
Abstract
Background:
Pain, sleep, and functional disturbances are a common occurrence in people living with HIV/AIDS-related distal sensory peripheral neuropathy (PLWHA-DSPN) yet lack group classification and quantification.
Methods:
A total of 46 PLWHA-DSPN were recruited, as part of a 2-group intervention study, to complete the Neuropathic Pain Scale and the Pittsburgh Sleep Quality Index (PSQI) questionnaires. The participant’s performance during a forward reach task and walking distance in 6 minutes was recorded as a measure of function.
Results:
The pain (60.77 ± 17.85) and sleep (14.62 ± 4.28) scores denote marked pain and sleep disturbances, compared to sero-negative, age-matched individuals. The ambulation distance was limited (243.99 ± 141.04 m) and inversely associated with the PSQI-sleep efficiency subscale (rs = −.35, P < .05). The average reaching distances measured (36.07 ± 7.37 cm) were similar to sero-negative, age-matched individuals. Pain, sleep, and functional measures exhibited significant associations.
Conclusions:
The data collected suggest that PLWHA-DSPN report moderate-to-severe pain and significant sleep disturbances and exhibit limited ambulation distances.
Introduction
Pain and sleep disturbances are commonly reported in people living with chronic systemic diseases such as fibromyalgia, arthritis, chronic liver disease, and HIV infection. 1 –3 Data collected from a cohort of 317 people living with HIV and AIDS (PLWHA) indicate that 55% of them experienced and ranked increases in pain and sleep disturbances among the top 4 symptoms associated with people living with HIV infection. 4 Pain and sleep disturbances were only preceded in prevalence by self-reports of fatigue and drowsiness in PLWHA. A review of systemic diseases’ impact on sleep suggests that increases in sleep disturbances are associated with HIV disease progression into AIDS. 5
Functional limitations have been reported in PLWHA compared to age-matched sero-negative individuals. Simmonds et al 6 reported approximately a 30% decrease in the 6-minute walk distance (6MWD) for PLWHA compared to age-matched sero-negative individuals. More importantly, the authors described a relationship between pain, 6MWD, and average forward reach (FR) distance that accounted for 26% of the variance in self-reported quality of life. Additionally, significant decreases in gait quality, walking speed, and 6MWD in individuals living with a diagnosis of peripheral neuropathy compared to age-matched control cohorts have been reported. 7,8
Distal sensory peripheral neuropathy (DSPN) is among the most common comorbidities associated with long-term survival people with HIV infection. Of all PLWHA, 30% to 60% may develop clinical symptoms of DSPN as the disease progresses into AIDS. 9 –12 Pain and paresthesia at the extremities, loss of vibratory sensation, and decreased deep tendon reflexes are the defining clinical symptoms for the diagnosis of DSPN. 13 The impact of pain manifestation in HIV-related DSPN on function and sleep disturbances is yet to be reported in this clinical cohort. The purpose of this study is to describe pain, function, and sleep disturbance characteristics and the strength of their respective relationship in PLWHA and DSPN.
Methods
Inclusion and Exclusion Criteria
Adult PLWHA from an outpatient public clinic associated with the Harris Health System (HHS) were recruited to participate in this study. This study was part of a 2-group design intervention study. All participants had a clinical diagnosis of symptomatic bilateral lower extremity DSPN. Only participants with a documented clinical diagnosis of DSPN in their medical charts were recruited to participate in this study. The participants were English speaking and on both stable pain and antiretroviral (ARV) regimens. Eligible participants reported at least 1 of the following clinical symptoms: paresthesia, dysesthesia, or night cramps in the lower legs. Participants were excluded if they had a concurrent clinical diagnosis of significant cardiovascular or pulmonary disease, paraplegia, hemiplegia, diabetes, sleep apnea, or were pregnant.
Pain Measure
A composite pain score was collected using the self-reported Neuropathic Pain Scale (NPS). On this 0 to 100 scale, the participant was asked to quantify the different aspects of the pain experience in the presence of neuropathies. Galer et al 14 reported that the NPS exhibits both predictive and discriminant validity as well as was sensitive to the effect of treatments impacting neuropathic pain. Galer et al 14 suggested that a NPS-10 score greater than 43 of 100 may indicate the presence of neuropathic conditions. The NPS may be scored in 4 different ways. It may be scored as a global score or “NPS-10” including all items in the scale. It can be scored as the NPS-8 selecting only the 8 pain descriptors present in neuropathies, excluding the global scores for pain intensity and unpleasantness. It can be scored as the NPS nonallodynic (NPS-NA) scale using the 8 items of the NPS but excluding “surface pain” and “skin sensitivity.” Finally, it can be scored as the NPS-4, which includes the score for “sharp pain,” “hot pain,” “dull pain,” and “deep pain.” 15 Galer et al 16 reported that the scores obtained with any of the NPS scoring options appear sensitive to detect treatment effects. All scoring options of the NPS and pain intensity were included in the analysis to evaluate their ability to capture the construct of neuropathic pain in PLWHA and DSPN.
