
Abstract
Objective:
Given the emerging data suggesting the key role of brain-derived neurotrophic factor (BDNF) in the immune system, we assessed longitudinally whether BDNF depletions induced by hazardous alcohol use (HAU) would impact a response to antiretroviral therapy (ART).
Methods:
In a prospective single-site cohort, virological and immunological responses to ART in 200 hazardous and 200 nonhazardous users were obtained, along with plasma BDNF levels.
Results:
Hazardous drinkers were more likely to have BDNF levels <4000 pg/mL (odds ratio [OR] = 1.6, P = .01). Participants with BDNF <4000 pg/mL were less likely to have CD4 counts of more than 500 cells/mm3 (P = .02) and to achieve viral suppression over the follow-up period (OR = 1.5, P = .03). Multivariate analysis confirmed the significant role of HAU and low BDNF in predicting viroimmune responses.
Conclusion:
Hazardous alcohol use was associated with BDNF alterations, which in turn were linked to a limited response to ART in terms of viral suppression and CD4 count improvements.
Keywords
Introduction
Antiretroviral therapy (ART) has been one of the greatest advances in the fight against the HIV. When a complete virologic suppression (viral load [VL] <400 copies/mL by 24 weeks or <50 copies/mL by 48 weeks) is attained, people living with HIV (PLWH) benefit from immune reconstitution and AIDS-free survival. 1,2 Unfortunately, incomplete suppression of viral replication, which is present in a sizable proportion of cases, results in immune exhaustion, the emergence of drug resistance, and ultimately in increased morbidity and mortality. 2 Even among patients reaching these virologic targets, substantial interindividual differences in immune responses occur among them, suggesting that other factors may be involved. 3 Our group, along with others, has demonstrated that hazardous alcohol use (HAU) influences CD4 count recovery and clinical outcomes. 4 Our previous studies indicated that alcohol decreases the size and cellularity of the thymus, leading to low total numbers of peripheral T cells. 4,5 Others have demonstrated only small gradual increases in CD4 counts that largely remained less than 500 cells/mm3. 6 -8 However, the thymus model only partially explains the impaired recovery of hazardous alcohol users living with HIV (HAULWH), indicating the need to look for additional factors.
As indicated by many studies, brain-derived neurotrophic factor (BDNF) is a neutrophil mostly known for its role in the central nervous system (CNS) that is affected by HIV. 9 -11 Brain-derived neurotrophic factor plays an important role in a variety of brain functions, including the lasting potentiation of synaptic efficacy that modulates brain plasticity. Brain-derived neurotrophic factor is involved in learning and memory processes and has been closely associated with cognitive deficit in HIV, aging, and neurodegenerative diseases. 9 -11 Until recently, BDNF has been linked with the immune system, but several lines of evidence indicate that BDNF plays important roles in proliferation, apoptosis, and T-cell survival. 12 -14 Yet, its role in CD4 count depletion or immune replenishment under ART is unknown. Of interest is the study by Avdoshina and colleagues 15 who did not relate the findings to genetic mutations, nor to platelet counts. However, their sample was small, and information on platelet counts was not provided. Although evidence that gender can impact BDNF levels, 16 the authors failed to analyze gender differences in BDNF levels.
In light of these findings, we examined whether a decrease in BDNF could explain the reduced T cell counts and the excessive VL observed in PLWH (with comorbidities such as HAU and/or thrombocytopenia [TCP]). Because the Platelets Mediating Alcohol and HIV Damage Study (PADS) includes a gender-diverse sample of participants, with substantial variation in alcohol use, we were afforded a valuable opportunity to explore the multifaceted associations among alcohol use, BDNF, gender, and immune responses to ART.
Methods
Sampling
The Platelets Mediating Alcohol and HIV Damage Study PADS is a large, single-site multiethnic cohort, consisting of 400 PLWH who are at least 18 years old and younger regular care at Miami’s primary open-access public health system. Patients were recruited via flyers, personal contact at the clinics, or calls to our office to schedule appointments. Recruitment and follow-ups took place in the period between June 2010 and June 2012. Our choice of PLWH in an open-access public health system with standard treatment protocols was purposefully designed to minimize social, medical, and treatment inequalities.
