
Abstract
Background:
HIV-associated neurocognitive disorder (HAND) is a great source of morbidity in sub-Saharan African region. However, the magnitude of this problem remains largely uninvestigated despite having the largest number of population with HIV/AIDS. The aim of this study is to determine the prevalence of HAND among patients attending a tertiary health facility in Nigeria.
Method:
We conducted a cross-sectional study among HIV-positive patients on antiretroviral therapy (ART) for at least 1 year. They were assessed using the International HIV Dementia Scale, Word Recall Test, Stick Design Test, Subjective Cognitive Complaint Questionnaire, Alcohol Use Disorder Identification Test, Drug Abuse Screening Test, Center for Epidemiological Study–Depression Scale, Instrumental Activity of Daily Living, and neurological examination. The CD4 count and viral load were determined for all the participants. A consensus diagnosis was made on each case based on the Frascati criteria. Data obtained were analyzed using “SPSS” for Windows version 15.
Results:
A total of 418 HIV-positive patients participated in the study, of which 325 (77.8%) are females. The mean age (standard deviation) of the participants was 37.2 (9.3) years. The prevalence of HAND was 21.5% (95% confidence interval [CI] = 17.6%-25.4%), of which 9.6% were asymptomatic. The significant predictors of HAND in this study are duration of illness (odds ratio [OR] = 1.33 P < .001), detectable viral load (OR = 0.19, P < .001), CD4 count (OR = 0.99, P < .001), education (OR = 0.94, P = .011), stopping medication (OR = 3.55 P = .01), and severity of illness (OR = 1.24, P = .005).
Conclusion:
One-fifth of the HIV-positive patients in this study had HAND. Various sociodemographic and clinical features were related to the prevalence of HAND.
Introduction
One of the important challenges facing the human race in the 21 century is AIDS caused due to HIV infection. 1 The sub-Saharan African (SSA) countries have the highest prevalence of people with the disease, accounting for almost two-third of the cases. 1 –4 The introduction of antiretroviral (ARV) drugs have prolonged the survival and improved the quality of life among people living with HIV/AIDS (PLWHA). 5 However, neurological complications of the disease have remained a great source of morbidity and burden and significantly decreased the quality of life among these patients and the informal caregivers of PLWHA. 6,7
In the early years of HIV epidemic, various terms like HIV encephalopathy, AIDS dementia complex, and HIV-associated dementia had been used synonymously to describe the neuropsychiatry complications of advanced HIV infection. 8,9 In recent years, the term HIV-associated neurocognitive disorder (HAND) has become more popular and streamlines the nosology of neurological complications of HIV infection. HAND refers to a spectrum of neurological complications of HIV infection, which includes HIV-associated asymptomatic neurocognitive impairment (ANI), HIV-associated mild neurocognitive disorder (MND), and HIV-associated dementia (HAD). 9 –11 The diagnosis of HAND is based on the evaluation of at least 5 out of 7 cognitive domains, which include executive function, episodic memory, motor skills, speed of information processing, language, attention/working memory, and sensory perception. 11 The formulation of Frascati criteria in 2007 streamlines the diagnosis of HAND and recognizes cognitive disturbance and impairment in the activities of daily living as the most essential elements in the diagnosis of HAND. 11 Studies carried out in SSA region estimated the prevalence of HAND to be over 30%. 6,7
Despite the enormity of neurological and neuropsychiatric complications of HIV/AIDS, the magnitude of the problem remains largely undocumented in SSA. 2,6,7 Moreover, access to antiretroviral treatment (ART) by patients in Africa is limited, and it is often started late in the course of the disease, thereby predisposing them to neurological complications. 2 This study is aimed at determining the prevalence and factors associated with cognitive impairment among patients on ART attending a tertiary health facility in Nigeria.