Sleep Quality and Quantity
The Pittsburgh Sleep Quality Index 17 (PSQI) is a 10-item questionnaire that covers the following 7 components of sleep: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunctions. Each of the 7 subscales has a maximum score of 3, with a high score on the PSQI indicative of poor sleep quality. Buysse et al 17 reported sensitivity and specificity values of 89.6% and 86.5%, respectively, for this sleep scale in identifying good (PSQI score <5 of 21) and poor sleepers (PSQI score ≥5 of 21).
Functional Tests
Forward Reach Test
For the FR test, the investigator collecting data asked the participants to stand next to a wall without shoes, with their feet positioned hip width apart on the floor and with the self-selected shoulder not touching the adjacent wall-mounted yardstick. The starting point for each reaching attempt was identified along a yardstick affixed to the wall by locating the ulnar styloid process of the arm closest to the wall. The participant was instructed to “Please reach as far forward as possible.” The translated distance of the distal aspect of the styloid process was recorded as a reaching trial. The average distance of 3 reaching trials was recorded in centimeters.
Six-Minute Walk Distance
For this test, the participants were instructed as follows: “Please walk as far, as fast, and as safely as you can for up to 6 minutes.” The walking test was performed on a level surface void of obstacles and with a predetermined path of 10.36 m, 20.72 m per lap, requiring a 180° turn at each end. The single-trial 6MWD was recorded.
The 6MWD and the FR distance were collected using the same methods used by Simmonds et al. 6 Both the 6MWD and the FR tests have exhibited intersession intraclass correlation coefficient values greater than 0.83. 18 The minimal clinical important difference (MCID) for the 6MWD has been reported to be 54 m (95% confidence interval [CI] 37-71 m). 19 –21 The FR distance has been reported to have a MCID of 2 cm (95% CI 4-11 cm). 22,23 Finally, the 6MWD and FR, in conjunction with self-reported pain, have been reported to exert significant influence on the self-reported quality of life in PLWHA. 6
Procedures
All participants signed an informed consent form approved by the institutional review boards of HHS and Texas Woman’s University. Baseline demographics and HIV disease markers were collected to describe the participants in this study. The participants completed the NPS and PSQI questionnaires. The physical performance tests immediately followed the self-reported questionnaires completion.
Data Analysis
The data analysis was performed using the SPSS version 16.0 (IBM, Armonk, New York). Descriptive statistics were computed on all variables. A correlation matrix was developed and consisted of both Pearson (r) and Spearman (rs) correlation coefficients for parametric and nonparametric data, with an α level at .05 for significant associations set. For further analysis, all data collected were screened for extreme values. Histograms and scatter plots were obtained and analyzed for assumptions of normality. The analysis of extreme values was performed using a residual analysis on the data retained for final analysis.
Results
Participants
Informed consent was obtained from 46 community-dwelling PLWHA. Data were collected on 45 participants. One participant failed to disclose a recent diagnosis of type II diabetes and was excluded from the analysis. The majority of participants were African American males in their fifth decade of life, living with HIV infection for an average of 10.82 years. The most common ARV medication used by the participants was once daily, fixed-dose formulation of tenofovir (TDF)/emtricitabine/efavirenz (EFV). Of the 45 participants, 36 (80%) were on an ARV medications containing at least 1 nucleoside reverse transcriptase inhibitor (NRTI) agent; 21 (47%) of the participants were on an ARV medications containing at least 1 protease inhibitor agent; and 18 (40%) of the participants were on an ARV medications containing at least 1 non-NRTI agent. One (2%) participant was using an ARV medication containing an integrase inhibitor, but none of the participants’ ARV medications included entry inhibitors. Undetectable viral load levels (<48 copies/mL) were noted in 31 (69%) participants in this study. The participants’ characteristics for all dependent variables are reported in Table 1. A participant’s average FR distance was 63.07 cm, which was greater than 3 standard deviations distance from the mean distance reached by the rest of the participants. This participant’s contribution to the FR distances was excluded from further analysis. No extreme values were identified for pain, sleep, or walking endurance scores.
Participants Characteristics.