Participants were dichotomized as hazardous and non-HAUs, based on self-reports of alcohol intakes. Alcohol consumption scores were computed by averaging cross products of quantity and frequency of beer/wine and hard liquor reported on the Alcohol Use Disorders Identification Test, developed by the World Health Organization (WHO) as a simple method of screening for excessive drinking and to assist in brief assessment, and the Alcohol Dependence Scale responses. 17,18 Then, based on the National Institute of Alcohol Abuse and Alcoholism guidelines criteria, men who reported >14 drinks/week or >4 drinks in 1 day and women >7 drinks/week or >3 drinks in 1 day were classified as HAU, while those who reported fewer drinks were categorized as non-HAU. 19
The group was chosen to represent relatively “pure” alcohol users with minimal drug use and without major confounding factors. Nonambulatory patients and those presenting major medical comorbidities such as major neuropsychological (ie, active CNS opportunistic infection, tumors, and developmental disorders), immune-based (ie, malignancies and autoimmune diseases), and chronic diseases (renal failure) were excluded. In addition, individuals who had cirrhosis, active viral hepatitis, or liver enzymes and who were 2 standard deviations (SDs) above the normal values were not eligible to participate in the study. To reduce the confounding effects of illicit drug use, the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition, Text Revision) questionnaire was applied, and those participants who were dependent on drugs or injecting illicit psychoactive substances were also excluded. Otherwise, the patients were enrolled.
The Platelets Mediating Alcohol and HIV Damage Study was approved by the Central Governing Institutional Review Boards at Florida International University and University of Miami. The study was conducted according to the principles expressed in the Declaration of Helsinki. Those participants who provided written informed consent were consecutively enrolled and followed over a period of 6 months.
Laboratory Outcomes
Blood was drawn from fasting patients to best evaluate the immunological, hematological, and platelet-associated factor profiles. Blood samples were collected and processed within 6 hours. Isolated peripheral blood mononuclear cells were prepared for 4-color direct immunofluorescence procedures (Becton Dickinson, San Jose, California). Flow cytometry quantified the percentage and absolute numbers of T-lymphocyte subpopulations CD3/CD4 and CD3/CD8. A good immunological response was defined as having a CD4 count of more than 500 cells/mm3 or as a gain in CD4 count ≤50 cells/mm3 from week 0 to week 24.
HIV viral burden was quantified using the Amplicor HIV monitor test (Roche Diagnostic System, Indianapolis, IN). The lower threshold for detection at the time of the study was 50 copies/mL. Virological success was defined as achieving undetectable VL. Poor virological response was defined as a plasma VL >2.7 log10 copies/mL at week 24.
Sample Characteristics by BDNF Groups.

Abbreviations: BDNF, brain-derived neurotrophic factor; AST, aspartate aminotransferases; ALT, alanine aminotransferases.
Multivariate Analyses Examining Predictors of CD4 Counts after 24 Weeks of ART.a

Abbreviations: ART, antiretroviral therapy; Std, standard; Sig, significance; BDNF, brain-derived neurotrophic factor; CDC, US Centers for Disease Control and Prevention; TCP, thrombocytopenia.
a The results presented here emerged from final multivariate regression analyses. The model was adjusted for covariates that in previous studies have been related to CD4 counts after ART (ie, age, race, gender, income, albumin, anemia, TCP, and liver enzymes), HIV factors (viral load, CD4, CDC stage, years living with HIV, ART, and adherence).
Brain-Derived Neurotrophic Factor
The circulating levels of BDNF were selected because prior studies have demonstrated that, although different from those in the cerebrospinal fluid (CSF), they are correlated with CSF measures in other CNS diseases. 20 To obtain platelet-poor plasma (PPP), the blood samples were collected in EDTA-coated tubes (plasma; BD Diagnostic Systems, New Jersey) and stored on ice. Plasma was separated by centrifugation at 40°C for 15 minutes at 1500g. This plasma was again recentrifuged at 10 000g and the aliquots of PPP were stored in polypropylene tubes at −80°C until assayed. The BDNF levels in PPP were measured using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (R&D System), according to the manufacturer’s instructions. However, during the standardization a sizable proportion of PLWH had a BDNF value of 4000 pg/mL (ceiling effect), so the samples were 20-fold diluted. The concentration of BDNF in plasma was calculated based on a standard curve. The minimum detectable dose of BDNF is typically less than 62 pg/mL. The repeatability of the BDNF ELISA as measured by intra-assay precision was 6%, and the reproducibility as measured by interassay precision was 9%. Coefficient of variation (CV) was 7.9 (CV% = SD/mean × 100%).
