
Abstract
Background/Aims:
Distal symmetrical peripheral neuropathy (DSPN) and sleep disturbances are among the most common complications reported in people living with the human immunodeficiency virus infection and acquired immunodeficiency syndrome (PLWHA). DSPN-pain is predominantly managed by using systemic agents with little evidence supporting their analgesic efficacy. The purpose of this study is to evaluate the effect of nighttime lower extremity splinting application on DSPN-related pain and sleep disturbances compared to a parallel splint liner application in PLWHA.
Methods:
Forty-six PLWHA and DSPN were randomized to nighttime wearing of bilateral lower extremity splints or the liners only. Pain and sleep outcomes were measured at baseline, week 3, and week 6. The pain was measured using the Neuropathic Pain Scale and sleep using the Pittsburgh Sleep Quality Index.
Results:
Pain and sleep scores improved in both groups over time. The median percentage pain reduction at week 6 was 8% in the liner group and 34% in the splint group. The change in pain scores in the splint group was found to be significant over time, P < .0005. The contrast between the splint and liner groups was underpowered (26%) and was not found to be significant, P > .05. Sleep scores improved 20% from baseline to the end of the study in both groups; all participants were classified as poor sleepers.
Conclusion:
The 6-week use of nighttime splints reduces DSPN-pain possibly by providing peripheral inhibition of external stimuli. Future studies are needed to validate this inhibitory intervention to manage DSPN in PLWHA and other neuropathic conditions.
Introduction
Distal sensory peripheral neuropathy (DSPN) is among the most common complications associated with long-term survival with HIV infection and AIDS. HIV-related DSPN has been reported in 30% to 60% of all people living with HIV and AIDS (PLWHA). 1 –4 Distal sensory peripheral neuropathy in PLWHA appears to be mediated by HIV glycoprotein 120 exposure to the neuraxis, leading to chemokine production. The inflammatory-mediated peripheral nerve damage leads to cell death in the dorsal root ganglia, neurite damage, retraction at the periphery, astrocytosis in the spinal cord, and sensitization at the central processing centers. 5,6 Neuropathic pain is predominantly managed by using antidepressants, calcium channel α2-δ ligands, topical agents, and opioid analogs. 7,8 The direct analgesic effect attributed to topical agents, such as topical lidocaine application, demonstrates the presence of peripheral pain-generating mechanisms. 8 –10 None of the aforementioned systemic agents have demonstrated superior analgesic effects to placebo interventions in HIV-related DSPN. 7
In addition to pain, sleep disturbances have been reported in people living with end-stage renal disease–related neuropathies and HIV-related DSPN. 11,12 A review of systemic diseases’ impact on sleep suggests that alterations in sleep stages and increases in sleep disturbances are associated with HIV disease progression into AIDS. 13 The impact of DSPN-related pain on self-perceived sleep quality remains uncertain based on the limited number of reports in the literature.
In a recent pilot study, 12 the use of nighttime lower extremity (LE) splints showed promising results in the management of pain and sleep disturbances. This pilot study was a crossover study design that included 22 PLWHA and DSPN. A 20% improvement in both pain and sleep scores were reported at the end of this trial with a moderate effect size for pain and sleep scores. The pilot study could not determine whether the analgesic effect was due to the application of a full contact protective sheath on the lower leg or the short-term immobilization at the ankle joints provided by the splints. The purpose of this study was to evaluate the impact of wearing bilateral LE splints compared to a parallel intervention of wearing bilateral LE splint liners only on pain and sleep disturbances in PLWHA and DSPN.
Methods
Inclusion/Exclusion Criteria
Adult PLWHA from an outpatient public clinic with a clinical diagnosis of symptomatic DSPN were recruited to participate in this study. The eligible participants reported at least one of the following clinical symptoms: paresthesia, dysesthesia, or night cramps in the lower legs. Participants were excluded if they were pregnant, had a concurrent diagnosis of cardiovascular or pulmonary disease, paraplegia, hemiplegia, diabetes, or sleep apnea.
Intervention Equipment
Walkabout splints (Don Joy Orthopedics, Vista, California) were used in the splint group. The Walkabout splint is composed of a soft liner coupled to a 90° rigid plastic exoskeleton to immobilize the foot and ankle. The liners from the Walkabout splints were fitted to the participants in the liner group.
