
Abstract
Research has demonstrated that adherence to antiretroviral therapy (ART) results in lower rates of morbidity and mortality associated with HIV infection, yet adherence remains a challenge in resource-limited settings like the Dominican Republic. Clínica de Familia La Romana addressed this problem with an education-based adherence program for adult patients new to ART, and this retrospective cohort study aimed to evaluate the impact of this intervention. Appointment adherence and biological markers were assessed in cases and controls through 12 months. A total of 101 participants were included, with 61 controls and 40 cases. The baseline CD4 count was 162 and 157 cells/mm3 in controls and cases, respectively. Cases showed a 15-fold increase in CD4 count compared with a 2.5-fold increase in controls. Cases were more likely to adhere to appointments with adherence rates of 86% versus 76% in controls. There was no difference between the rates of treatment abandonment, transfer of care, or death.
Background
The prevalence of HIV among adults in the Caribbean is approximately 1.0%, 1 making it the most affected geographical region outside sub-Saharan Africa. Together, populations in the Dominican Republic (DR) and Haiti make up almost 75% of all HIV infections in the Caribbean. 1 Government-initiated national provision of antiretroviral therapy (ART) started in 2004, with distribution guidelines based on the most recent World Health Organization (WHO) recommendations. 2 As of August 2012, more than 20 000 persons living with HIV/AIDS in the DR were receiving ART, representing coverage of 80% of the population with CD4 count less than 350 cells/mm3. 3
The impact of adherence to ART has been well studied, demonstrating both a reduction in HIV-1 viral load and lower rates of resistance as well as lower rates of morbidity and mortality associated with HIV disease. 4 –7 Adherence evaluation allows researchers to assess the factors that may predict poor outcomes. Additionally, because suboptimal adherence may result in resistance, evaluating adherence is particularly important in resource-limited settings where second-line medication options are limited. 8
Adherence research has traditionally been focused on sub-Saharan Africa and North America. It has been noted that in Western countries, predictors of nonadherence include depression, 9 substance abuse, 10,11 social instability, 12 and low literacy. 13 In resource-poor settings in sub-Saharan Africa, adherence is more closely tied to transportation access 14 and competing necessities, including food and housing. 15 –17 By contrast, there is a paucity of research on the barriers to adherence in Caribbean nations, despite being among the most affected geographic regions.
In response to this data and the need for outcome measures, a new adherence program was implemented at the Clínica de Familia La Romana (CFLR), a nongovernmental organization that serves as a regional referral center for HIV care. The intervention was implemented in August 2011, with a planned evaluation 1 year after its inception.
The objective of this study was to assess program efficacy by evaluation of factors such as appointment adherence in both the nonintervention and intervention groups and to determine whether adherence counseling had an impact on the biologic and clinical outcomes for the participants.
Participants and Methods
Study Design and Participants
The new adherence program consisted of one-on-one counseling that targeted patients beginning ART for the first time. Enrolled participants received 2 adherence counseling visits prior to starting ART. In structured counseling interventions, the counselor discussed predetermined themes pertaining to adherence, including (1) education on HIV/AIDS, resistance, and therapeutic failure; (2) evaluation of family support; and (3) identification of barriers to adherence, with strategies to overcome these barriers. The counselor also attempted to pair each participant with an adherence “buddy,” a family member or close friend who could accompany the participant to appointments and offer support. Subsequent clinic visits consisted of both medical evaluation and counseling sessions.
A retrospective cohort study was designed to evaluate the adherence program at CFLR. Participants ≥ 18 years of age who initiated ART between May and October 2011 (at least 12 months prior to study entry) were included in this study. Participants who initiated treatment between May and mid-August 2011 did not participate in adherence counseling and were therefore identified as controls. All participants who initiated treatment between mid-August and end-October 2011 did participate in adherence counseling and were therefore identified as the cases.
Exclusion criteria included participant age < 18 years, previous exposure to ART for >2 weeks, and crossover from nonintervention to intervention group. Participants were excluded as cases if they started the adherence counseling more than 2 weeks after the initiation of ART or if there was a lack of documentation.
Data regarding participant demographics (age, sex, nationality, employment, education, etc), biological markers of the disease (CD4 count, viral load), adherence effects (appointment adherence, abandonment of treatment, transfer of care), and mortality were collected at baseline and monthly for 12 months.
