
Abstract
Physicians are not routinely offering patients HIV testing, partly due to perceived patient discomfort with discussing HIV. This study assessed patients’ comfort level and whether physician recommendations can overcome any discomfort that does exist. In a publicly funded primary care clinic, we administered a survey exploring patient facilitators to HIV testing, with 266 patients answering the 2 main survey questions of interest. Most participants wanted their physician to offer HIV testing (n = 175; 65.8%). Even among participants who did not want their physician to offer HIV testing (n = 91), over half (n = 54; 59.3%) reported they would “likely” or “very likely” accept HIV testing if their physician recommended it. Based on our findings, not only are negative attitudes about HIV testing among patients uncommon but physician recommendations may be able to convince patients to receive HIV testing in spite of patients stating they do not want the test.
Introduction
Over 1.2 million people in the United States are living with HIV. Unfortunately, 15% of them are unaware they are infected. 1 Because of the benefits of earlier diagnosis of HIV, the US Centers for Disease Control and Prevention (CDC) has recommended since 2006 that all patients aged 13 to 64 in high HIV prevalence areas of the United States receive routine screening for HIV. 2 Most recently, in 2013, the United States Preventive Services Task Force (USPSTF) also updated their HIV testing recommendation to support routine testing of all adults. 3 According to the CDC’s most recently available data, 55% of people in the United States have never been tested for HIV. 4 Furthermore, national surveillance data have revealed that 23% of people diagnosed with HIV are simultaneously diagnosed with AIDS, highlighting years of missed opportunities for HIV testing to avert such diagnoses. 5 Early HIV diagnosis allows infected individuals to begin life-saving antiretroviral therapy to prevent HIV-associated morbidity and mortality. 6 Additionally, early diagnosis and treatment of HIV can reduce by 96% the risk of transmission to others by decreasing the infected individual’s viral load. 7
One way of improving HIV testing rates is for physicians to recommend the HIV test to patients, as studies have shown that a physician recommendation for HIV testing can help convince patients to get the HIV test. 8 –10 Despite the potential of physician recommendations to improve HIV testing behavior, physicians do not routinely offer the HIV test. 11 –14 One barrier to physicians offering the HIV test is physicians’ belief that patients may be offended or refuse the test. 14,15
Study Objective
With physicians’ perceived patient discomfort with HIV testing being a barrier to offering the HIV test, the objective of this study was to determine the patient’s perspective by assessing whether patients want their physician to offer them an HIV test. We also sought to determine whether a physician’s recommendation for testing could influence HIV testing acceptance by the patients. This study will help address the gap in knowledge of patients’ comfort level with physician recommendation of HIV testing and whether a physician recommendation can overcome any patient discomfort that does exist.
Methods
This study took place between June 2014 and February 2015 in a publicly funded primary care clinic in Houston, Texas. This clinic is in an area of the city with a high rate of HIV diagnoses. 16 Using a convenience sample of waiting room patients, we recruited adult patients to complete a paper-and-pencil survey. There were posters on display in the clinic to advertise the study, and a research assistant was present at a designated research booth onsite in the clinic to explain the study and enroll participants. When enough study staff were available at the clinic, one member of the study team also stood by the main clinic door to ask patients if they would like to participate in the study. Patients were eligible if they were older than 18 years and were receiving health care at this primary care clinic. Patients who were eligible and interested were given a cover letter describing the purpose and voluntary nature of the study. Verbal consent was obtained. Participants received a US$10 gift card to a local grocery store upon completing the survey. The institutional review board of Baylor College of Medicine approved this study.
Survey Instrument
The research team developed a survey to explore patient facilitators to HIV testing, with a specific focus on patient– physician communication. This study focuses on 4 specific survey questions of interest. We first examined responses to the question, “What would convince you to get tested for HIV?” There were multiple possible responses presented for answering this question (eg, a, b, and c). Participants could select as many responses as were appropriate for them. We then evaluated participant responses to the yes/no question, “Has your doctor ever recommended that you be tested for HIV?” We additionally examined responses to the following 2 questions: “Do you want your doctor at this clinic to offer you an HIV test?” and “How likely would you be to accept an HIV test if your doctor recommended it?” The former was a yes/no question, and the latter used a Likert-type scale of “not at all likely,” “somewhat likely,” “likely,” and “very likely.” Standard demographic questions were also asked as a part of the overall survey.