Dependent Outcome Measures
Pain Measure
A composite pain score was collected using the self-reported Neuropathic Pain Scale (NPS). 14 In this 0 to 100 scale, the participants were asked to quantify the different aspects of the pain experience in the presence of neuropathies. Galer and Jensen 14 reported that the NPS exhibits both predictive and discriminant validity as well as being sensitive to the effect of treatments impacting neuropathic pain.
Sleep Quality and Quantity
The Pittsburgh Sleep Quality Index (PSQI) is a 10-item questionnaire covering the following 7 components of sleep: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunctions. 15 Each of the 7 subscales has a maximum score of 3; a high score on the PSQI indicates poor sleep quality. Buysse et al 15 reported sensitivity, specificity, and κ agreement values of 89.6%, 86.5%, and 0.75, respectively, for this sleep scale in identifying poor sleepers (global PSQI score >5/21).
Procedures
All qualifying participants signed a consent form approved by the Harris Health System and Texas Woman’s University institutional review boards. Baseline demographics and HIV disease markers were collected to describe the participants in this study. The participants completed the NPS and the PSQI questionnaires. After baseline completion of questionnaires, the participants were randomly assigned to either the complete splints or the liners-only group using a precoded allocation table. The researcher individually fits all participants with either bilateral splints or bilateral splint liners according to their group assignment. Both groups received the same instruction to wear their devices at night while sleeping. The participants were asked to return at week 3 and week 6 from baseline to complete the NPS and PSQI questionnaires. All participants were contacted weekly by telephone to record compliance with the protocol procedures and to document issues concerning the wearing of the splints or liners.
Data Analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 16.0 (IBM, Armonk, New York). Descriptive statistics were computed on all variables. To evaluate group equivalence at baseline, all descriptive and outcome data were analyzed for extreme variables using histograms, scatterplots, and residual analysis. The baseline data were compared using contrast to test for independence. The following null hypotheses were tested: (1) there is no difference in pain scores between individuals wearing bilateral LE splints and those using the splint liners only, following a 3-week and 6-week nighttime use protocol, (2) there is no difference in sleep scores between individuals wearing bilateral LE splints and those wearing splint liners only following 3 and 6 weeks of nighttime use, and (3) there is no difference in pain scores between baseline scores and following a 6-week nighttime LE splints use protocol to manage DSPN-related pain.
The null hypotheses were tested using 2 separate 3 × 2 repeated measures analysis of variance (ANOVA) for the dependent variables of pain and sleep scores with time (3 levels) by group (2 levels). A Kruskal-Wallis ANOVA was utilized for the sleep scores.
Each of the above-mentioned ANOVAs was followed by planned contrasts of interest. The between-group contrasts compared pain and sleep score differences at week 3 and week 6 and a single additional within-group contrast of interest in the splint group from baseline to week 6. The level of significance was split, with α set at .04 for the pain score analyses and α set at .01 for the sleep scores. Each pain score contrast of interest was tested using an adjusted level of significance to maximize power for these contrasts, as the NPS is sensitive to detect changes in self-reported pain following analgesic interventions, α < .013 (or .04/3). The sleep score contrast was tested at an adjusted level of significance of α < .005 (or .01/2). Finally, an intention-to-treat analysis was conducted on the outcome variables to mitigate the attrition rate impact on the data collected. For the participants who discontinued the trial at baseline, the baseline scores were transposed for week 3 and week 6. For those participants missing follow-up visit data, the average outcome variable scores for their available data were used to impute the missing information.
Results
Participants
Data were collected from 46-community dwelling PLWHA. The participants were equally randomized to either the splint (23 of 46) or the liner (23 of 46) groups. One participant in the liner group failed to disclose a recent type 2 diabetes diagnosis and was excluded from the study, with none of the data used in the analyses. Thus, 45 participants began the study, 23 in the splint group and 22 in the liner group. The study attrition and the number of patients kept for final analysis are illustrated in the CONSORT diagram (Figure 1).

CONSORT diagram.
