
Abstract
Objectives:
Nigeria has the world’s highest burden of pediatric HIV. In the face of paucity of monitoring tests in Nigeria, we studied the spectrum of pediatric mucocutaneous manifestations and evaluated their clinical utility as surrogate markers for immunodeficiency and plasma viral load levels.
Methods:
Cross-sectional study comparing mucocutaneous manifestations in 155 HIV-positive children aged 12 weeks to 14 years with 155 HIV-negative children. Relationships between mucocutaneous manifestations in HIV-infected patients and their immunologic and virologic indices were analyzed.
Results:
Mucocutaneous lesions were seen in 53.5% of HIV-infected children compared with 18.1% of the controls. Prevalence of lesions increased with worsening levels of immunodeficiency and increasing viral loads (P < .01). Oral candidiasis, angular stomatitis, and fluffy hair were associated with more severe degrees of immunodeficiency.
Conclusion:
Mucocutaneous disorders are common in HIV-infected children. Oral candidiasis and nutritional dermatoses can be used as surrogates for advanced or severe immunodeficiency.
Introduction
Nigeria has been ranked second to South Africa in the number of people living with HIV. In 2011, 3.4 million people were living with the virus in the country. It also has the world’s highest burden of pediatric HIV of approximately 440 000 (2011) children living with the virus. 1 In spite of this, several regions of the country lack immediate access to monitoring tools that are essential for efficient management of these patients.
The manifestations of HIV are myriad, with a high susceptibility to infectious, inflammatory, and malignant diseases. They arise as a result of a critical abnormality leading to a progressive decline in the number of CD4+ T-lymphocytes with the viral burden directly and indirectly mediating CD4+ T-cell destruction. 2,3 Viral load indicated by the number of plasma viral RNA copies per milliliter is an indication of HIV replication and progression and together with CD4 indices are used as monitoring tools to determine the progress of the disease. 4
In many resource-poor countries like Nigeria, the World Health Organization (WHO) immunologic criteria is used to classify children into 4 different levels of immunodeficiency based on age and CD4%. 5 Infected children with the “not significant” and “mild levels” of immunodeficiency are not eligible for antiretroviral therapy (ART) unless the clinical stage of disease is advanced or the child is less than 2 years of age, whereas those with the “advanced” and “severe levels” of immunodeficiency are eligible for ART irrespective of the disease stage or age of the child. However, CD4 profile of an infected child, which may be necessary to determine the ART eligibility, may not always be available.
Skin disorders have been reported to be very common in HIV, and as high as 90% of infected adult patients will have these manifestations at one time or the other. 6 Previous studies have correlated these disorders with immunodeficiency levels. 7 –10 In the face of a high burden of disease and paucity of monitoring tools, we studied the spectrum of mucocutaneous disorders in a population of HIV-infected Nigerian children and investigated the clinical utility of these disorders as surrogates for immunodeficiency and viral load levels.
Materials and Methods
This was a descriptive cross-sectional comparative study that involved HIV-infected children aged between 6 weeks and 14 years and age- and sex-matched controls. The study participants were recruited from the pediatric infectious disease clinic (IDC) and the wards of the University College Hospital, Ibadan, a tertiary center in South West Nigeria.
The IDC is one of the treatment centers for HIV funded by the President’s Emergency Plan for AIDS Relief (PEPFAR) and the Nigerian Government. It operates once a week when patients with HIV and tuberculosis are followed up, with an average of 30 HIV-positive children attending per week. CD4 counts, CD4 percentage, and viral load were performed monthly as part of the routine evaluation of HIV-infected children attending the clinic. Infected children who were too ill to be managed as outpatients were admitted into the pediatric wards. All children had free access to antiretroviral drugs, and based on the National guidelines for pediatric ART in Nigeria, all eligible children were commenced on antiretroviral drugs.
Controls were HIV-negative children seen in the general pediatric outpatient clinics, with no chronic illnesses and who were not on chronic medications.
Recruitment was carried out between May 2009 and April 2010. Children considered eligible for the study were recruited consecutively provided they and their caregivers were willing to participate. HIV diagnosis was based on positive rapid diagnostic tests confirmed by positive HIV DNA polymerase chain reaction in children younger than 18 months and Western blot in children older than 18 months.