Materials and Methods
Study Area
The study was conducted at the Ahmadu Bello University Teaching Hospital (ABUTH), Zaria, Nigeria. According to the national sentinel survey carried out in 2010, the prevalence of HIV in Nigeria was 4.1% (affecting about 3.1 million people); however, there are regional variations in the prevalence. 12 Benue state in North Central zone has the highest prevalence (ie, 10.6%), while Ekiti state in South West zone has a prevalence of 1.0%. 12 The Ahmadu Bello University Teaching Hospital, Zaria, is the largest referral center in Northern Nigeria. It provides specialized medical services not only for people in the region but also for patients from the neighboring West African countries. The HIV clinic is run in conjunction with international donor agencies. It provides HIV care that includes voluntary counseling and testing (VCT), ART for adult and pediatric patients, and prevention of maternal-to-child transmission (PMTCT) of infection. Basic laboratory investigations for patients with HIV/AIDS are also available in the center. HIV care in Nigeria is provided by all the 3 tiers of health care facilities in the country. In the primary health care (PHC) centers, the only service available is that of VCT, which is usually manned by a cadre of low level health personnel. While the secondary health facilities are manned by a cadre of middle level. The services available include VCT, ARV drug pickup, and routine laboratory services including CD4 count. In the tertiary health centers, comprehensive HIV/AIDS care services are provided. However, in all the 3 tiers of health facilities in Nigeria, mental health services are not provided for PLWHA. Northern Nigeria is the largest region in terms of land mass and population in the country. 13 A survey by the Nigeria National Statistics Bureau in 2010 reported that over 60% of the region’s population was living below the internationally acceptable level of poverty. 14 This is higher than the level of poverty in the Southern part of the country. The major ethnic group in the area is the Hausa-Fulani that are found not only in Nigeria but also across the West African subregion.
Sample Size Determination
Using a sample size calculation for single proportion, a sample size of 331 was estimated. This was oversampled by 26% to achieve a sample size of 418. This was done to improve the statistical power of the final sample. The power of n = 418 was estimated to be 1 using sample size power calculator.
Participants
The participants of the study are HIV-positive patients attending the ARV clinic of Ahmadu Bello University Teaching Hospital, Zaria. The inclusion criteria are that the HIV-positive patients must be at least 18 years old, should have been on highly active antiretroviral therapy (HAART) for at least a year and must have consented to participate in the study. The Ahmadu Bello University Teaching Hospital’s Human Research Ethical Committee gave approval for the study. An informed written consent was obtained from each of the participants or their next of kin before the start of the assessment, and the participants or next of kin were to sign or thumb print the consent form as a confirmation to participate in the study.
Instruments
The neuropsychological instruments used in this study were chosen based on their psychometric properties of ability to measure cognitive function and activities of daily living as contained in the Frascati criteria. In addition, the normative values of this instrument among Africans had been based on those reported by earlier studies. The participants were assessed using the following instruments. Sociodemographic data collecting sheet: This was designed to elicit variables like age, gender, education, income, and other sociodemographic variables. International HIV Dementia Scale: International HIV Dementia Scale (IHD) was developed by Sactor et al for the screening of dementia and cognitive impairment among HIV-positive patients.
15
It tests registration, recall, motor function, and information processing.
15
It has a sensitivity and specificity of 74% and 46%, respectively, at a cutoff point of 9.5.
15
The test has the advantage of not requiring any special instrument except a timer or wristwatch. It can be administered easily by other health workers, not necessarily by a physician. Another major advantage of the IHD is that it is free of cultural bias as it can be used in many developing countries of the world. Stick Design Test: The Stick Design Test (SDT) was developed by Baiyewu et al to test the visuoconstructional activity of individuals.
16
As opposed to the paper-and-pencil test, the SDT can be used to measure motor functions like constructional praxis in participants with little or no education. The test has the ability to differentiate between normal and cognitive-impaired individual. It has a possible score of 0 to 12. A normative score of 3 had been reported among Nigerians, using this instrument.
16
Word List Learning and Recall test: The 10 Word List Learning (WLL) and Word Recall Test (WRT) are part of the Consortium to Establish Registry for Alzheimer Disease.
17
It has been widely used to assess dementia and cognitive impairment in clinical setting.