The overall attrition rate in the splint group was around 35%. In all, 3 (13%) participants discontinued participation within the first week of the study for personal reasons and 3 (13%) additional participants failed to return for all follow-up sessions. Two (9%) additional participants in the splint group had incomplete data, missing 1 follow-up session. Thus, complete data were collected on 16 (70%) of the 23 participants, and incomplete data on 2 (9%) additional participants by the end of the trial.
For those in the liner group, 1 (7%) participant failed to report for all follow-up sessions, 2 (9%) additional participants failed to report for the final follow-up session. Complete data were obtained for 19 (83%) of the 23 participants in the liner group and incomplete data for 2 additional participants. The data collected at week 3 and week 6 of the trial were used for the contrasts of interest comparing the pain and sleep outcomes between the intervention groups.
The majority of the participants were African American men in their fifth decade of life and had been living with HIV infection an average of 10.82 years. The most common antiretroviral therapy (ART) used by the participants was once daily formulation of emtricitabine/tenofovir (TDF)/efavirenz (EFV). In all, 40 (89%) of the 45 participants were on ART at the beginning of the trial, while 36 (90%) participants on ART were on a regimen containing at least 1 nucleoside reverse transcriptase inhibitor (NRTI) agent. Twenty-one (53%) participants on ART were on a regimen containing at least 1 protease inhibitor (PI) agent. Of the participants on ART, 18 (45%) were on a regimen containing at least 1 nonnucleoside reverse transcriptase inhibitor (NNRTI) agent; 1 (3%) participant was using an ART containing an integrase inhibitor but none of the participants on ART were on a regimen containing entry inhibitors. Undetectable HIV viral load levels (less than 48 copies/mL) were noted in 31 (69%) of the 45 participants. The average CD4 count was 518 cells/mm3 for all participants, while the median nadir CD4 was 215 cells/mm3. The participants used a combination of nonsteroidal anti-inflammatory drugs, antidepressants, calcium channel α2-δ ligands, and opioid analogs as primary agents to manage DSPN pain. In addition, other agents such as anticonvulsants and muscle relaxants were included alongside the other systemic agents to maximize pain relief. The most common analgesic agents used by this sample of participants were antidepressants (22 of 45) and calcium channel α2-δ ligands (28 of 45). The participants’ characteristics at baseline are reported in Table 1. The groups were equivalent for all baseline demographics and pharmacological regimens. Although not statistically significant, the participants in the splint group appeared to be slightly older, had prior exposure to neurotoxic ART regimens, and had slightly higher baseline CD4 counts than those randomized to the liner group.
Participant Characteristics.a

Abbreviations: ART, antiretroviral therapy; D4T, stuvadine; DDI, didanosine; ddC, zalcitabine; NSAID, nonsteroidal anti-inflammatory drug; NPS, Neuropathic Pain Scale; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation.
a N = 45.
b Independent Student t test.
c Mann-Whitney U test.
Of the 23 participants in the splint group, 16 (70%) reported discomfort with immobilization while using the splints during the first 2 weeks of the trial; however, these issues resolved by week 3 of the trial. No comfort-related issues were reported by any of the participants in the liner group. Of the 45 participants, 33 (73%) reported painful night calf cramps at the beginning of the study. Painful night cramps were reported in 17 (74%) of the 23 participants in the splint group and 16 (73%) of the 22 participants in the liner group at baseline assessment. Of the 17 participants in the splint group originally reporting night cramps, 14 returned for the final follow-up session; none of them reported painful cramps at the end of the study. Night calf cramps continued to be reported at the end of the trial in 14 (88%) of the 16 participants in the liner group that originally reported night cramps at baseline.
For the dependent variable pain, the splint group’s mean percentage pain score reduced 11.89% ± 23.23% from baseline to week 3, and 32.89% ± 23.23% from baseline to week 6. The average percentage pain reduction in the liner group was 10.12% ± 22.12% from baseline to week 3 and 14.52% ± 39.74% from baseline to week 6. The median pain reduction from baseline to week 6 was 34% and 8% in the splint and liner groups, respectively. In all, 11 (61%) of the 18 participants in the splint group and 5 (26%) of the 19 participants in the liner group reported at least 30% pain reduction from baseline at week 6 of this trial (Figure 2).