Ethical clearance was obtained from the Health Research Ethics Committee of the University College Hospital. Signed informed consent was obtained from the caregiver/parent of eligible children after a clear explanation of the study was given. An assent was also sought from the children 10 years and older who were old enough to understand. A semistructured questionnaire was administered to obtain sociodemographic information as well as clinical history. A complete physical examination in a well-lit room after proper exposure of each child was carried out by the investigator to identify all possible mucocutaneous disorders. Areas examined included the hair, scalp, face, trunk, nails, oral mucosa, genitalia, and extremities. For the physical examination of older children, 10 years and older, a chaperon was present. A picture of each lesion was taken, and the diagnosis of the skin disorder was mainly clinical. Where relevant, investigations such as skin biopsies, skin scrapings, and swabs were carried out by a pediatric dermatologist. All suspected malignancies were diagnosed histologically. Investigations such as CD4 count, CD4 percentage, and viral load were also performed.
Based on the CD4 count and percentage, each HIV-positive child was classified as having, not significant, mild, advanced, or severe immune suppression using the WHO classification of HIV-associated immunodeficiency in infants and children. This was subclassified into 2 groups for ease of some statistical analyses. Based on the viral load, the HIV-infected children were also classified as having a high or low viral load using the cutoff of 100 000 viral RNA copies/mL. This was adapted from a study by Mofenson et al. 11
Data were analyzed with the Epi info version 2007. Frequency distribution tables and cross tabulation of variables, graphs, and charts were generated to report descriptive statistics. Discrete variables were compared using the chi-square test, whereas continuous variables were analyzed using the paired t test. The level of significance was established at P value of <.05.
Results
The 155 HIV-positive children studied comprised of 92 boys and 63 girls (male–female ratio of 1.5:1), which was similar to the controls. The major mode of transmission was maternal-to-child transmission. More than half (62.6%) of the HIV-infected children were orphans. Of the children whose parental HIV serostatus was known, 38 of them had discordant serostatus (Table 1). Most (72.9%) of the patients were on ART and the mean duration on ART was 20.52 ± 15.25.
Sociodemographic Characteristics of the Study Population.

Abbreviation: MCT, maternal-to-child transmission.
Mucocutaneous lesions were found in 53.5% of the HIV-infected children, which was significantly higher than 18.1% found in the uninfected children (odds ratio = 5.2; 95% confidence interval = 3.03-9.08; Table 2).
Among the infected children with severe immunodeficiency, mucocutaneous disorders were found in 80.6% of them, which was significantly higher than 35.9% seen in those with “not significant” immunodeficiency. Similarly 78.1% of children with high viral load had mucocutaneous lesions, which was also higher than 47.2% seen in those with low viral load ( Table 2).
The prevalence of skin disorders among those on ART compared to those not on ART was significantly lower (Table 3).
Association between Presence of Mucocutaneous Disorders and Levels of Immunodeficiency and Viral Load.

a Significant.
Use of ART in Relation to the Presence of Mucocutaneous Disorders in HIV-Infected Children.

Abbreviation: ART, antiretroviral therapy.
a Significant.
Figure 1 shows the disorders seen in both groups of children. Those seen exclusively in the HIV-infected children include nutritional dermatoses like angular stomatitis (2.6%) and fluffy hair (2.6%); pruritic papular eruptions (9%), generalized xerosis (5.2%), Kaposi sarcoma (1.3%), pityriasis vesicolor (1.3%), and generalized pruritus (1.3%). Specific mucocutaneous lesions that were associated with worsening levels of immunodeficiency are as shown in Table 4.