18
This psychometric instrument test is used for registration and immediate recall of a patient. Even though HAD is a subcortical dementia, with the introduction of ART and increased survival of PLWHA, it is becoming difficult to distinguish from cortical dementia.
9
Its modified version had been widely used in developing countries including Nigeria.
19
A score of 3 or less is indicative of a possible cognitive impairment in the individual.
18,19
Subjective Cognitive Complaints questionnaire: The Subjective Cognitive Complaints (SCC) questionnaire is a brief self-report questionnaire of subjective cognitive complaints with specific items for 4 cognitive domains: memory, concentration, speech, and thinking.
20
It rates the problem patients have with memory, concentration, speech, and thinking. The questionnaire has a possible score range of 0 to 8. Higher scores are indicative of self-reported cognitive problem. The questionnaire has been used to assess self-reported problem with cognition among HIV-positive patients in cross-cultural studies.
21
Instrumental Activity of Daily Living: The Instrumental Activity of Daily Living (IADL) test was developed to assess the activities of daily living in the elderly individuals.
22
However, IADL has been used to assess the activities of daily living in patients with HIV/AIDS.
6
The test has a possible score range of 0 to 8, with higher scores indicative of optimal functioning. Center for Epidemiological Study–Depression Scale: The Center for Epidemiological Study–Depression Scale (CES-D) is a 20-item self-report depression screening instrument that has been widely used in Africa.
23,24
The CES-D scale has laid emphasis on depressive symptoms like depressed mood, feeling of guilt, worthlessness, and psychomotor retardation. Unlike Hamilton Depression Rating Scale (HAM-D) or Beck Depression Inventory (BDI), the CES-D contains few vegetative symptoms that can overlap with those of HIV/AIDS.
2,25
Unlike HAM-D or BDI, the CES-D can also be administered by nonclinicians.
25
A score of 16 and over is indicative of possible depressive illness. Alcohol Use Disorder Identification Test: The Alcohol Use Disorder Identification Test (AUDIT) is a 10-item instrument designed by the World Health Organization to screen excessive consumption, hazardous, and harmful use of alcohol.
26
The instrument has been validated in many countries including Nigeria.
27,28
A score of 8 and above is indicative of either harmful use or dependence. Drug Abuse Screening Test: Drug Abuse Screening Test (DAST) instrument was designed to screen for drug use other than alcohol.
29
The DAST-10 version was used in this study and is answered in a “yes or no” pattern. A score of 3 and above is indicative of problem with psychoactive substance abuse.
29
CD4 count was carried out for each participant using flow cytometry method with an automated Partec cyfolw counter manufactured by PARTEC-GMBH PARTEC machine. Viral load was carried out for each of the participants using reverse transcriptase method with an automated machine (cobas Ampliprep) by ROCH-AMPICLOR. Physical examination was conducted for each of the participants with an emphasis on neurological examination.
Using the back translation method, all the psychometric instruments were translated into Hausa Language, which is the predominant language of the area.
Training on the Use of the Instruments
Two research assistants were trained in the administration of the psychometric instruments. The research assistants are university graduates and are fluent in both English and Hausa languages. They were trained in the administration of the instruments by one of us (A.J.Y.). The test–retest reliability between the 2 research assistants and A.J.Y. was .85.
Procedure
The participants were recruited on each clinic day through balloting of patients who fulfilled the inclusion criteria. Two trained research assistants interviewed the study participants using the psychometric instruments. Physical examination and collection of blood specimens from the participants were carried out on the same day of the interview by 2 of the authors, A.J.Y. and A.H., who were blind to the scores of the psychometric instruments. A consensus diagnosis was made for each of the participants based on Frascati criteria,
11
taking into consideration the scores of the psychometric instruments by a panel that included a psychiatrist (A.J.Y.) and 2 hematologists (A.H. and A.M.S.). The Frascati criteria consist of the following 3 subgroups of disorders: HIV-associated ANI. For this category, the patient has to meet the following criteria: Cognitive impairment involving at least 2 cognitive domains (performance of at least 1 standard deviation [SD] below the mean for norms on neuropsychological tests). The cognitive impairment does not interfere with everyday functioning. HIV-1-associated MND. For this category, the patient has to meet the following criteria: Cognitive impairment involving at least 2 cognitive domains (performance of at least 1 SD below the mean for norms on neuropsychological tests). The cognitive impairment produces at least mild interference in daily functioning. HIV-1-associated dementia. This category requires that the patient has the following: Marked cognitive impairment involving at least 2 cognitive domains (performance of at least 2 SD below the mean for norms on neuropsychological tests). The cognitive impairment produces marked interference with day-to-day functioning.