Percentage pain change from baseline to week 6. *indicates change in pain from baseline to week 6, P < .0005.
The sleep scores improved from baseline to week 6 in both groups (see Table 2). The change in sleep and pain scores at each follow-up interval is illustrated in Figures 3 and 4, with sleep scores normalized to 100. Of the 45 participants, 5 (11%) were using zolpidem to assist in optimizing sleep. In all, 2 (4%) of the 5 participants were randomized to the splint group, while the other 3 (7%) participants were assigned to the liner group. The average sleep score for these participants at baseline was similar to the rest of the participants in the study (14.40 ± 3.58).
Mean Pain and Sleep Scores.
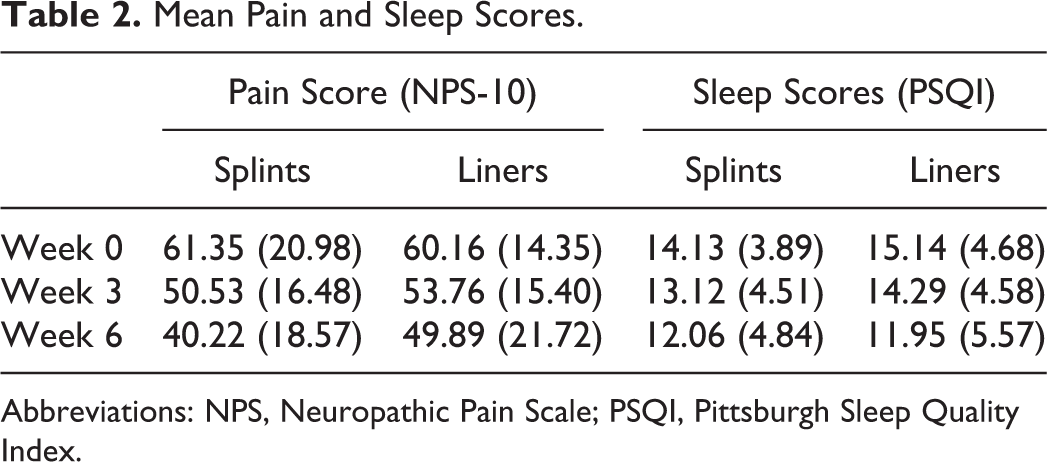
Abbreviations: NPS, Neuropathic Pain Scale; PSQI, Pittsburgh Sleep Quality Index.

Pain scores.
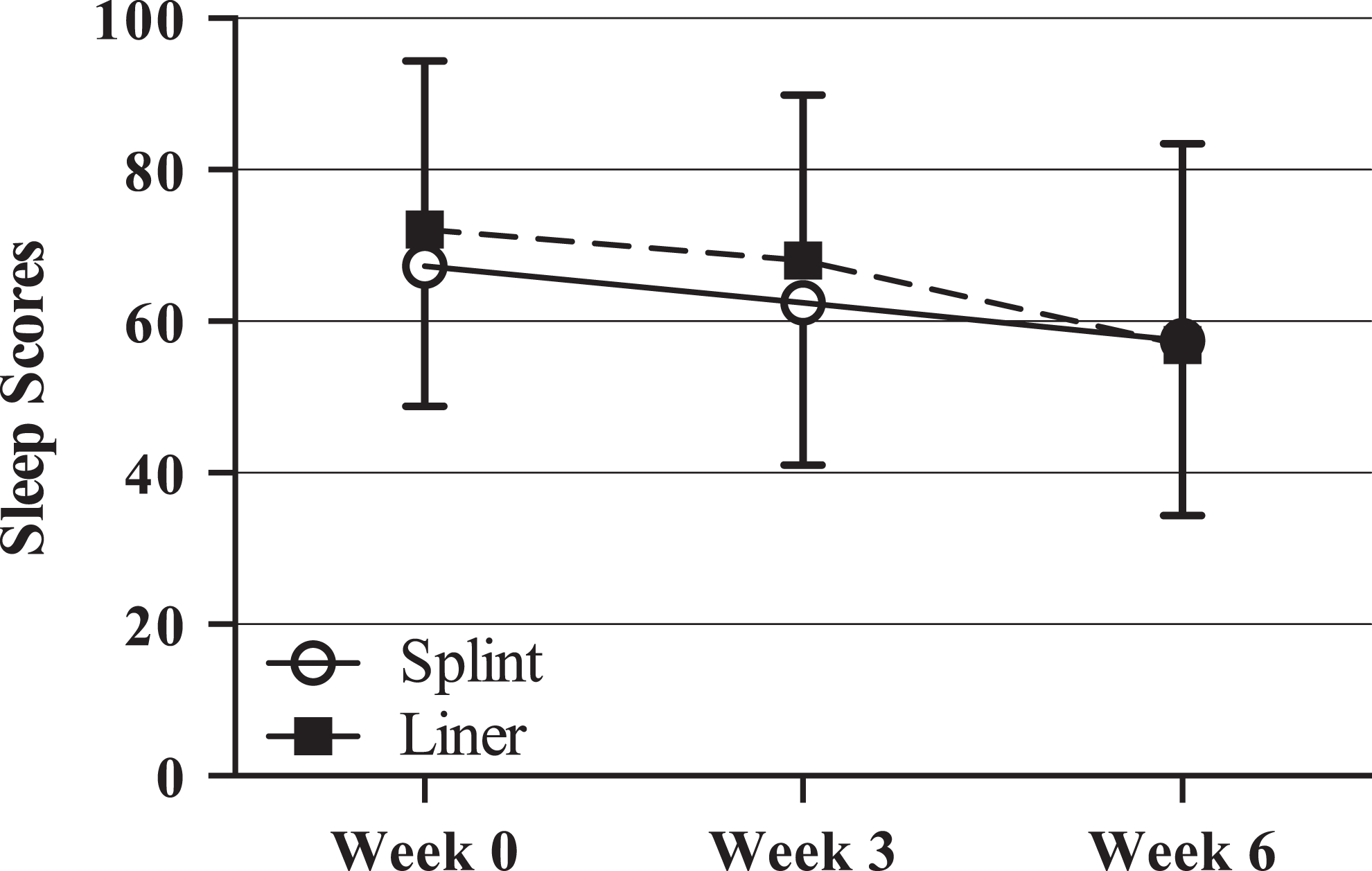
Sleep scores.
Pain Scores (Intention-to-Treat Analysis)
A repeated measures ANOVA was conducted to test the null hypothesis that there is no difference in pain scores between the intervention groups. To address the potential for missing data to affect the results, the analyses were repeated with the imputed data using the aforementioned approach to handle missing data. For the dependent variable pain, Mauchly test for sphericity demonstrated that the assumption of sphericity was not tenable for the factor pain scores, χ2(2) = 15.47, P < .0005, therefore degrees of freedom were corrected using Huynh-Feldt estimates of sphericity (∊ = 0.81). The repeated measures ANOVA was found to be significant, F1.61,69.26 = 15.38, P < .0005. No significant interaction was found between the factors time and group, F1.61, 69.26 = 0.781, P = .44. The main effect of time for the factor pain score was found to be significant, F1,43 = 19.77, η 2 = 0.32, P < .0005. No significant main effect was found for the group assignment on pain scores, F1,43 = .01, P = .935. The observed statistical power for the between-group analysis was .05 and .97 for the within-group analysis.
Per-Protocol Analysis
For the dependent variable pain, only the statistical power and effect size were found to be different between the intention-to-treat analysis (η 2 = 0.32, 5% statistical power for within group analysis) and the perprotocol analysis (η 2 = 0.36, 26% statistical power for within group analysis) conducted on the data retained. No overall changes in statistical significance were noted between these analyses for the omnibus repeated measures ANOVA, F1.71,56.46 = 14.07, P < .0005; the interaction between group allocation over time, F1.71,56.46 = 1.28, P = .282, or the main effect of time for the factor pain score was found to be significant, F1,33 = 9.01, P = .001.