Data Analysis
These analyses included only patients who completed the survey in English. Two research assistants independently abstracted the data from paper surveys into a Microsoft Access database (Microsoft Corporation, Redmond, Washington). Stata 13 (StataCorp, College Station, Texas) was used for the analyses. Data entry discrepancies were mediated by members of the research team. Standard descriptive statistics were calculated. For categorical variables (gender, race, ethnicity, education level, and income) and responses regarding HIV testing, participants’ responses were summarized as simple proportions. For the continuous variable, age, median, and interquartile range (IQR) were calculated. Differences between demographic groups in this study’s outcomes of interest were compared using χ2 or Fisher exact test, as appropriate. 17
Results
There were 285 patients who participated in the survey; 281 participants answered at least one of the questions of interest for this study. The median age of these 281 participants was 54 years (IQR = 46-59 years), and the majority (67.9%) of these participants were female. The largest racial group represented was black/African American (43.4%), while approximately one-fifth of the participants were Hispanic/Latino (21.7%). Almost half (49.5%) of the participants had received at least some college education. Finally, three quarters (75.1%) of participants had a yearly household income of less than US$20 000. See Table 1 for the demographic characteristics of this study’s sample.
Demographic Characteristics.a
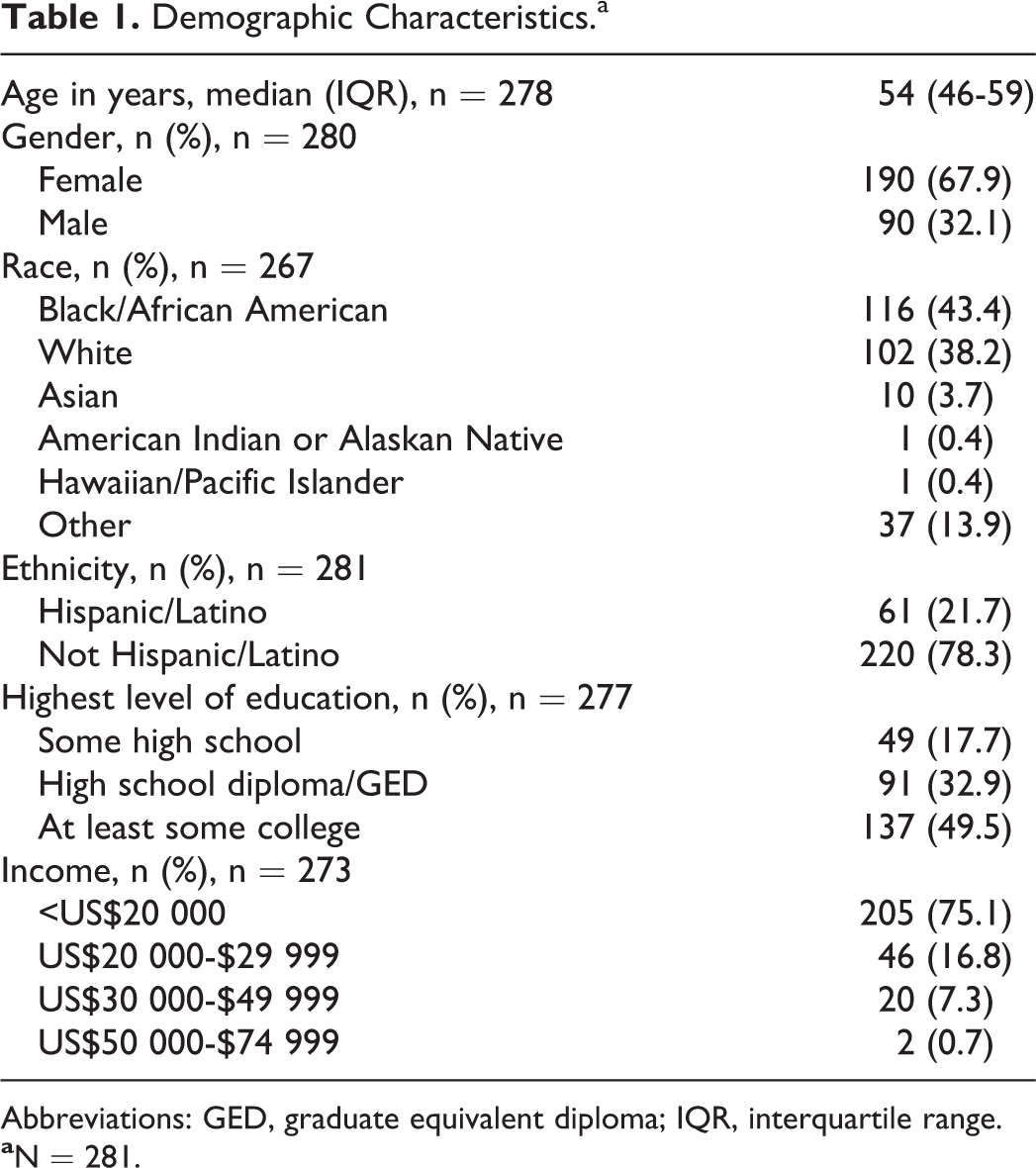
Abbreviations: GED, graduate equivalent diploma; IQR, interquartile range.