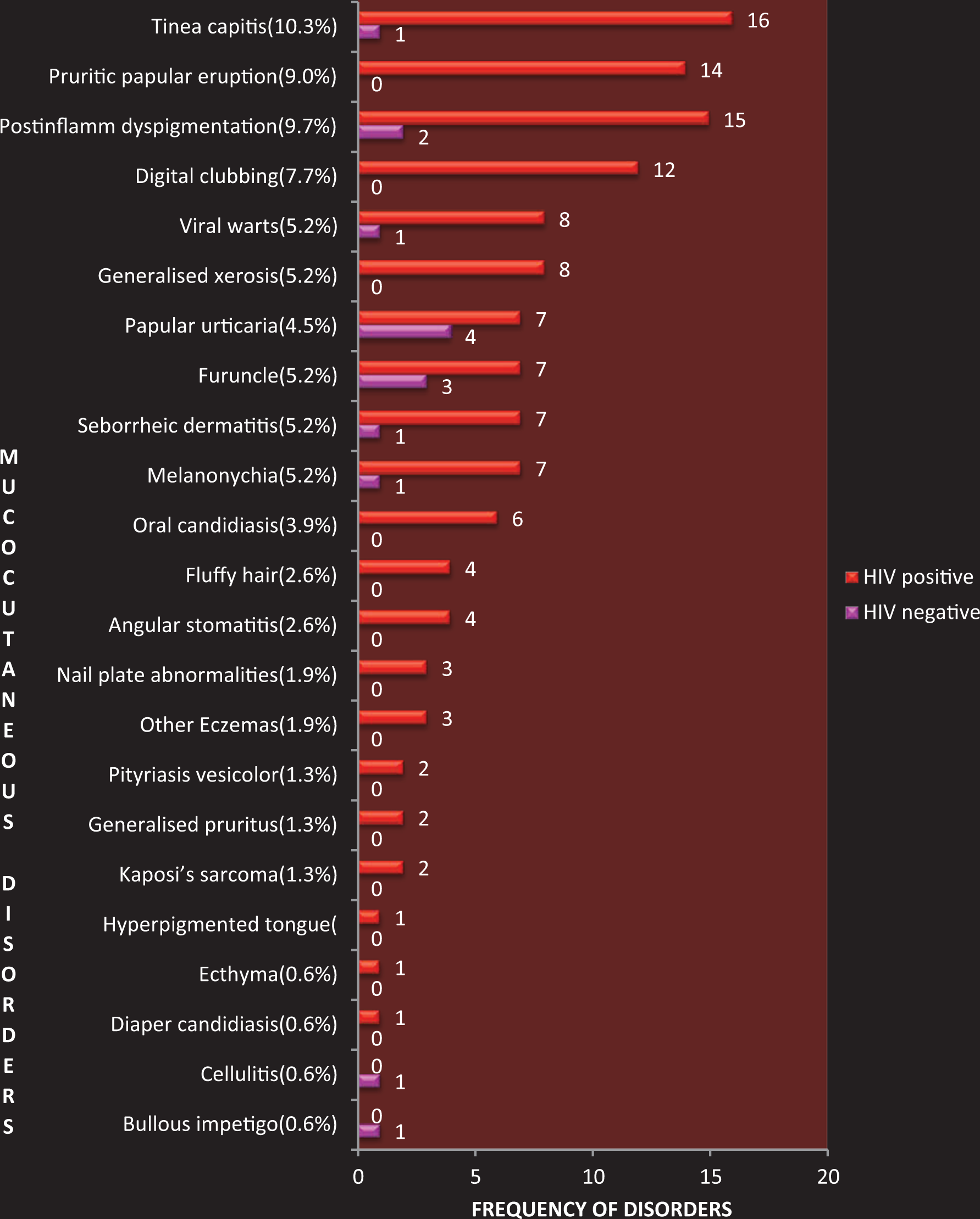
Spectrum of mucocutaneous disorders in HIV-infected children in comparison to HIV-negative children.
Relationship between Specific Mucocutaneous Disorders and Immunodeficiency Levels.