Sleep Scores (Intention-to-Treat Analysis)
The same data extrapolation described for pain scores was used to impute the missing sleep scores. A Kruskal-Wallis ANOVA failed to reveal a significant between-group effect of group on sleep scores at week 3, χ2(2) = 0.797, P = .372, and week 6, χ2(2) = 0.002, P = .962, of this trial. A Friedman ANOVA revealed a significant effect over time on sleep scores, regardless of group assignment, χ2(2) = 16.66, P < .0005.
Per-Protocol Analysis
No significant differences were found between the intention-to-treat analysis and the data retained for final analysis for sleep scores. The Kruskal-Wallis ANOVA failed to reveal a significant effect between the groups on sleep scores at week 3, χ2(2) = 1.628, P = .202, and at week 6, χ2(2) = 0.109, P = .741, of this trial. A Friedman ANOVA revealed a significant reduction in sleep scores over time, which was independent of group assignment, χ2(2) = 12.32, P = .002.
This analysis suggests that there was a significant decrease in pain and sleep scores from baseline to week 3, baseline to week 6, and from week 3 to week 6, regardless of group assignment.
Contrasts of Interest
Independent student t tests were performed to test the null hypothesis that there is no difference in pain scores among the intervention groups at week 3 and week 6 of this trial. No significant mean difference was found for the contrast of interest at week 3 (−3.23/100 points, 95% confidence interval [CI] −13.93 to 7.47, t35 = −1.45, P = .155) or at week 6 (−9.67/100 points, 95% CI −23.20 to 3.85, t35 = −0.61, P = .544). The results of the paired student t test showed a statistically significant reduction in pain scores from baseline to week 6 of 21.11/100 points (95% CI 11.54-30.69) of this trial in the splint group, t17 = 4.65, P < .0005.
A Mann-Whitney U test failed to find a significant difference in sleep quality index scores between the groups at week 3 (−1.16/21 points, 95% CI −4.23 to 1.91, P = .39, r = .49) or at week 6 (0.11/21 points, 95% CI −3.44 to 3.67, P = .13, r = .54).
Discussion
The results of this trial support the use of LE splinting to manage HIV-related neuropathic pain, with a moderate effect size attributed to this intervention. None of the participants randomized to the splint group completing this trial reported painful night cramps at the end of this trial and reported a median percentage pain score reduction greater than 30% in the splint group compared to less than 10% in the liner group at the end of the study. As such, night splinting can be considered as an effective adjunct intervention to inhibit peripheral input in patients reporting painful night cramps. The results of this trial suggest that either the use of nighttime LE splints or splint liners reduces DSPN-related pain and improved the sleep quality in PLWHA The peripheral inhibition achieved by direct contact on the LE skin appears to have a positive effect on a hyperactive neuraxis, which in turn is preferentially conditioned to interpret innocuous stimuli as pain in PLWHA and DSPN. The results of this trial support a theory where multiple concurrent clinical phenotypes directly influenced by peripheral input may be present in HIV-related neuropathies.
Splinting devices have been used at the wrist to manage symptoms associated with carpal tunnel syndrome (CTS). Distal sensory peripheral neuropathy in PLWHA and people living with CTS share a similar clinical presentation that includes complaints of hypernociception, paresthesia, and allodynia. In a recent Cochrane database review, O’Connor et al 16 concluded that the use of a wrist brace at night or continuously improved symptoms of pain in people living with CTS. Many of the currently approved pharmacological agents to manage neuropathic pain have been approved for use with less than half of the participants reporting greater than 30% pain relief, while none have proven superior to placebo application in HIV-related DSPN. 7,17,18 The neuropathic pain management guidelines from the International Association for the Study of Pain suggest that a 30% pain reduction from baseline represents an effective analgesic treatment outcome. 7 In the current study, this level was achieved with the nighttime splinting program. The splinting program provides a nonpharmacological, cost-effective, patient-modulated option to manage disrupting neuropathic symptoms in PLWHA. The findings of the current study are congruent with those reported in a pilot study on the use of LE splints to manage pain in PLWHA and DSPN. 12 The authors reported a 20% reduction in pain and sleep scores following a 3-week nighttime use of LE splints. A moderate effect size was attributed to the splints for pain and sleep scores during that LE splints trial.