We first analyzed responses to the survey question, “What would convince you to get tested for HIV?” Among the 116 participants who answered this question, the most popular response was “My doctor recommends I get tested,” with over half of the participants (57.8%, 67/116) selecting this response (see Table 2).
Participant Responses to the Question, “What Would Convince You to Get Tested for HIV?”a,b

aN = 116.
bParticipants could select more than one response.
Despite most participants reporting that a physician recommendation would convince them to get an HIV test, most also reported not having received that recommendation. Of the 278 participants who responded to the question “Has your doctor ever recommended that you be tested for HIV?,” 55.4% reported their physician had not recommended the HIV test, while 30.6% reported their physician had recommended the test, and 14.0% did not remember.
We then sought to analyze patient attitudes toward patient–physician communication about HIV testing and patient intentions to get tested for HIV. To this end, we focused our remaining analyses on the 2 questions, “Do you want your doctor at this clinic to offer you an HIV test?” and “How likely would you be to accept an HIV test if your doctor recommended it?” There were 266 participants who answered both of these questions. Of these participants, 65.8% (n = 175) reported that they wanted their physician to offer them an HIV test. Whites (60%, 57/95) were significantly less likely than blacks (74.8%, 83/111) to report wanting their physician to offer the HIV test (P = .023). For those who reported a race other than black or white, 63.3% (31 of 49) reported wanting their physician to offer the HIV test. Patients who were Hispanic/Latino (54.2%, 32/59) were significantly less likely than patients who were not Hispanic/Latino (69.1%, 143/207) to report wanting their physician to offer the HIV test (P = .034). There was no statistically significant difference by gender in wanting to be offered the HIV test. We also evaluated whether a physician’s recommendation would impact the likelihood of patient HIV test acceptance. Of these same 266 participants, 84.6% (n = 225) reported they would “likely” or “very likely” accept the HIV test if they received a physician’s recommendation. There were no statistically significant differences by race, gender, or ethnicity in the likelihood of accepting the HIV test if a physician recommended it (data not shown).
We then examined whether a physician’s recommendation could convince patients to accept the HIV test whether or not patients wanted their physician to offer them the HIV test. Of the 175 participants who reported wanting their physician to offer the HIV test, 97.7% (n = 171) reported they would be “likely” or “very likely” to accept an HIV test if their physician recommended it (see Figure 1). Notably, of the 91 patients who did not want their physician to offer an HIV test, over half (n = 54, 59.3%) reported they would be “likely” or “very likely” to accept an HIV test if their physician recommended it (see Figure 1). Finally, we reviewed any demographic differences in likelihood of accepting the HIV test among patients who did not want it to be offered. Among those patients who did not want to be offered an HIV test and who responded to the survey question on race (n = 84/91), whites (73.7%, 28/38) were significantly more likely than blacks (50.0%, 14 of 28) to report they would “likely” or “very likely” accept the test if their physician recommended it3 (P = .048). For those who did not want to be offered the HIV test and reported a race other than black or white, 50% (9 of 18) reported they would “likely” or “very likely” accept the test if their physician recommended it. There were no statistically significant differences by gender or ethnicity in the likelihood of test acceptance among patients who did not want to be offered the HIV test.

