1), 29.9% were in the second PGY (PGY2), and 31.86% were in the third PGY (PGY3) or higher (see Table 1).
Resident Physician Demographics.a

Abbreviations: PGY, postgraduate year; OBGYN, obstetrics and gynecology.
aN = 205.
Knowledge
Knowledge of HIV epidemiology was suboptimal (see Table 2). Less than half of all house staff knew (1) the most common mode of transmission in the United States, (2) the percentage of people with HIV infection who are unaware of their diagnosis, (3) that treatment of HIV reduces transmission by 96%, and (4) the overall prevalence of HIV infection in Chicago. Interestingly, IM residents at our community hospital affiliate were significantly more knowledgeable than UCMC IM, EM, OBGYN, and pediatrics residents regarding the most common mode of HIV transmission in the United States (48.8% correct versus 18.6%, 20%, 6.3%, and 26.5%, respectively; P = .005). Pediatric residents were significantly more knowledgeable regarding partner notification requirements (P = .0013).
Differences in HIV-Related Knowledge among Resident Trainees, February to April 2012.a

Abbreviations: OBGYN, obstetrics and gynecology; IM, internal medicine; EM, emergency medicine; NA, not applicable; UC, University of Chicago.
aN = 205.
Knowledge regarding the details of the CDC’s HIV testing recommendations was variable. Although 47% correctly identified the opt-out component of the recommendation, 69% were not familiar with the age-based recommendations for testing. Seventy-eight percent knew high-risk individuals needed repeat testing, and although UCM IM residents appeared to be more knowledgeable than the other resident groups regarding this detail, the difference approached but did not reach significance (P = .06).
Knowledge of local and institutional policies was mixed. Only the EM residents were familiar with our institution’s notification and linkage to HIV care program (P < .00001).
Attitudes
Attitudes regarding routine HIV screening were overwhelmingly positive (see Figure 1). The majority of residents agreed that HIV testing is important for patients and the community (98%) and would not interfere with meeting the other needs of their patients (86.7%). They also felt HIV screening was not an unreasonable burden (69.9%) or waste of health care resources (76.8%).

Resident attitudes toward routine HIV screening.
Testing Behaviors
Despite positive attitudes regarding routine screening, few residents reported consistent (always or usual) utilization of such a testing approach (30.6% in the outpatient clinic, 24.4% in the hospital, and 15.9% in the emergency department [ED]). Moreover, some residents do not order HIV tests in patients with known risk factors for HIV. This was most pronounced in the ED setting, where 13.8% of residents reported never ordering HIV tests in patients with 1 or more risk factor for HIV (see Table 3).
Frequency with which HIV Testing Is Performed by Setting February to April 2012.a

Abbreviation: NA, not applicable.
aN = 205.
Barriers and Facilitators to Testing
Residents most frequently identified competing priorities (59.8%), not thinking of it during the clinical encounter (52.9%), patient refusal (52.9%), and insufficient time (43.6%) as barriers to routine HIV testing (see Figure 2). The most frequently cited facilitators to routine testing included institutional elimination of the written consent form (67.8%), electronic reminders (46.5%), reminders from attending physicians or preceptors (35.6%), and the 2006 revision of the CDC guidelines (28.2%; Figure 3); 90.7% would be in favor of having nursing obtain consent and facilitate testing.
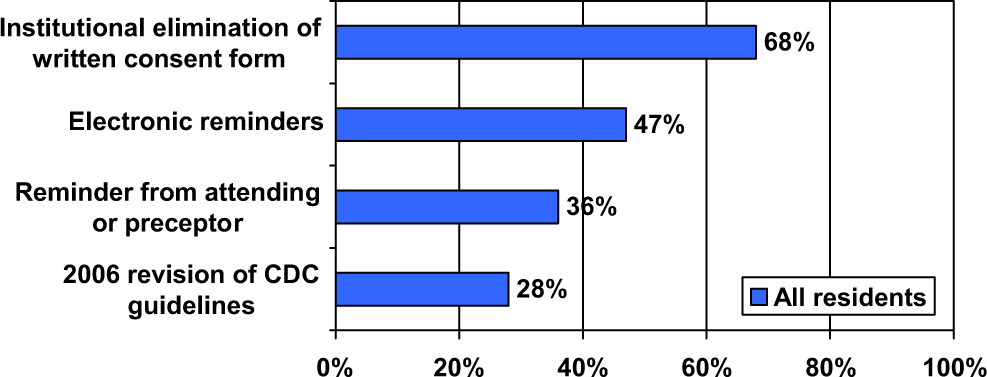
Facilitators to routine HIV testing (N = 202).