Abbreviations: D4T, stavudine; DDI, didanosine; ddC, zalcitabine; NA, nonallodynic; NPS, Neuropathic Pain Scale; PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation; 6MWD, 6-minute walk distance.
aNormalized to 100.
bAverage of 3 consecutive trials, n = 44.
The average score for all PSQI subscales are represented in Figure 1. The average pain intensity and pain scores using the NPS and its scoring variants are depicted in Figure 2. The average pain scores obtained reflect moderate to severe pain experienced in PLWHA and DSPN. With the one outlier removed, the average FR distance was clustered around the mean of 36.07 cm. The 6MWD varied greatly in this sample of PLWHA, with a mean distance walked of 243.99 m. This mean ambulation distance represents a 40% reduction in distance walked than previously reported mean ambulation distance measured in PLWHA using similar methods. 6
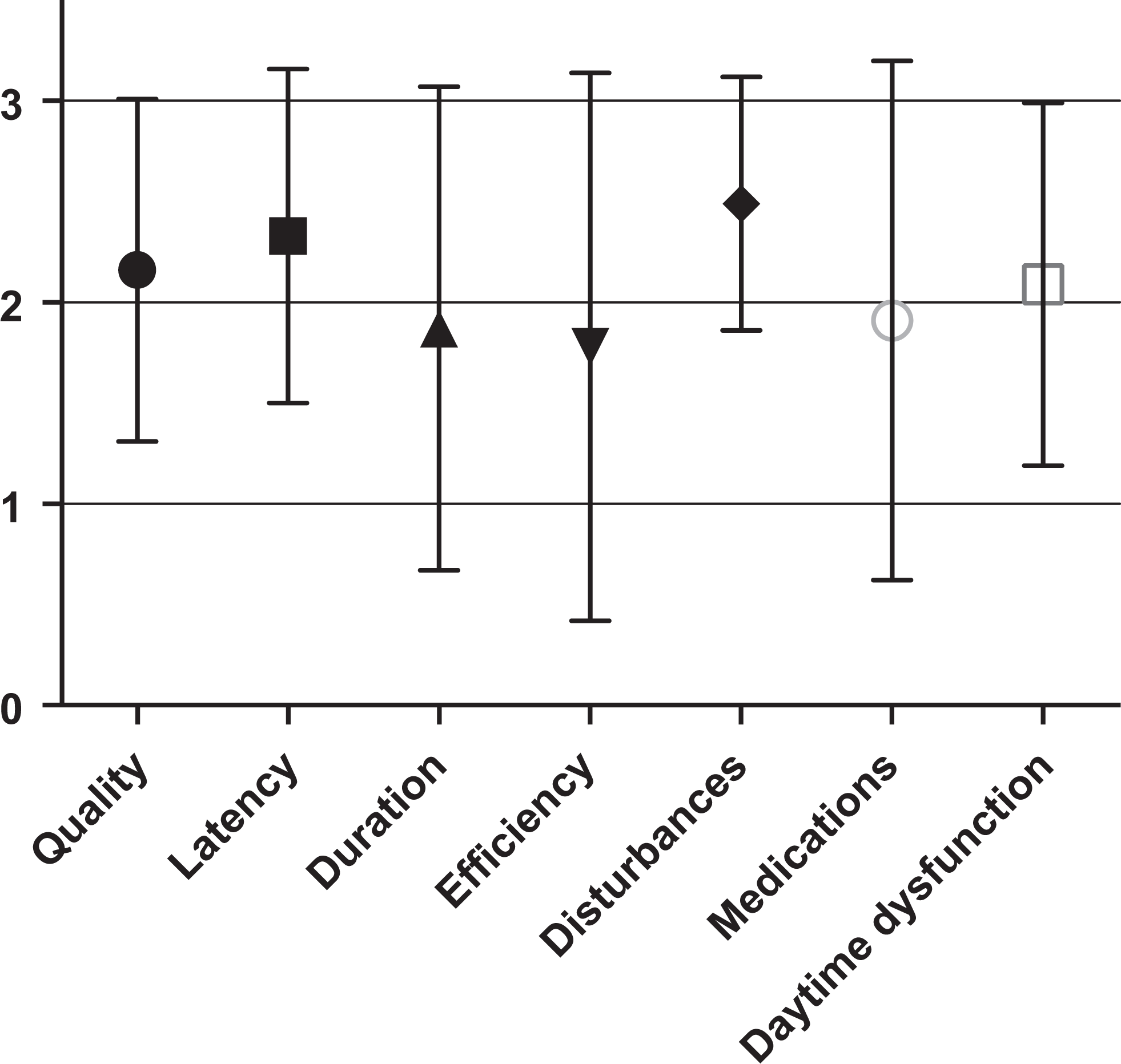
Average Pittsburgh Sleep Quality Index (PSQI) subscale scores (maximum score = 3).