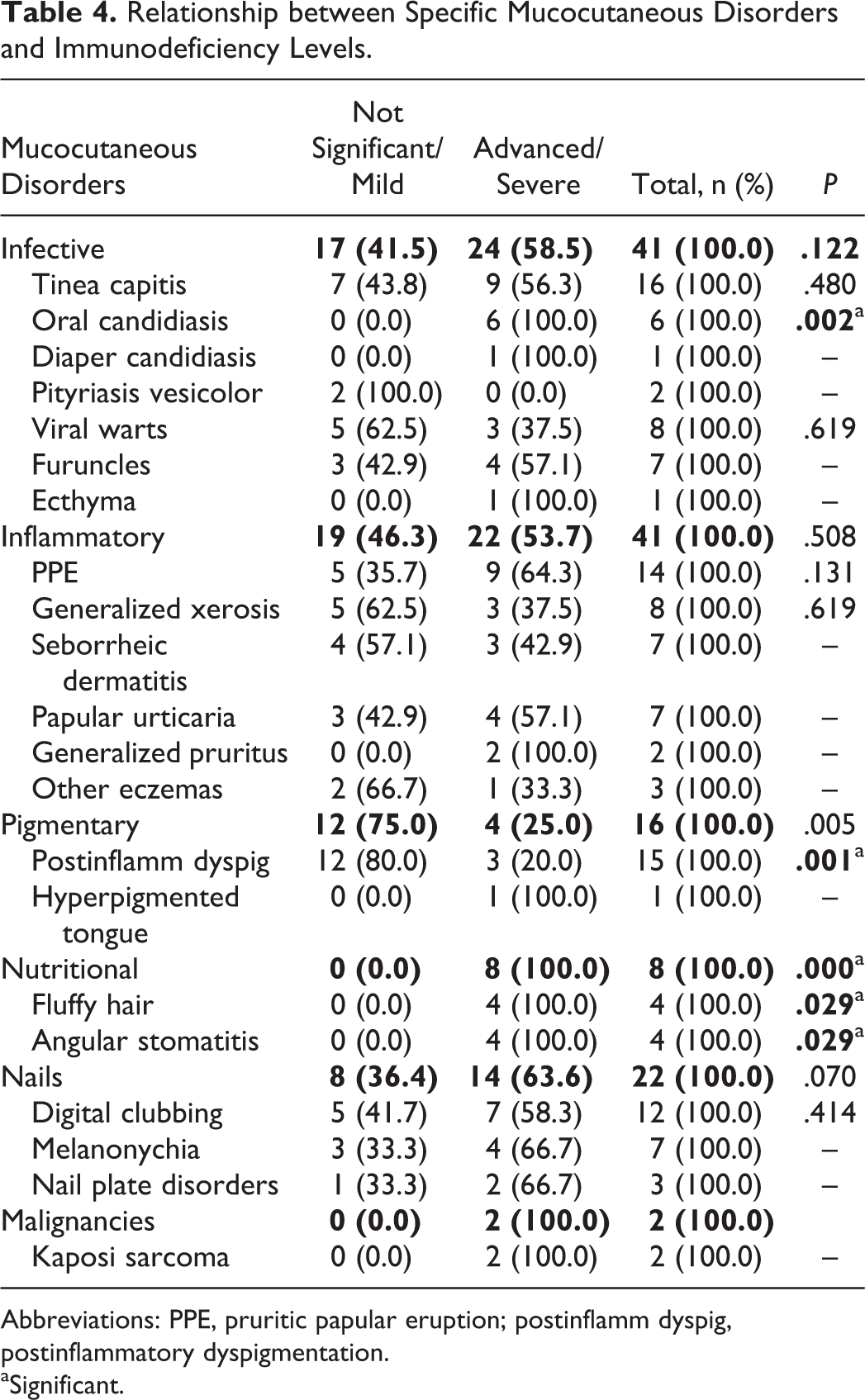
Abbreviations: PPE, pruritic papular eruption; postinflamm dyspig, postinflammatory dyspigmentation.
aSignificant.
Cutaneous disorders significantly associated with low viral load are as shown in Table 5. No mucocutaneous manifestation was significantly associated with a high viral load.
Relationship between Specific Mucocutaneous Disorders and Levels of Viral Load.

Abbreviation: postinflamm dyspigment, postinflammatory dyspigmentation.
aSignificant.
The mean CD4% of the nutritional dermatoses was the lowest (less than 15%), whereas the mean viral load of the malignancies (Kaposi sarcoma) was the highest (>700 000 viral RNA copies/mL). Postinflammatory dyspigmentation was associated with the lowest mean viral load <100 000 viral RNA copies/mL as well as the highest CD4% (>25%; Figure 2).