Barriers to routine HIV testing (N = 204).
Logistic Regression Analysis
Age, experience (PGY1-2 vs 3-4), knowledge (total number of correct responses to knowledge questions), and attitude (total number of “positive” responses to attitude questions) did not correlate with routine (ie, testing of all patients younger than 64 years of age) or targeted (ie, testing those with at least 1 risk factor for HIV) testing frequency in any setting (outpatient clinic, hospital, or ED). In hospitals, residents who specialized in EM were less likely than those in IM to offer both routine (P = .033) and targeted testing (P = .0036). Non-IM residents (ie, pediatrics, OBGYN, and EM) were less likely than IM residents to perform targeted testing on hospitalized patients.
Discussion
In this survey regarding HIV-related knowledge, attitudes, and testing behavior among resident trainees practicing in underserved communities with high prevalence rates of HIV on the South Side of Chicago, our findings reveal that residents are not very knowledgeable about HIV epidemiology and testing guidelines.
The differences in HIV-related knowledge noted between the various resident groups may reflect diverse exposures to educational programming as well as different efforts to promote testing. That said, we cannot easily explain the interesting finding that IM residents in a community hospital residency program were significantly more knowledgeable about the risk factors for HIV than residents in our university training programs. We enquired as to whether or not the community hospital residents had received prior educational programs on HIV screening, and this was not the case. Another possible factor is that many of the community hospital residents received their medical degrees outside the United States in areas with much higher prevalence rates of HIV, and they thus had more overall exposure to HIV even prior to residency. Finally, it is possible that local data or individual resident experience influenced the response to the questions about the mode of HIV transmission. Although men who have sex with men (MSM) is the single greatest risk factor for HIV acquisition in the United States, our HIV screening program has identified more patients who have acquired HIV by high-risk heterosexual behavior than HIV screening programs working outside of the health care settings. This would certainly explain why OBGYN residents scored lowest in this domain. Similarly, we are not sure why pediatric residents were most knowledgeable about partner notification requirements but would hypothesize that this may be in part because their training is by nature more family and even public health centered than the other specialties surveyed. The ED residents were much more knowledgeable about the institutional protocol for follow-up of HIV-positive tests, and this is likely explained by the fact that our group has greatly focused our programming efforts on testing in the ED.
We also found that residents are not routinely offering HIV tests as recommended by the CDC and other important and influential medical groups. These findings are consistent with other studies showing that adoption of routine screening remains low, even 6 years after the release of the CDC guidelines. Importantly, this infrequent adherence to the guidelines was independent of knowledge related to HIV epidemiology and testing guidelines. Additionally, this was in spite of overwhelmingly positive attitudes regarding both the individual and public health–related benefits of routine HIV screening. Changing physician behavior will require a clear understanding of the barriers to routine HIV screening, and our study suggests important barriers to adoption of routine screening that likely contribute to both a knowledge–behavior and belief–behavior gap.
The most frequently identified barriers to routine screening were (1) competing priorities (59.8%), (2) not thinking of it during the clinical encounter (52.9%), (3) patient refusal (52.9%), and (4) insufficient time (43.6%). Although our institution no longer requires written consent for HIV testing, 26.5% of residents reported that the “cumbersome consent process” was a barrier to testing. The reported barriers were similar to those described in other studies of resident physicians, and many of these barriers have been or can be addressed at the institutional level. 8,9 For example, electronic alerts or reminders and elimination of the written consent form can reduce the impact of barriers (1) and (4). In accordance with this, the most frequently cited facilitators to routine testing included institutional elimination of the written consent form (67.8%) and electronic reminders (46.5%). Additionally, utilizing support staff for routine screening may free residents to use their limited time to address other issues or the so-called competing priorities. Physicians in this study were overwhelmingly supportive of this idea as over 90% were in favor of having nursing obtain consent and facilitate testing. Notably, at least two separate studies have shown that doing so would not alter patient acceptance rates. 15,16