Neuropathic Pain Scale (NPS) scoring options and NPS-pain intensity.
The 6MWD data point distribution revealed the presence of a bimodal distribution with a virtual threshold at 250 m, see Figure 3. The group of participants was stratified based on the 6MWD, a group of participants with walking distances above 250 m (n = 21, 380.05 ± 58.42 m) and a group of participants walking less than 250 m (n = 24, 127.90 ± 70.00 m). A subanalysis of the 6WMD groups confirmed the presence of 2 independent groups based on the participant’s ability to walk above or below 250 m, t(43) = −12.84, P < .0005. The participants that were able to walk more than 250 m exhibited longer FR distances (39.47 ± 7.14 cm) than those walking less than 250 m (33.22 ± 6.40 cm), t(42) = −3.07 and P = .004. The walking distance groups were significantly different based on the gender distribution, z = −2.31, P = .021. Of the 19 women in the study, 14 (74%) were included in the group able to walk below 250 m in 6 minutes, compared to 5 (26%) of the 19 in the group of participants walking more than 250 m in 6 minutes. The global PSQI scores appeared higher in the group of participants able to walk less than 250 m (15.79 ± 4.06), compared to those walking more than 250 m (13.29 ± 4.21), z = −1.96 and P = .05. All other descriptive variables failed to reach a level of significance below 0.05 for this subanalysis.

Function data point distribution.
Associations
Bivariate correlations were obtained between the descriptive variables. A significant inverse association was found between the number of CD4 cells and the PSQI scores, rs = −.33 and P < .05. The amount of CD4 counts also exhibited a significant inverse relationship between the scores obtained in the PSQI subscales of sleep latency (rs = −.35, P < .05) and sleep duration (rs = −.36, P < .05). Men in this study exhibited longer 6MWD, rs = .39 and P < .01. No significant associations were found between the age of the participants and the sleep scores, pain scores, 6MWD, and average FR distance, P > .05. Only the sleep latency subscale exhibited a significant association with the 6MWD, rs = −.32 and P < .05. The number of years living with HIV/AIDS was inversely associated with PSQI scores (rs = −.36, P < .05), scores in the PSQI subscale of sleep latency (rs = −.33, P < .05), and sleep efficiency (rs = −.35, P < .05). No significant association was found between the sleep scores and the self-reported pain intensity scores, P > .05. As predictable, sleep scores were correlated with each other, as were pain measures. In addition, pain and sleep scores were generally associated (rs > .40, P < .01), although not in respect to daytime dysfunction scores and use of sleep medications, P > .05. The FR and 6MWD were also associated (r = .46, P < .01), but neither was significantly associated with pain or sleep scores on any consistent manner. All correlations’ coefficients between sleep, pain, and functional performance are given in Table 2.
Correlation Matrix.

Abbreviations: FR, forward reach; NA, nonallodynic; NPS, Neuropathic Pain Scale; PSQI, Pittsburgh Sleep Quality Index; 6MWD, 6-minute walk distance.
a Pearson.
b P < 0.01 (2-tailed).
c Spearman.
d P < 0.05 level (2-tailed).
Discussion
Pain, sleep, and function characteristics presented in this study provide us with greater insight into the association between pain, sleep disturbances, and function in PLWHA with a diagnosis of DSPN. The data collected in the current study suggest that PLWHA and DSPN live in moderate to severe pain, are poor sleepers, and exhibit limited ambulation distance. The average NPS-10 in the current study was greater than 60 of 100. All the participants in this study had PSQI scores greater than 5 of 21, classifying them as poor sleepers. The average sleep score recorded in the current study sample is nearly 17% higher than the one reported in cohorts of people living with insomnia. 24 The data collected in the current study suggest that sleep quality is influenced by lower CD4 counts and longer duration of HIV/AIDS. These findings are similar to those reported by Lee et al, 4 where the authors found significant sleep disturbances in PLWHA, which increased with HIV infection’s progression into AIDS. Long-term survival with HIV infection exhibited an inverse relationship to sleep scores, perhaps suggesting an adaptation to chronic sleep disturbances in this cohort. Galer et al 16 indicated an increased sensitivity and discriminant validity of the NPS score in all of its scoring options (NPS-10, NPS-4, NPS-8, and NPS-NA) over those obtained using the self-reported pain intensity alone. In the current study, pain intensity scores alone did not exhibit a significant association with functional performance tests, pain, and sleep scores. Conversely, a small yet significant association was found between NPS and PSQI scores, suggesting that these variables represent different but related constructs. These findings suggest that future researchers may opt to use any of the NPS scoring options, as they appear equivalent in capturing the construct of pain in PLWHA and DSPN. Using shorter versions of self-reported questionnaires has an added advantage of reducing the response burden on future study participants.