Mean CD4% and viral load of the various groups of mucocutaneous disorders in HIV-infected children.
Discussion
Varying prevalent rates have been found for mucocutaneous disorders in HIV. Our prevalent rate of 53.5% is comparable to cross-sectional studies in Thailand 7 and Chile, 10 with a prevalence rate of 51.6% and 56%, respectively. It is however slightly lower than other cross-sectional studies in Africa, and this could be related to the characteristics of the patient like the age range, sample size, and use of ART. 12,13 In Tanzania, the age ranged from 6 months to 16 years, with a sample size of 374 and a prevalence of 85%. 12
These skin disorders were also significantly higher in HIV-infected children (53.5%) than their HIV-negative counterparts (18.1%). In a study of 196 symptomatic HIV-infected children between 1 month and 12 years, Davachi in Zaire had a prevalence of 65% compared to 22% in HIV-negative controls. 14
Cutaneous abnormalities have been attributed to decreased capability of the Langerhans cell in the skin of the HIV-infected children to induce proliferation of the T lymphocytes, thereby compromising the immune system.
The infective skin diseases are usually the most common type of skin disorder as corroborated in our study; however, the inflammatory dermatoses reported by Carvalho et al 15 was just as common.
The higher incidence of fungal skin disorders among the infective disorders in HIV-infected children was in contrast to the more prevalent bacterial dermatoses among the uninfected. Cotrimoxazole, which is routinely given to the infected children, may be responsible for this observation. However, among infected children bacterial dermatoses, when present, were more severe (Figure 3).

Multiple furuncles that are unusually large in a 6-month-old child with severe immunodeficiency.
Tinea capitis (10.1%) was the most prevalent cutaneous disease and the only dermatophytic lesion observed in this study. Tinea unguium found by Umoru et al 13 was not seen; however, it is a lesion common in adolescents and adults, and considering that the age range of that study extended to 18 years, such findings are not unexpected. HIV-infected children with tinea capitis had extensive lesions with multiple areas of scarring, even more so with worsening immunodeficiency.
Oral candidiasis noted in many reports 16 –18 as the most common fungal infection was the second most common after tinea capitis. This is similar to other studies in Africa, where dermatophytosis was more prevalent. 12,13 Only the pseudomembranous form was seen involving the tongue and buccal mucosa, and it was associated with the higher levels of immunodeficiency. This is similar to the findings by Lim et al. 19
The only viral skin disorder seen in infected children was viral warts (5.2%), and the only variant found was the planar warts (Figure 4A). Four children had “epidermodysplasia verruciformis-like” lesions characterized by hypopigmentation resembling pityriasis vesicolor with a typical distribution on the face, neck, and upper trunk (Figure 4B). This finding has also been previously documented in HIV-infected children. 20,21 This could serve as a pointer to the disease, which may hence warrant screening.

A, Flat warts the only viral disorder seen. B, “Epidermodysplasia verruciformis” a variant of flat warts in a child with low viral load.
Pruritic papular eruption, generalized xerosis, and generalized pruritus are inflammatory dermatoses exclusively seen in the HIV-infected children. Pruritic papular eruption, the second most common cutaneous disorder (9%), is a common manifestation of HIV in Africans (Figure 5). It is postulated that this condition reflects an altered and exaggerated immune response to arthropod antigens in susceptible HIV-infected patients. 22 Symmetric pruritic papules were found commonly around the limbs and in some cases involving the face and the trunk. It has been significantly associated with advanced and severe immunodeficiency states, though this finding was not corroborated in this investigation.

Pruritic papular eruptions and “half and half nails” in a child with severe immunodeficiency.
Nail abnormalities were prominent in this study. Digital clubbing, the most common abnormality, was seen only in infected children (Figure 6). Most patients had grade 3 or 4 lesion. The etiology of finger clubbing among HIV-positive patients could be an area for future research as this was not within the scope of this study.

Digital clubbing, the most common nail disorder. Note the bulbous uniform swelling of the nail with loss of the normal angle between the nail and the nail bed.