Covariates
Upon entry into the study, data were collected at baseline and after 24 weeks by using standardized questionnaires; sociodemographic (age, gender, income, and race/ethnicity) and medical history information and the following covariates were obtained (ie, AIDS-defining conditions = yes/no and US Centers for Disease Control and Prevention [CDC] clinical staging): complete blood counts (thrombocytopenia was defined as platelet counts of less than 150 × 103 cells/mm3 [41-42] and a biochemical profile (calcium, sodium, potassium, albumin, glucose, lipids, kidney, and liver function). HIV-related and not-related treatments (ie, start date and discontinued) were obtained and confirmed with the pharmacy and medical records. An AIDS Clinical Trial Group (ACTG) self-reported adherence questionnaire was used at each visit. Based on the missed doses per week and during the weekend, the percentage of adherence was calculated at baseline and at the follow-up visit.
Statistical Analyses
The data were analyzed using SAS version 8 and SPSS version 19, and P values <.05 were considered to be statistically significant. The normality of the distribution of primary outcomes of interest was examined with a normal probability plot. Viral load was log transformed to correct skewness. Following descriptive statistical analyses, the mean variables were compared using Student t test and one-way analysis of variance procedures. Correlations among the main variables of interest were examined with Pearson coefficients. Additionally, chi-square analyses were performed to compare the proportions for gender and race. Univariate analyses were used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs). Logistic regression analyses were used to evaluate the effects of alcohol (continuous or as hazardous versus nonhazardous), thrombocytopenia (counts and dichotomized as thrombocytopenia <150 000 versus normal platelet counts), age (continuous and dichotomized at age 50 years), and gender.
The multivariable models aimed to predict VL and CD4 count status at the last visit and included all covariates whose likelihood ratio for P value from the univariate analyses was <.1. Although no significant differences were observed between groups for education level or CDC status, both variables were controlled for in the final analyses. In addition, other potential predictors (ie, gender, race/ethnicity, and body mass index) were selected on the basis of the literature and were added to the model. 6 Although the nadir CD4 count has been recommended as a preferable measure of disease severity, data were not available for most participants and therefore the baseline CD4 counts were used. More parsimonious models were explored by removal of covariates, one at a time, starting with the covariate with the largest P value, until the final full model was achieved.
Results
Brain-Derived Neurotrophic Factor and Sample Characteristics
Among the 400 PLWH, a wide concentration range of BDNF was found in circulation, from 298 to >20 000 (mean 8384 ± 6366 pg/mL). Based on our prior studies, participants were dichotomized as more than and less than 4000 pg/mL: low-BDNF group for those with values <4000 pg/mL and high-BDNF group for those with values >4001 pg/mL. To permit a better definition, a brief characterization of the different groups was performed.
As depicted in Table 1, the BDNF levels differed by gender, with women exhibiting the highest levels (9958.9 ± 6578 versus 7470 ± 6068 pg/mL, P = .001). Participants in the low-BDNF group were twice as likely to be male (95% CI: 1.4-3.4, P = .003). Although at first glance age was not significantly different, we pursued additional analyses as prior literature indicated an age effect over BDNF. Indeed, PLWH aged 50 years and older had significantly higher levels than that of their younger counterparts (11 207 ± 8790 versus 8369 ± 6529, P = .003). Race distribution was similar, though a slightly (nonsignificant) higher proportion of Hispanics were in the low-BDNF group. Overall parameters, such as albumin and liver enzymes, were similar between the groups.
Notably, participants in the low-BDNF group were more likely to be (OR = 1.6, 95% CI: 1-2.4; P = .01) and to have thrombocytopenia (OR = 3; 95% CI: 1-7.8, P = .04). While in those who had less than 3 drinks per day, no significant differences were observed, beyond this the threshold differences were always statistically significant (see Figure 1). However, it needs to be recognized that not all HAUs exhibited low BDNF levels.
Brain-Derived Neurotrophic Factor and T Cells
Participants had open access to antiretroviral (ARV) medicat, and all received a prescription for ART. Most were receiving Truvada (44%) followed by Atripla (22%) alone or in combination with Norvir (32%) or Kaletra (13%). At the follow-up visit, all but 2% of the sample were not taking ART. Notably, all non-HAUs were taking ART as prescribed. Adherence, as measured by the ACTG questionnaire, was similar between the groups and was high during the week (93%) and more limited during weekends (83%, baseline). Adherence was also similar between the BDNF groups (85% versus 87%).