Patient desire to be offered the HIV test and likelihood of HIV test acceptance.
Discussion
Our study of a predominantly racial and ethnic minority low-income patient population highlights the fact that a physician recommendation for HIV testing is important in convincing patients to get the HIV test. Despite the significant impact a physician recommendation has on HIV testing behavior, our study found that HIV testing is not being routinely offered by primary care physicians. Importantly, this is the first study to our knowledge that examined and found that even patients who do not “want” the HIV test are likely to accept testing if their primary care physician recommends it.
In our study, a physician recommendation was the top reason patients reported they would be convinced to accept the HIV test. Previous studies have found that a physician’s recommendation for HIV testing impacts patients’ HIV testing behaviors. In a national survey, over one-third of people who had been tested for HIV reported their reason for testing was a physician had suggested it. 8 Furthermore, over one-third of people who had not been tested said their reason was their physician had never recommended the HIV test. 8 In a large study of New York City residents, those who received a physician’s recommendation for HIV testing were 10 times more likely to have been tested than those who did not receive this recommendation. 9 In a survey of African American men—a population disproportionately affected by the US HIV epidemic 18 —the strongest predictor of having been tested for HIV was receiving a physician’s recommendation. 10
Despite national HIV testing recommendations and the impact a physician recommendation for HIV testing can have on testing behavior, physicians are not routinely offering their patients the HIV test, 11 even in high HIV prevalence cities. Our present study in Houston found that the majority of patients had never received a physician’s recommendation for an HIV test. A New York City study showed that only 35.8% of internal medicine residents routinely test their patients for HIV. 12 Another study revealed that only 20.3% of San Francisco medical providers routinely offered all patients an HIV test. 13 Additionally, in our own study of Houston primary care providers, 32.0% reported not routinely testing their patients for HIV. 14
One barrier to physicians offering patients the HIV test is perceived patient discomfort with or reluctance to discuss HIV. 15,19 In a 2011 study of general internists, 63.9% reported perceived patient reluctance or refusal as a barrier to HIV testing. 15 In our own 2014 study of primary care physicians in a large publically funded health-care system, 35.4% of physicians thought their patients would be uncomfortable discussing HIV and 16.6% thought their patients would be offended if offered the HIV test. 14 However, a study by McAfee et al found that 52% of emergency department patients wanted an HIV test. 20 Similarly, our present study done in the primary care setting revealed that most patients want their physician to offer them an HIV test. Moreover, we found that not only do most patients want their physician to offer HIV testing, but even patients who do not want their physician to offer it are still likely to accept an HIV test if their physician recommends it.
While all patients overall wanted their physician to offer the HIV test and were likely to accept the test if offered, there were some differences by race and ethnicity in the degree of these findings. Our study found that black patients were more likely than white patients to report wanting their physician to offer the HIV test. This may be because racial and ethnic minorities are harder hit by the HIV epidemic in the United States and are more likely to report that HIV is a problem in their community. 20 -22 It is unfortunate that Hispanic patients in our study were less likely to want the HIV test, given that they are also disproportionately affected by the HIV epidemic. 21 However, among patients who did not want to be offered the HIV test, there was no difference between Hispanics and non-Hispanics in likelihood of accepting the HIV test. Among patients who did not want to be offered the HIV test, whites were most likely to report a willingness to accept the test if it were recommended. Notably, white patients are the racial group least likely to be tested for HIV, 4 possibly because they are the racial group least likely to receive a physician’s recommendation for testing. 22 Although national data show that whites are less likely than racial and ethnic minorities to be HIV tested, 4 these latter minority groups are also disproportionately impacted by HIV and should be tested more routinely. 18,21 Therefore, encouraging physicians to continue to focus on offering the test to these minority groups remains critical. Finally, the majority of patients in this study had an income below US$20 000 and was receptive to HIV testing. Given that patients with low income are disproportionately impacted by HIV 23 and less likely to have access to consistent medical care and preventive health services, 23 it is especially important for physicians to capitalize on this opportunity to offer the HIV test while such patients are in their care.