The study was approved by the Columbia University Institutional Review Board and the Dominican National Council on Bioethics in Health (Consejo Nacional de Bioética en Salud [CONABIOS]).
Effect Measures and Definitions
Adherence to visits
The end point measured was adherence to clinic appointments rather than adherence to medications. Appointment adherence was operationalized based on 3 calculations: appointments attended out of the number scheduled, average number of days late, and average number of missed visits.
Appointments attended out of the number scheduled was used rather than the absolute number of appointments kept to account for individual variations in the number of scheduled appointments (eg, participants from more distant provinces had fewer appointments), based on the methodology of Catz et al. 18
Number of days late was defined as the number of days after which the participant arrived to the scheduled appointment.
A missed visit was defined as a clinic appointment with a physician in the outpatient setting in which the participant was a no-show and did not send a surrogate to collect medications or in which the participant came late to the clinic by 4 or more days in the first month of weekly visits or by 15 or more days in subsequent months of monthly visits. Time periods were selected to maintain unique dates for each visit but also to allow for flexibility, given the travel constraints for participants.
Clinical visits and visits to the pharmacy (by participant or surrogate) to collect medications were combined to provide the overall adherence rather than adherence specific to clinical interactions.
Other outcomes included percentage of treatment abandonment and transfer of care to another center within 12 months of the start of treatment.
Clinical effects
The CD4 count (cells/mm3) at ART initiation, CD4 count at 6 to 12 months, and percentage of participants with a viral load and/or CD4 count at ART initiation were abstracted from the medical records of the participants. Percentage of death within 12 months after the start of treatment was also assessed.
Statistical Analysis
The analysis was performed using SAS 9.3 Software and Microsoft Excel 14.2.3. Qualitative variables were compared by chi-square tests. The significance threshold was .05.