In making the consensus diagnosis, at least 2 members of the panel had to agree that a patient had fulfilled Frascati criteria based on the performance on the psychometric instruments. We used the consensus method of arriving at diagnosis to improve the accuracy of our diagnosis. The panel was blind to results of the viral load and CD4 count at the time of making the consensus diagnosis.
Data Analysis
The data was analyzed using Statistical Package for Social Sciences version 15 for windows. Descriptive statistic was calculated for all variables. The student t test and chi-square test determined the relationship between cognitive impairment and the variables. The variables found to have significant association with cognitive impairment using bivariate analysis were further analyzed using multiple regression analysis to confirm the relationship. All tests of statistics were conducted at the 5% significance level.
Results
A total of 418 patients participated in the study. The mean (SD) age of the participants was 37.2 (± 9.3) years. The mean (SD) age of male participants was 44.7 (± 10.1) years, while that of female participants was 35.1 (± 7.8). The mean years of education were 7.9 (± 6.2) years. The use of psychoactive substance was uncommon, as only 25 (6.0%) and 6 (1.4%) patients used alcohol and cannabis, respectively. The details of sociodemographic characteristics of the participants are shown in Table 1.
Sociodemographic Characteristic of the Participants.
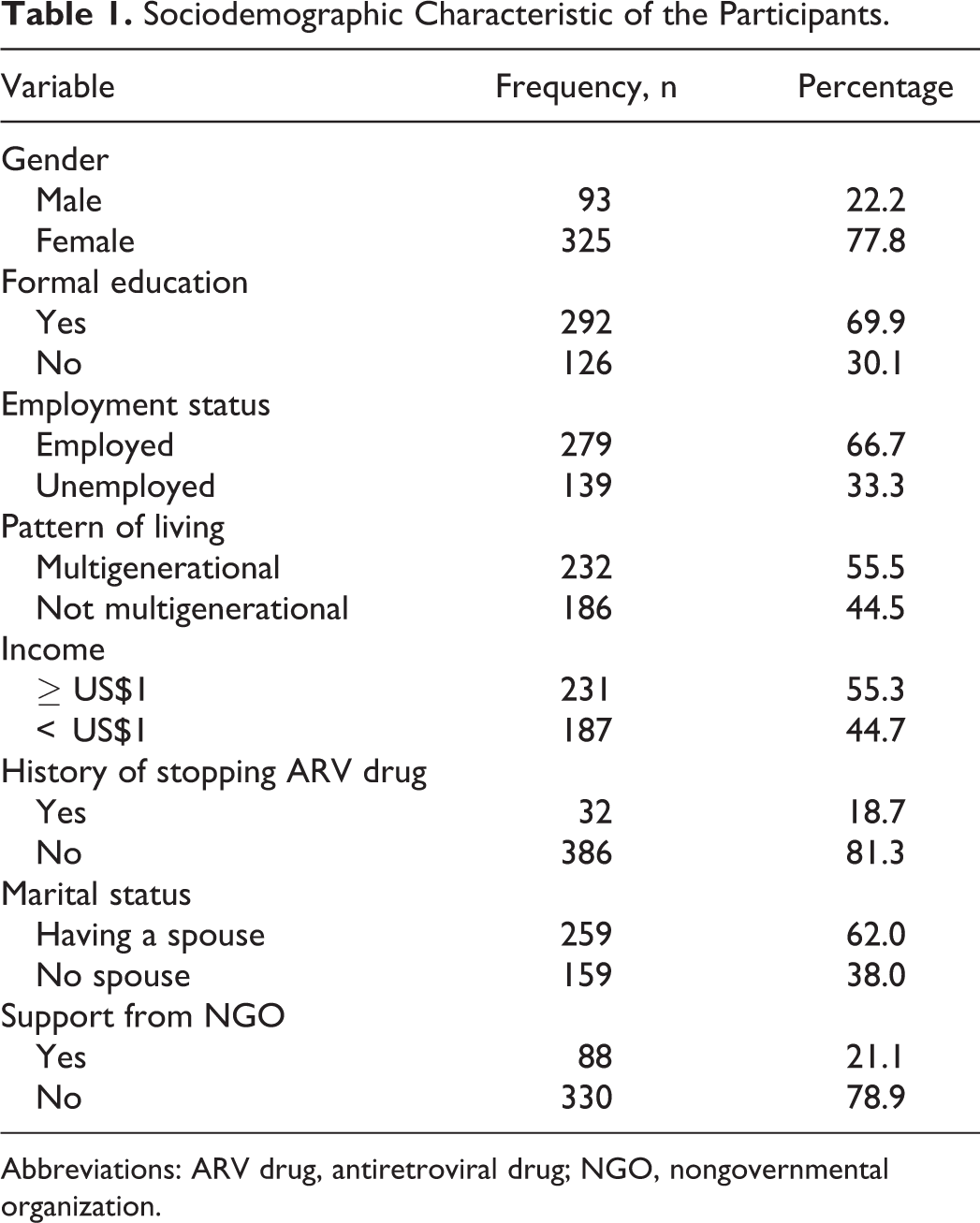
Abbreviations: ARV drug, antiretroviral drug; NGO, nongovernmental organization.
A total of 90 (21.5%, 95% confidence interval [CI] = 17.6%-25.4%) participants were found to have cognitive impairment. Based on the Frascati criteria, 13.3% (2.9%) had HAD, 42.2% (9.1%) had MND, and 44.4% (9.6%) had ANI, within this group. The relationship of sociodemographic characteristics of the participants and HAND is shown in Table 2. In the entire psychometric tests, it was found that the performance of the HAND group was significantly poorer compared with the