It is difficult to determine if some reported barriers to screening may be perceived rather than true barriers. Education addressed at deconstructing these barriers is crucial. This is the case with the third most frequently cited barrier in our study––patient refusal. Although we do not have formal data on patient acceptance of testing at our institution, the high number of residents (53%) reporting that patient refusal to HIV screening was a major barrier was surprising and contrary to both prior studies and our own local experience anecdotally. For example, in our ED, triage nurses are often the first to approach patients about HIV screening, and they do not perceive patient refusal to be a significant barrier. Recent studies demonstrate low rates of patient refusal, especially in high prevalence settings such as the South Side of Chicago. This is especially true in other countries where HIV infection is an even greater problem. In a study performed in Ugandan hospitals, where the HIV prevalence is 28%, virtually all patients (98%) accepted testing. 17 Acceptance rates may be lower in the United States but are still very high. Most of the data on HIV test acceptance rates in the United States comes from ED-based screening programs, but patients also seem to be very accepting of screening in other areas, including dental clinics. 18 Nevertheless, reported acceptance rates have ranged from 39% to 91% in the ED alone. Freeman et al reported that 91% of patients offered testing in an ED accepted, and they also found that white and married patients were less likely to accept testing. 19 Another study of ED patients by Haukoos et al reported a patient acceptance rate of 81%, regardless of whether testing was opt-out or opt-in. 20 Brown and coworkers reported that 59.7% of ED patients accepted testing. 21 In another study by Brown et al, acceptance was 53%, and the most common reasons for refusal were that patients did not perceive they were at risk (49%) or they had been tested previously. 22 In a study by Merchant and coworkers, however, only 39% of ED patients accepted HIV testing, with patients who were white, married, younger than 45 years, and having private medical insurance more likely to refuse testing. 23 Christopoulos and colleagues tried to understand patient reasons for the basis of patients accepting or refusing HIV screening and surveyed patients who were offered screening and compared those who accepted and those who refused screening. Some patients refused screening for understandable reasons, including the feeling that they were at low risk, while others admitted that they refused testing because they feared the psychosocial ramifications of being diagnosed with HIV infection. 24,25
One underexplored but important facilitator of routine testing is encouragement by attending physicians and preceptors. A survey performed in 2009 found that only 53.4% of clinician educators encouraged trainees to perform routine HIV screening, and yet this was the third most frequently cited facilitator of testing in our study. 26 Clinician educators have an important role in the dissemination of the recommendations regarding universal testing, and interventions to improve faculty encouragement of testing could have a significant impact. Our study also shows that a reminder from a supervising attending or preceptor would positively influence resident behaviors. Although we have focused our attention on resident knowledge, attitudes, and behaviors, it will be just as important to continue to promote HIV screening to attending physicians and to make attempts to understand their knowledge and beliefs regarding HIV screening.
Our study findings should be interpreted in the context of several limitations. First, HIV screening behaviors were self-reported and may not accurately reflect actual screening practices. Second, our center provides care to a largely underserved population with a relatively high prevalence of HIV and may not be generalizable to areas with low prevalence rates of HIV. Finally, due to the large number of statistical tests performed and skewed distribution of respondents by specialty and institution, the results generated may have occurred by chance alone. There were many more residents in IM (113 of 205) compared to the other specialties, and the small number of residents surveyed at the community hospital were all IM. These factors, along with a relatively small sample size, make it difficult to assert that our findings are definitive.
In conclusion, this study finds that house staff HIV-related knowledge, including familiarity with details of the 2006 CDC recommendation regarding routine HIV testing, is suboptimal. Moreover, self-reported HIV screening behaviors are not reflective of resident physicians’ overwhelmingly favorable beliefs regarding the individual and public health benefits of routine screening. System changes such as electronic alerts and streamlined consent processes are perceived as important facilitators of testing but do not guarantee improved testing behavior. 27 While legislative changes led to a significant improvement in prenatal HIV screening rates, the same has not been true for routine HIV screening. Expanded HIV screening will require cultural changes in physician behaviors. Education and interventions targeted at reducing and demystifying the most frequently cited barriers will likely increase adoption of universal HIV testing.
Footnotes
Acknowledgments
The authors would like to acknowledge the residents who participate in the survey as well as those who provided time for survey administration including the program directors and chief residents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr David Pitrak receives grant support for expanded HIV testing from Gilead (HIV FOCUS).