Results
Between May 1 and October 31, 2011, a total of 132 treatment-naive adult participants were started on ART. Of these participants, 61 were included as controls (with no counseling) and 40 were included as cases (with counseling). The average age of the participants was 40.6 years. Approximately half of the participants were male, and a vast majority of the participants were Dominican.
Participant Characteristics
As shown in Table 1, participants in both groups were comparable. Eighty-nine percent of participants had a CD4 count measured within 3 months of starting therapy. At the time of initiation, the mean CD4 count was 162 and 157 cells/mm3 in the controls and cases, respectively. Notably, 18% of the controls and 29% of the cases had an initial CD4 count <50 cells/mm3. Less than half of participants had an initial viral load recorded.
Baseline Characteristics.
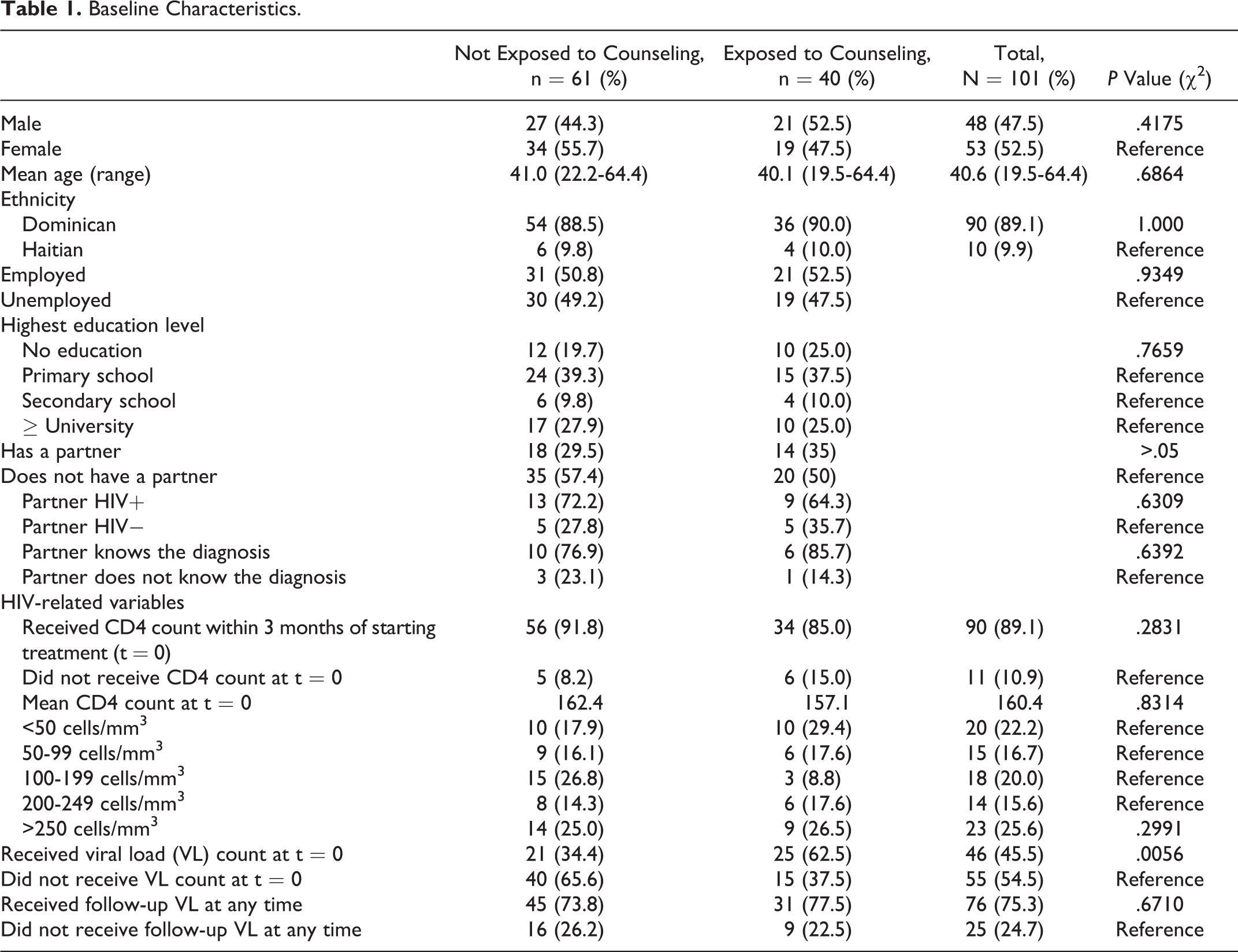
In all, 18 participants (30%) of the controls and 14 participants (35%) of the cases were recorded as having a sexual partner. Of these participants, the majority reported that the partner was also HIV infected and that the partner was aware of the patient’s HIV status.
The participants who underwent adherence counseling had initial data collected regarding family support and barriers to adherence. Of the cases, 83% perceived family support and 68% had an adherence buddy to accompany them to appointments. Eighty percent of participants identified at least 1 barrier to adherence. Significant barriers to adherence included transportation (47%), work schedule (38%), lack of money (20%), nausea and vomiting (20%), and fear of rejection (20%).
Effects of Exposure to Adherence Counseling
Adherence effects
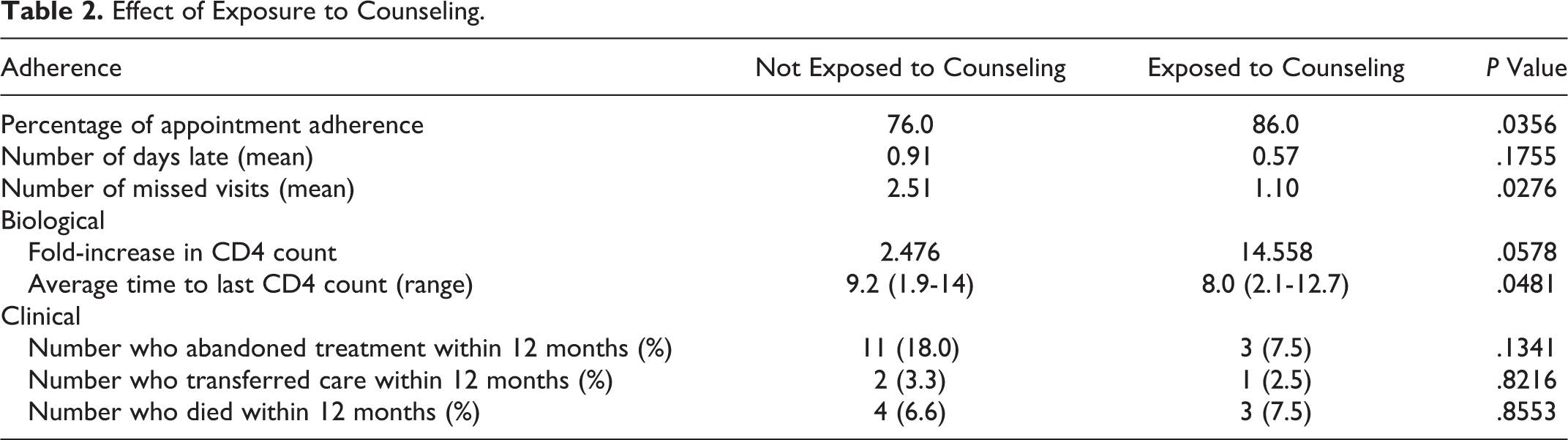
A total of 101 participants were included in efficacy analysis (Table 2). Cases were more likely to adhere to scheduled appointments with adherence rates of 86% versus 76% of controls (P = .035). The average number of missed visits in the cases versus controls was 1.10 and 2.51 per year, respectively (P = .028). There was no difference in days late for appointments.