cognitively normal group. The scores on the various psychometric instruments and cognitive status of the participants are shown in Table 3. In the initial bivariate analysis, cognitive impairment in the participants was significantly associated with CD4 count, viral load, age, education, days confined to bed, frequency of missing drug doses in a month, and history of stopping ART completely in the past. However, multiple logistic regression analysis confirmed that all these factors with the exception of age and frequency of missing drug dose are predictors of cognitive impairment in the participants. Summary of the multiple logistic regression analysis is shown in Table 4.
Relationship between Prevalence of HAND and Sociodemographic Characteristic of the Participants.a
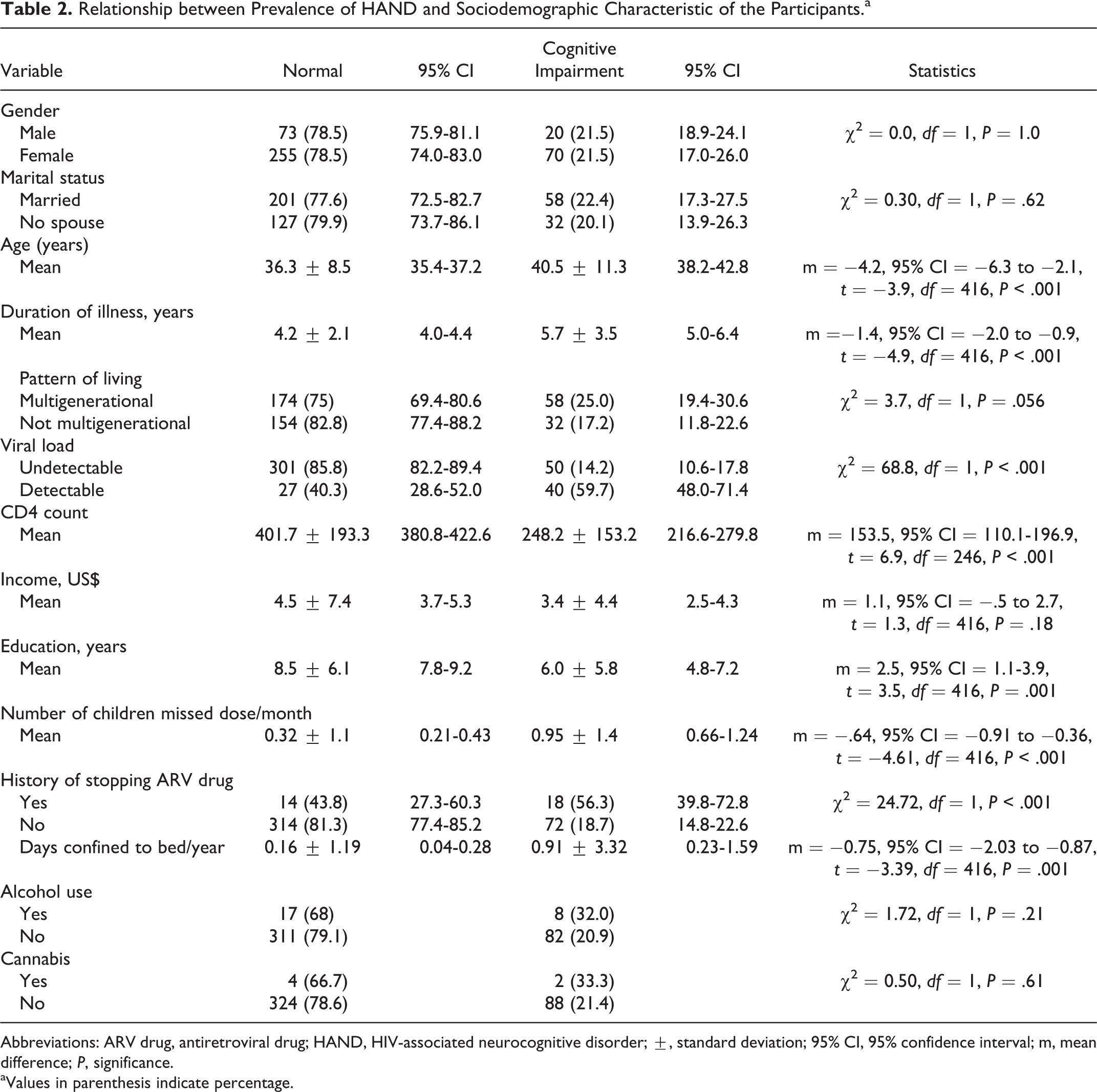
Abbreviations: ARV drug, antiretroviral drug; HAND, HIV-associated neurocognitive disorder; ±, standard deviation; 95% CI, 95% confidence interval; m, mean difference; P, significance.
aValues in parenthesis indicate percentage.