Despite studies which show that physicians do not offer the HIV test because they believe that patients will refuse the test or be offended if offered, our study from the patient perspective refutes this belief. Our results align with the findings by Street and Haidet that physicians are not good judges of what their patients value. 24 Based on our findings, physicians should not allow their own perceptions of supposed patient discomfort or reluctance to be a barrier to offering routine HIV testing in adherence with the CDC and USPSTF recommendations. Our results show that not only are negative attitudes about HIV testing among patients uncommon but that a physician’s recommendation may be able to convince patients to be tested for HIV in spite of patients stating that they do not want the test. Now that the USPSTF has given a grade A recommendation for routine HIV testing of all adults, 3 campaigns are needed to encourage physicians to initiate HIV testing discussions with their patients. According to a review by Street, campaigns for physicians may need to involve multiple methods such as role-playing, feedback, and practice. 25 Campaigns could inform physicians of the latest HIV testing recommendations and display patients’ comfort with the discussion and willingness to accept HIV testing. These interventions may be particularly useful in health-care settings serving predominantly racial and ethnic minority patient populations, given that physicians have poorer communication with patients of these populations. 26 This discordant communication between physicians and patients of racial and ethnic minorities may partly explain why these patients are more likely to be diagnosed with HIV late—near the onset of AIDS. 27
The importance of physician recommendations is seen in other preventive health interventions as well. A 2001 study found that a physician’s recommendation for immunization was significantly associated with the tetanus, influenza, and pneumococcal vaccination statuses of Swiss adults. 28 In a 2003 study of African Americans, respondents were significantly more likely to have received colorectal cancer screening tests if they had previously received a physician’s recommendation. 29 In addition, a 2011 study of women aged 19 to 26 found that patients who received a strong physician recommendation for the human papillomavirus vaccine were 4 times as likely to be vaccinated as patients who received a recommendation that was not strong. 30
This study is subject to several limitations. The study was conducted at a single site in a publically funded health-care system. Therefore, these results may not be representative of patient attitudes in other health-care settings. However, this site is in an area with a high rate of HIV diagnoses and thus may have important implications for patient willingness to be HIV tested and for patient–physician interactions about HIV testing in areas with similar HIV prevalence. Because this was a convenience sample for a survey about HIV testing, it is possible that those who chose not to complete the survey differ in their attitudes toward HIV testing or the physician’s role in HIV testing. This study only included patients who completed the survey in English. It is possible that participants who did not complete the English language survey may differ in their desire to receive a physician HIV testing recommendation. Because native Spanish speakers may have a language barrier with their physicians, this may negatively impact the HIV testing discussion, thereby widening the gap we found between Hispanics’ and non-Hispanics’ attitudes toward physician HIV testing recommendations. Despite these limitations, to our knowledge, this is the first study in a primary care clinic in a high HIV prevalence area to find that even if patients do not want their physician to offer the HIV test, they are likely to accept the test if offered.
Given the ongoing HIV epidemic in the United States—and that over 50% of US adults still have not been HIV tested, 4 despite now long-standing recommendations for the HIV test 2,3 —new paradigms are needed to improve HIV testing. One important intervention remains integrating HIV testing in the daily practice flow in clinical settings as recommended in the 2015 National HIV/AIDS Strategy (NHAS). 31 As specifically highlighted in the NHAS, efforts are needed to ensure that physicians are following the USPSTF recommendations on HIV screening. 31 As it stands now, numerous studies have found that physicians are not routinely offering HIV testing, even when these physicians are caring for high-risk patient populations. 32,33 While much attention has been paid to the development of patient- and general public-focused HIV testing campaigns, there has been a dearth of work on developing physician campaigns for the health-care setting. Our work demonstrates the important role physicians play in increasing HIV testing in health-care settings, and this should be a key theme in physician-targeted campaigns, given the critical role primary care physicians can play to help us move closer to the US Healthy People 2020 objective to “increase the proportion of adolescents and adults who have ever been tested for HIV.” 34
Footnotes
Authors’ Note
The views expressed in this article are those of the author(s) and do not necessarily represent the views of the National Institutes of Health or the Department of Veterans Affairs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number K23MH094235 (PI: Arya). This work was also supported in part by the Center for Innovations in Quality, Effectiveness and Safety (#CIN 13-413) in Houston, Texas.