Black melanonychia with varying involvement of the nail plate and nail bed was seen. Two patients had longitudinal melanonychia, and this has been associated with zidovudine (ZDV) therapy. 23 Zidovudine therapy may also have been the cause of a hyperpigmented tongue seen in 1 child, as previously reported. 24 This child had been on this drug for about 6 months; however, there were other children who had been on the same therapy for much longer without any similar lesion.
“Half and half nails” seen in a child was characterized by distal brown and proximal white discoloration of the nails and has been described in HIV and mimicks the nail findings in chronic renal failure (Figure 5). 25 However, this child did not have features of uremia.
The only malignancy seen was Kaposi sarcoma found in 2 HIV-infected adolescent boys. It is rare in HIV-infected children compared to adults. 16 The variant in both cases was the mucocutaneous form with lesions in the palate (Figure 7A) and the eye in one case and involvement of the right foot in the other (Figure 7B). Mean CD4% was 17%, and mean viral load was 717 494 copies/mL.
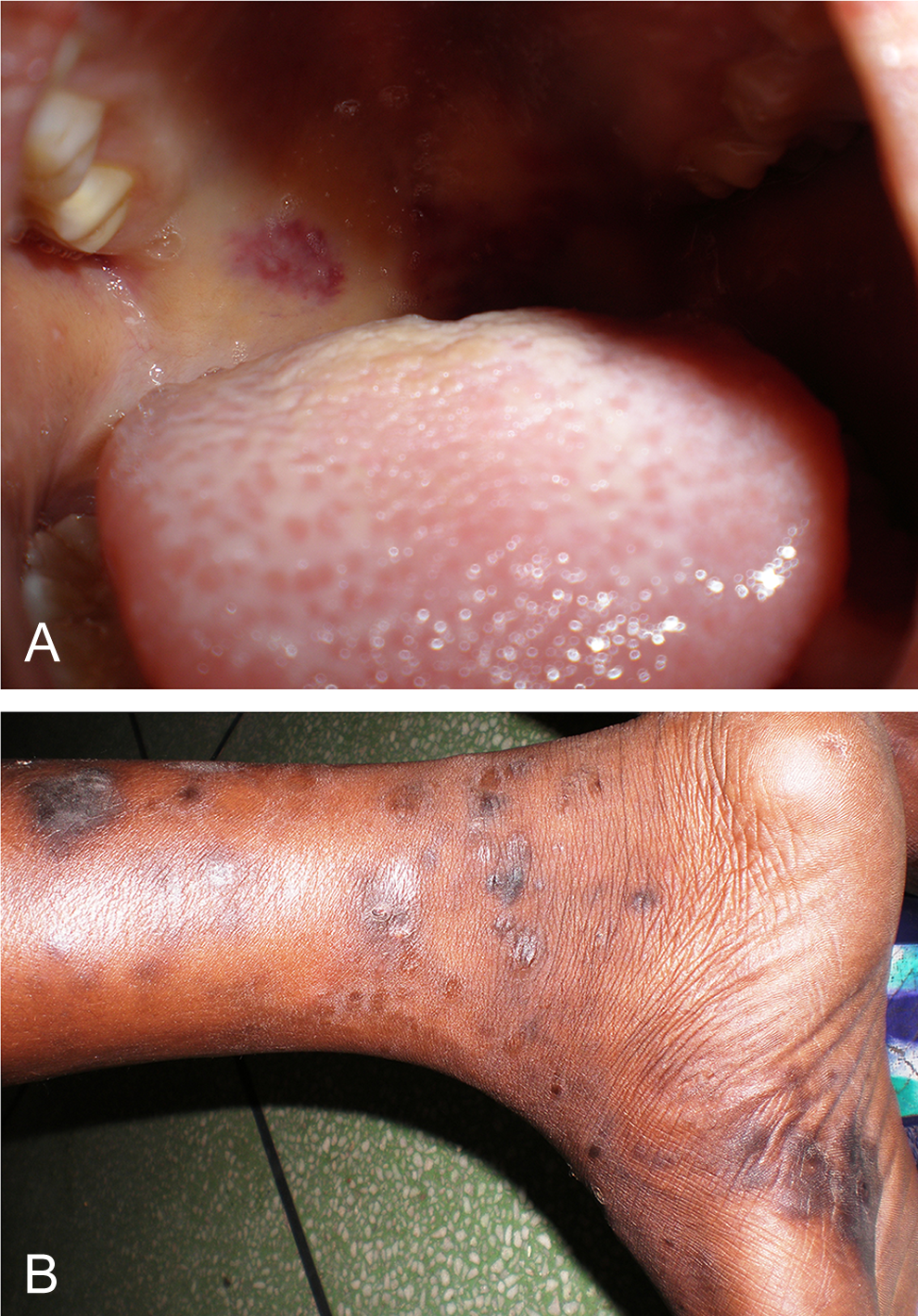
Mucocutaneous Kaposi sarcoma involving (A) palate and (B) the right leg.