Relationship between Psychometric Instrument and Cognitive Status of the Patients.a
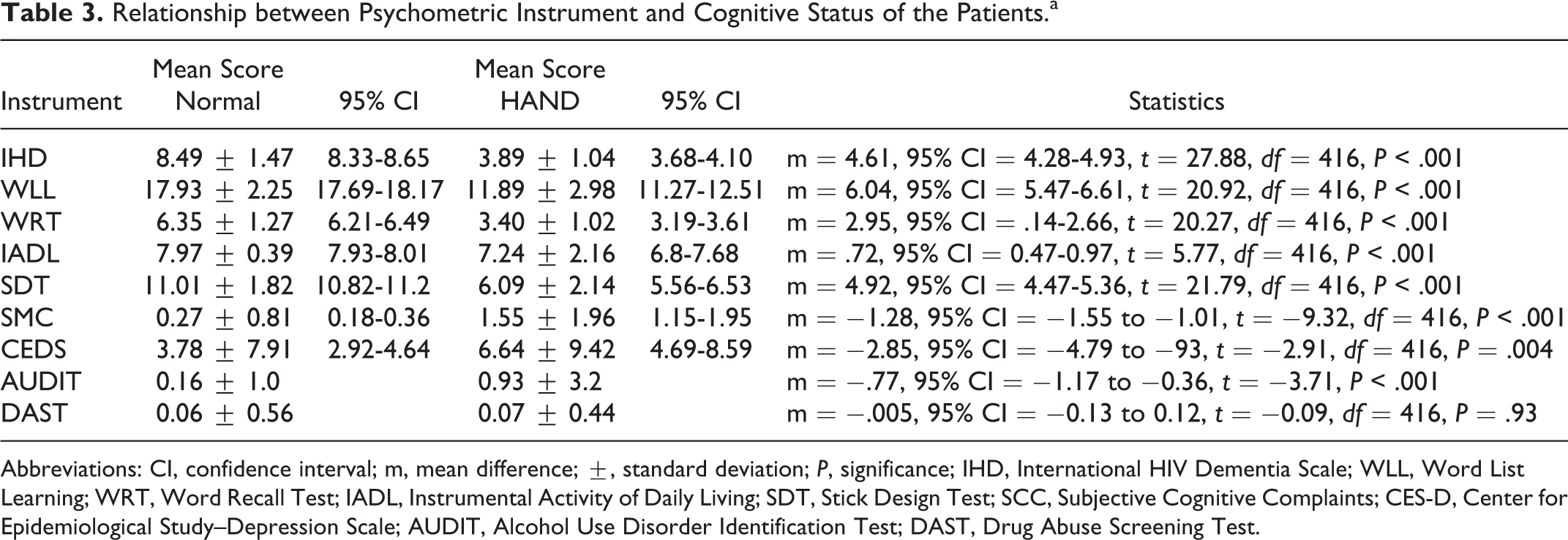
Abbreviations: CI, confidence interval; m, mean difference; ±, standard deviation; P, significance; IHD, International HIV Dementia Scale; WLL, Word List Learning; WRT, Word Recall Test; IADL, Instrumental Activity of Daily Living; SDT, Stick Design Test; SCC, Subjective Cognitive Complaints; CES-D, Center for Epidemiological Study–Depression Scale; AUDIT, Alcohol Use Disorder Identification Test; DAST, Drug Abuse Screening Test.
Summary of Logistic Regression.

Abbreviations: ART, antiretroviral therapy; CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
Sociodemographic Characteristics
The preponderance of female participants in this study indicates that HIV/AIDS infection is more common in women than in men in SSA. There are many reasons for this finding, which include cultural and economic factors that make women to have little control over sexual issues and reproductive health. 30 Another unlikely reason is that men do not come to the hospital either because of stigma or because they do not know their HIV status. Moreover, women are usually screened during antenatal visit as part of PMTCT, and when found to be positive they are referred for treatment. Lastly, the finding of this study that HIV infection is more common in women is similar to the observation made by National Agency for Control of AIDS in Nigeria. 12 The result of this study showed that more than a third of the participants were unemployed, had no education, and were living below the internationally acceptable level of poverty. This is not surprising as the level of poverty in Northern Nigeria outstrips that of the Southern region of the country. 14
Prevalence of Cognitive Impairment
The prevalence of HAND reported in this study is similar to that found in Zaire, which was demonstrated by World Health Organization in a multicenter study carried out in 5 countries. 21 The study reported a prevalence of 19% among symptomatic HIV-positive patients. 21 However, the prevalence of cognitive impairment in this study is lower to that reported by the earlier studies carried out in Africa. 2,6,31 A study conducted in Uganda prior to the formulation of the Frascati criteria reported that almost 78% of the participants had some form of cognitive impairment. 31 The observed differences may be attributed to the differences in methodology. The earlier studies relied mainly on the scores of IHDS for the diagnosis of cognitive impairment. While in this study the diagnosis of HAND was made using standard criteria and based on the consensus by a panel, it is likely to be more reliable. Another possible explanation for the difference in prevalence of cognitive impairment between this study and the earlier studies is the sub-clades of the virus. It had been shown that certain clades of the virus are more neuropathogenic and hence are more likely to cause cognitive impairment. 32 –34 In the East and Southern African regions, clades A and D are the predominant subtypes of the virus, with the latter associated with a higher risk of HAND. 33,34 A report from Nigeria indicated that clades A and G are the predominant subtypes of the virus. 35 However, the prevalence reported by this study is similar to that of Chan et al, a study of a South Asian population using Frascati criteria to make diagnosis. 36
Factors Associated with HAND
Our study found that the length of time since HIV diagnosis in the participants is a significant predictor of HAND. Central nervous system (CNS) invasion occurs very early in the course of HIV infection and the viral replication continues in the CNS despite the suppression of the plasma viral load with HAART. 37 As such longer duration of the illness would lead to more damage in the brain. On the other hand, HAART are neurotoxic, leading to brain damage. This has been demonstrated in an observational study involving a cohort of HIV-positive patients on HAART. 