Effect of Exposure to Counseling.
Biological and clinical effects
During the study period, the average time available for CD4 assessment was 8.0 months (range 2.1-12.7 months) in the cases and 9.2 months (range 1.9-14 months) in the controls. Cases showed a 15-fold increase in CD4 count, while controls showed a 2.5-fold increase in CD4 count (P = .0578) over the study period. Cases were more likely to have an initial viral load recorded (63% in cases versus 34% in controls; P = .01). However, change in viral load was not assessed, as only less than half of the total participants had an initial viral load recorded.
There was no significant difference between the rates of treatment abandonment (7.5% in cases versus 18% in controls; P = .13). All cases who abandoned treatment (n = 3) re-entered care within 12 months, whereas only 3 of the 14 controls who abandoned re-entered care. There was no difference between the cases and controls in the rates of transfer of care, death, or alive/on treatment at 12 months.
Discussion
This is one of few published studies evaluating education-based adherence interventions in the DR. In this study, it was shown that participants who participated in an education-based adherence counseling program had improved rates of appointment adherence when compared to participants who did not participate in the intervention. This improvement in appointment adherence was associated with a trend toward increase in CD4 count in the first year on ART.
Long-term outcomes (eg, treatment abandonment, transfer of care, death) did not show statistically significant changes within 1 year, but quantitative assessments showed trends toward fewer missed visits, fewer days late, decreased rates of treatment abandonment over 12 months, and increased rates of patients alive and on treatment at CFLR after 12 months (Table 2).
These positive results have significant implications, as education-based counseling interventions are applicable in other resource-poor regions. Indeed, prior attempts at adherence counseling interventions in developing regions have shown similar results. Khachani et al and Abah et al have shown improved adherence and understanding of HIV/AIDS and ART in both Morocco and Nigeria, as a result of education-based interventions. 19,20
Our study demonstrated novel barriers to adherence in developing countries. Our study highlights transportation and work schedule conflicts as important factors, despite the previous focus on substance abuse and lack of money. 21
Despite its important implications, this study has limitations. This study has a nonrandomized, retrospective design that can generate channeling biased results. This is a single-center study with a small sample size, thus limiting its power and generalizability to other populations. Although appointment adherence is an established strategy for quantifying treatment adherence, it is an indirect measure when compared to pill counts or medication event monitoring systems. Finally, the end point for biological effects did not match the study end point due to poor follow-up.
Turning to the global implications of this work, data collection at this site highlighted the clinic’s successes and challenges in meeting the WHO standards of care for HIV-infected patients in resource-poor settings. Most patients at CFLR began treatment at CD4 count less than the threshold at treatment initiation set forth by WHO guidelines. Reasons for this include late presentation to care and failure to follow up after a low CD4 count was reported. The clinic has made continued efforts to expand regular testing in the bateyes, sugar worker villages with a high prevalence of HIV, in order to expedite the identification of the disease and presentation to care for treatment.
The CFLR’s appointment frequency for patients new to ART is currently aligned with WHO recommendations 22,23 and the Dominican Ministry of Health Guidelines, and the clinic is approaching the goal for CD4 count every 6 months. Regular viral load testing remains a challenge because the samples must be sent to the Ministry of Health National Laboratory for processing.
Conclusion
This study brings additional evidence to support the positive impact of education-based adherence interventions for HIV-infected patients new to ART in resource-limited settings.
Through comprehensive adherence counseling that integrated educational and social support, the program led to improved appointment adherence in the intervention group, with associated trends in improvement in biological markers. The intervention also addressed barriers to adherence to aid in the provision of targeted solutions. Future steps in this area will require continued observation to assess long-term effects of such interventions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.