The analgesic effect and lack of painful night cramps in this trial may be attributed to the splints’ short-term immobilization effect. Wearing both the splint and the splint liner seems to have had an unanticipated positive influence on pain response, which might be due to nighttime immobilization and inhibition of sensory nerve endings. Huber et al 19 investigated the inhibitory effect of 12-hour immobilization of the hand on motor task coordination, somatosensory-evoked potentials (SEP), motor-evoked potentials, and sleep slow wave activity (SSWA). The authors attributed changes observed in motor coordination, SEP, and SSWA to inhibitory neuroplastic events resulting from the short-term sensory deprivation and immobilization of the upper extremity. Additionally, animal models suggest the presence of an analgesic effect associated with acute and intermittent immobilization. 20 –23 The body of evidence in these animal models suggests that immobilization alters endogenous endorphins, serotonin absorption, and acetylcholine activity in the hippocampus resulting in intrinsic pain modulation. 23
In the current study, all participants were classified as poor sleepers based on the PSQI scores at baseline and at each follow-up session. Sleep disturbances are commonly reported during chronic pain conditions including those associated with chronic neuropathic pain. 24 –26 Sleep disturbances are frequently reported in PLWHA, with more than 50% of these individuals reporting some level of sleep disturbances. 13,27 –29 Aouizerat et al 30 described higher General Sleep Disturbances Scale scores for those PLWHA reporting pain than for those not reporting pain. The authors concluded that sleep disturbances are both common and coexist with pain in PLWHA. 31 Finally, Galer et al 26 surveyed 105 people living with diabetes-related neuropathic pain in a descriptive correlation study and reported that 57% of the participants had substantial sleep disruptions directly attributed to neuropathic pain symptoms. Additionally, 52% of the participants in Galer’s study reported worsening of neuropathic pain symptoms at night.
In the current study, the participants exhibited 17% more sleep disturbances, at baseline, than people living with insomnia. 32 Self-reported sleep quality improved by the end of the trial in both treatment interventions. It is interesting to point out that only a small number of participants were using zolpidem to optimize sleep and that the sleep quality index scores in these individuals were similar to the rest of the participants. These findings support the presence of an association between the constructs of sleep and pain. The pain–sleep association has been reported as both a linear and circular relationship between these variables in people living with neuromuscular pain syndromes. 25,33 The linear model suggests a direct association between pain and sleep, where pain directly interferes with sleep. In this model, addressing the source of the pain directly improves sleep quality. The circular model postulates a summative and circular effect, where chronic pain contributes to poor sleep; while a state of chronic sleep deprivation potentiates pain integration. 25 Either model supports the net beneficial effect of effective pain management on sleep quantity and quality.
The current study was limited by its inability to confirm the DSPN diagnosis with more invasive clinical tests such as punch skin biopsies. Additionally, all of the participants were recruited at a public outpatient clinic where the demographic characteristics may differ from those PLWHA and DSPN followed in private practice settings. The relative high attrition rate observed during the data collection phase may have had an impact on the results obtained, as a number of participant’s data had to be imputed using very conservative estimates. People with recent HIV/AIDS diagnosis may not have been adequately represented. Finally, the primary investigator responsible for data collection and analysis was not blinded to the group allocation of the participants for any of the follow-up testing sessions. Additional studies are needed to evaluate the clinical relevance to a progressive splinting or immobilization intervention. Finally, studies are needed to evaluate the theory that the analgesic effect observed might be the result of central neuroplastic events modulated by peripheral sensory nerve ending inhibition and intermittent limb immobilization.
Footnotes
Acknowledgments
The authors would like to thank the Harris County Hospital District Foundation (Houston, Texas) and Don Joy Orthopedics (Vista, California) for their generous research support.
Authors’ Note
R. Sandoval designed the study, collected data, enrolled the patients, and analyzed the data in this study as part of his doctoral dissertation. T. Roddey (chair), T. Giordano, K. Mitchell, and C. Kelley were part of the dissertation committee overseeing this research, providing scientific guidance, and editing assistance to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project received financial support in the form of a research grant from the Harris County Hospital District Foundation (Houston, Texas). The authors received material support in the form of a donation of the splinting supplies from Don Joy Orthopedics (Vista, California).