The recorded 6MWD represents 60% of the distance walked compared to that reported in previous PLWHA cohorts, 6 albeit large variability was noted in the current sample of participants with DSPN for this variable. The results of the 6MWD distance revealed the presence of 2 independent groups based on their walking distance. Manor and Li 7 reported an average 6MWD of 391 ± 27 m collected on a sample of 20 sexagenarian volunteers living with neuropathic conditions due to multiple etiologies. The current 6MWD collected in younger participants appears to be 40% lower than those previously reported in people living with neuropathy not associated with HIV infection. 7 The results of the 6MWD stratification based on the participant’s ability to walk 250 m suggest that women with HIV-related DSPN may exhibit greater functional disadvantages and sleep disturbances compared to men. The lack of homogeneity of the sample from Manor and Li 7 may also account for the discrepancy in 6MWD. The data collected in this sample of PLWHA with HIV/AIDS-related DSPN suggest that the distance walked was most influenced by sleep efficiency, defined in the PSQI as the ratio of the number of hours slept divided by the number of hours in bed. The average PSQI-sleep efficiency in the current study was calculated at 60.93% ± 32.27% compared to a higher efficiency score of 80.30% ± 12.90% in people with a clinical diagnosis of insomnia. 24 The associations between CD4 count, years living with HIV diagnosis, and pain appear to exert significant influence on self-reported sleep quality. Sleep quality in turn was reported to influence the 6MWD; therefore, a possible correlation matrix centered on self-reported sleep quality emerges. Future studies are needed to confirm the strength of these associations and the presence of the proposed matrix centered on self-reported sleep quality.
The average FR distances recorded in this sample of PLWHA and DSPN appeared to be associated only with the 6MWD and not with the pain or sleep disturbances. Manor and Li 7 reported significantly increased oscillations of the center of mass (COM) during quiet standing in individuals with diabetic neuropathy. The current study focused on the participants’ ability to volitionally control the COM along the sagittal plane while reaching forward. The average FR distances reported in the current study suggest a normal ability to perform this reaching task compared to sero-negative, age-matched individuals (34.73 ± 7.54 cm). 6 Finally, the average recorded FR distance suggests a very low risk of falls in this cohort of participants. 23
This current study was limited by its inability to confirm the DSPN diagnosis with more invasive clinical tests such a punch skin biopsies. In this study, 31% of the participants had detectable levels of viremia, which may have contributed to higher reports of pain and sleep disturbances in this cohort. Additionally, all the participants were recruited at a public outpatient clinic where the demographic characteristics may differ from those of PLWHA and DSPN followed in private practice settings. People living with HIV/AIDS with recent HIV/AIDS diagnosis may not have been adequately represented. Finally, unilingual Spanish-speaking PLWHA may have been underrepresented in this study, as the questionnaires used have only been validated in their English version.
Summary
Pain, sleep, and functional disturbances are a common occurrence in HIV/AIDS-related DSPN. The data reported in the current study suggest the presence of significant relationships between the constructs of pain, sleep disturbances, and function. Of particular interest is the high PSQI scores recorded in PLWHA and DSPN, which were found to be 17% higher than those reported in people living with clinical diagnosis of insomnia. The 6MWD in PLWHA and DSPN appears to be associated with sleep disturbances and not self-reports of DSPN-associated pain. Future studies should validate the proposed matrix of function, pain, and HIV disease factors with self-reported sleep quality in the center. Paradoxically, the results of the FR test suggest a normal ability to volitionally translate the COM along the sagittal plane and exhibit a significant association with the 6MWD. The latter may suggest the presence of separate yet related constructs of physical endurance and balance. Finally, significant gender differences in function were observed in the current study which would warrant further investigation.
Footnotes
Acknowledgments
The authors would like to thank the Harris County Hospital District Foundation (Houston, TX) and Don Joy Orthopedics (Vista, CA) for their generous research support.
Authors’ Note
RS designed the study, collected the data, and enrolled the patients and analyzed the data in this study as part of his doctoral dissertation. TR (chair), TG, KM, and CK were part of the dissertation committee overseeing this research, provided scientific guidance, and editing assistance to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by the Harris County Hospital District Foundation (Houston, TX) and Don Joy Orthopedics (Vista, CA).