A significantly higher percentage (80.6%) of children in the severe immunodeficiency group had mucocutaneous disorders than those who had insignificant levels (35.9%) of immunodeficiency. This is similar to the findings of Wananukul et al 8 in which 62% and 20% of the patients in the severe and no immunosuppression categories, respectively, had these lesions. However, the immunological classification for that study was based on the US Centers for Disease Control and Prevention, which has 3 subclasses as opposed to 4 in the WHO classification system used in our study.
The above findings imply that delay in presentation of infected children with subsequent development of severe immunodeficiency predisposes to higher incidence of cutaneous abnormalities, leading to a reduced quality of life.
A higher percentage (78.1%) of those with high viral loads than those with low viral loads (47.2%) had mucocutaneous lesions, thus corroborating the findings of Carvalho et al. 9 Very few studies have related cutaneous disorders to viral load.
In Spain, Seoane Reula et al 26 found a significant reduction in the prevalence of cutaneous diseases following the introduction of HAART. This has been similarly corroborated by this study where a much lower prevalence of cutaneous lesions was found among those who had not been initiated on HAART compared to those on HAART. The use of HAART in 79.4% of our patients may be responsible for the absence of some disorders like the parasitic dermatoses, scabies, and other viral abnormalities like herpes simplex and molluscum contagiosum.
Like oral candidiasis, nutritional dermatoses also observed by El Hachem et al 16 were significantly associated with immunodeficiency with a mean CD4% of 7.8%. Fluffy hair is indicated by the presence of thin sparse hair usually occurring due to hypoprotenemia, and angular stomatitis arises as a result of micronutrient deficiencies.
Postinflammatory dyspigmentation was significantly associated with lower levels of immune deficiency as well as low viral load. Hyperpigmentation was more common than hypopigmentation. These findings appear to be sequelae of other dermatoses that these children had during the course of their illness. Dyspigmentation secondary to herpes zoster (Figure 8) was seen in a 2-year-old infected boy with no apparent history of chicken pox.

A and B, Postinflammatory dyspigmentation following Herpes zoster. Note the dermatomal lesions.
No specific mucocutaneous manifestation was significantly associated with high viral load. This may be due to the fact that very few (20.6%) of the infected children in this study had a high level of viremia. Papular urticaria, seborrheic dermatitis, postinflammatory dyspigmentation, melanonychia, and viral warts were specific skin disorders associated with low viral load. Smith et al 27 reported that viral warts can be seen early in HIV infection and are not associated with disease progression. It can thus be inferred that these disorders may not be markers of HIV progression and can be seen even at very low levels of HIV viremia.
Conclusion
Mucocutaneous disorders are very common in HIV-infected children seen in South Western Nigeria, with dermatophytic infections being the most prevalent. Oral candidiasis and nutritional dermatoses are reasons to suspect advanced or severe immunodeficiency. Postinflammatory dyspigmentation, though common and could be generalized in these children, tends to be seen in infected children with lower levels of immunodeficiency. Pediatric HIV treatment and care centers that have no immediate access to monitoring tools can use these clinical disorders as surrogates.
Study Limitations
This study does not represent all the cutaneous manifestations that can be seen in the children attending the IDC as only a subset of children were examined, and cross-sectional past or newly evolving mucocutaneous disorders could not be assessed. Larger longitudinal studies need to be undertaken to develop an algorithm of skin disorders, which can be used as rough estimates of immunodeficiency levels and plasma viral load indices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.