Since little is known concerning the plausible impact of ART on BDNF, we first compared the values between those few who were prescribed but were not taking their ARV medications with those receiving treatment. Analyses indicated no significant differences in the BDNF levels between the treatment groups (8712 ± 6917 versus 7146 ± 4526 pg/mL, P = .2). Despite no differences in treatment or adherence, we the relationship between BDNF and the cellular immune response. Correlations between plasma BDNF and T-cell parameters were all significant. A moderate statistically significant correlation was found between BDNF and CD3 counts (r = .345, P = .0001). The association between BDNF levels and CD4 counts was also significant (r = .355, P = .0001), but was less strong with CD8 counts (r = .228, P = .0001).
At baseline, the low-BDNF group exhibited significantly lower CD3 counts than that of the high-BDNF group (1087.5 ± 482.8 versus 1426.5 ± 542.1 cells/mm3). Then, analyses were focused on determining whether, during ART, BDNF deficiencies have an impact on CD4 count status. As shown in Table 1, the low-BDNF group exhibited significantly lower CD4 counts (310.7 ± 219 cells/mm3) than those in the high-BDNF group (477.5 ± 299 cells/mm3, P = .0001). Significant group differences in CD8 counts were also observed; patients in the low-BDNF group exhibited lower CD8 counts. Then, CD4 counts of more than 500 cells/mm3 were used as a proxy of immune response for those under treatment. Univariate analyses indicated that PLWH with low BDNF were 3 times less likely to have a CD4 count of more than 500 cells/mm3 (OR = 3.3, 95% CI: 1.8-6.3, P = .0001).
Since gender differences in the BDNF levels were evident, we pursued gender analysis. At baseline, women had a mean CD4 count of 508 ± 323 cells/mm3 compared with 393 ± 267 cells/mm3 for men (P = .001). Indeed, women were twice as likely than men to have a CD4 count of more than 500 cells/mm3 (OR: 2.3, 95% CI: 1.4-3.4, P = .0001).
Lymphocyte profiles were available at the 6-month follow-up, and a similar trend was observed: the low-BDNF group exhibited even lower CD4 counts (287.9 ± 181 cells/mm3) compared to those in the high-BDNF group (463.6 ± 300 cells/mm3, P = .0001). In adjusted regression models, the low-BDNF group had greater odds of not increasing their T-cell counts during the 6 months of receiving ART (relative risk [RR] = 11, P = .02). Differences in CD8 counts were no longer significant.
The difference in CD4 count response between men and women also increased with time on ART. At the 6-month visit, men exhibited significantly lower CD4 counts when compared to women (365 ± 253 versus 521 ± 313 cells/mm3, P = .0001). They also exhibited lower CD8 counts (869.0 ± 437 versus 911.5 ± 503 cells/mm3, P = .004).
Brain-Derived Neurotrophic Factor and VL
The average VL burden was 36 849 ± 8935 copies/mL (log = 2.7 ± 1.3). Notably, nearly half of the study population had a VL of less than 400 copies/mL. Viral burden was not significantly different between genders, but this time females exhibited slightly higher burden than males did.
To further investigate the relationship between BDNF levels and VL, we started by correlating the 2 variables, and analyses demonstrated a significant relationship between plasma BDNF and HIV VLs (r = −.225, P = .0001). The low-BDNF group had higher VL (74,078 ± 35,489 compared to.…26,813 ± 7,015 3.2 ± 1.3 log) compared to those in the high-BDNF group (log = 2.6 ± 1.3, P = .004). In adjusted regression models, the low-BDNF group had greater odds of having detectable VLs compared to those in the high-BDNF group (RR = 1.35, 95% CI: 1.04-1.75; P = .03).
At the follow-up visit, the mean VL of the sample was significantly reduced to 21 550 ± 5638 copies/mL. Undetectable VL were achieved by 66% of the sample at the last visit. Paired t-test analyses indicated that being in the low-BDNF group was associated with less improvement in CD4 count. Additional analyses indicated that the low-BDNF group was less likely than patients in the high-BDNF group to achieve viral suppression during the follow-up period (OR: 1.5, 95% CI: 1-2.2, P = .03). This suggests that BDNF could, in part, explain the incomplete viral suppression.