38 However, one can speculate that in this cohort HAART toxicity is unlikely due to the limited supply of drugs and close monitoring of the patients for signs of toxicity. Our study also found that low CD4 lymphocyte count and high detectable viral load while on ART are significant predictors of HAND. This is not in keeping with the findings of studies carried out in the era of HAART, thereby tending to report no relationship between current plasma viral load, CD4 count, and HAND. 6,36 History of stopping ART for a month or more in our study is a predictor of HAND in the participants. This is contrary to the finding of an observational cohort study of HIV-positive patients. 38 A possible reason is that participants in this study already have a preexisting neurological damage in view of the fact that brain damage occurs early in the course of HIV infection and also patients in Africa often start the treatment late. Low educational status is also a predictor of HAND in our cohort. This also has been reported by other studies and had been attributed to the ability of participants with higher education to perform better in the neuropsychological testing. 6,36 Low educational status might also affect the ability to access medical care at the appropriate time. Severity of illness among this study participants measured as days confined to bed in the last 1 year was also found to be associated with HAND. Similar observation was made by earlier reports among HIV-positive patients on HAART. 36 The lack of association between HAND and age among this study participants was not as reported by other studies and can be attributed to the relative younger age of this cohort. 31 One important finding of this study is the lack of association between psychoactive substance use in this cohort and HAND. This might be attributed to the sociocultural practice of the area that frowns at alcohol and drug uses, as few numbers of the participants were using psychoactive substances.
Overall it would appear that the differences between this study and previous ones in Africa and elsewhere can be explained by demographic, clinical variables, and method of diagnosis. Some of the demographic variables are modifiable, but further studies are necessary to determine the relationship between clades A, C, and G of the virus to HAND.
Limitations
This is a study involving patients receiving ART carried out in tertiary health facility and as such might not be applicable to the general HIV-positive patients in Nigeria. However, our center provides care for large proportion of patients in Northern Nigeria and the study might give an insight to the problem of HAND in Nigeria. The possibility of selection bias in this study was minimized, considering that the participants were selected using a simple random sampling (balloting), as all patients who fulfilled the inclusion criteria had equal chances of participating in the study. We also did not exclude participants with significant depressive symptoms or cardiovascular disease in the study. Lastly, we used culturally and educationally fair psychometric instruments as minimizing measurement bias might be associated with such assessment.
Conclusion
Using the standard criteria, it was found that the prevalence of HAND is lower than that reported earlier in Africa and the associated factors also vary from that of earlier studies.
Footnotes
Acknowledgments
The authors are grateful to all the participants for volunteering to take part in the study. We are also grateful to the Ibadan-Indianapolis Dementia Project, Ibadan site, for logistic support.
Authors’ Note
AJY was involved with the conceptualization, study design, data collection, analysis, and writing of the article; AH was involved with the study design, data collection, analysis, and writing of the article; AIM was involved with the study design, data collection, analysis, and writing of the article; HMM contributed to the study design, analysis, and writing of the article; AMS contributed to the study design, data collection, analysis, and writing of the article; and OB contributed to the conceptualization, study design, analysis, and writing of the article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Fogarty International Center or the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by Grant Number R24TW008878 from the Fogarty International Center.