Multivariate
To examine the independent effect of alcohol and BDNF levels on CD4 count and VL, at the last visit we used a multivariate analysis to adjust for potential confounders, such as sociodemographic (ie, age, education, gender, race, albumin, and liver enzymes), HIV factors (VL, CD4 count, CDC stage, years living with HIV, ART, and adherence), and those variables that were significant in the simple regression analyses (ie, thrombocytopenia [TCP], alcohol use, and BDNF). After removal of covariates with no significant P value, these analyses indicate that alcohol use and BDNF alterations are significant predictors of viral-immune status (see Tables 2 and 3).
Multivariate Analyses Examining Predictors of HIV Viral Load.a
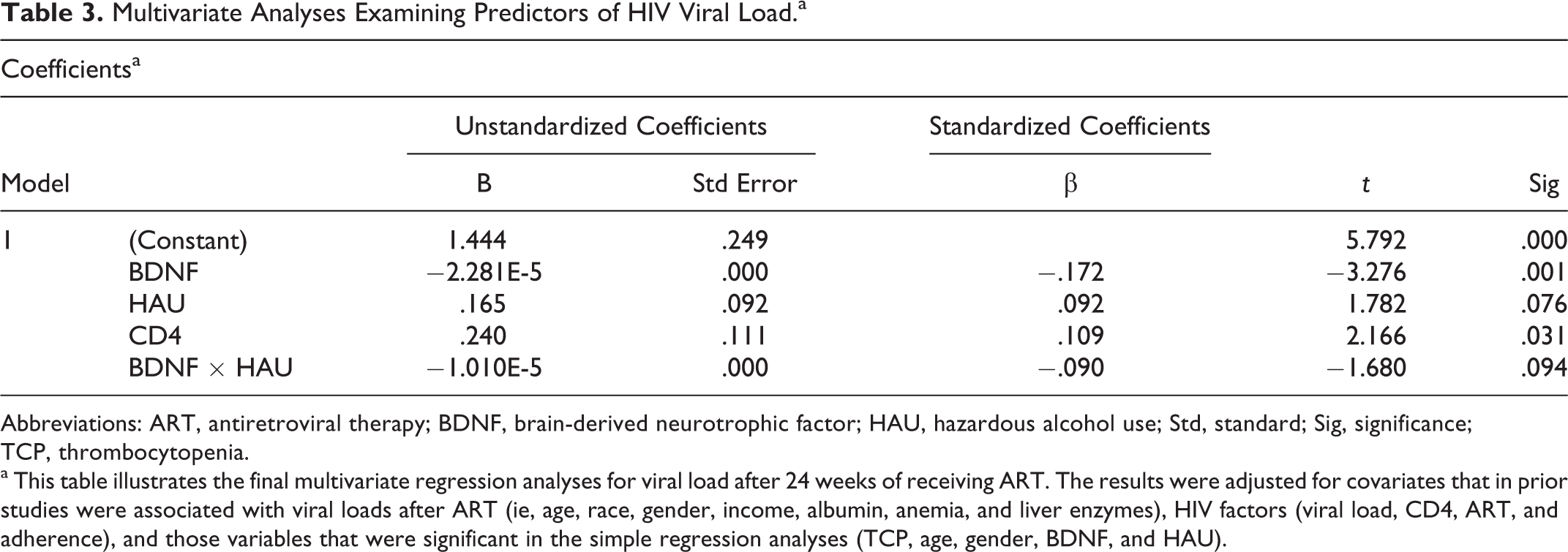
Abbreviations: ART, antiretroviral therapy; BDNF, brain-derived neurotrophic factor; HAU, hazardous alcohol use; Std, standard; Sig, significance; TCP, thrombocytopenia.
a This table illustrates the final multivariate regression analyses for viral load after 24 weeks of receiving ART. The results were adjusted for covariates that in prior studies were associated with viral loads after ART (ie, age, race, gender, income, albumin, anemia, and liver enzymes), HIV factors (viral load, CD4, ART, and adherence), and those variables that were significant in the simple regression analyses (TCP, age, gender, BDNF, and HAU).
The first regression model examined the predictors of CD4 counts at the last visit, and the R 2 was .24, indicating that the model predicted approximately 24% of the variance in the CD4 counts. The model indicates that no demographic or disease-specific variables except for gender and VL were associated with immunologic response. Alterations in BDNF and the number of drinks consumed per day were significantly associated with VL at the last visit. A trend was evident for older age (P = .06).
The second model (see Table 3) was aimed to predict VL status at the last visit, and the R 2 was .25, indicating that the model predicted approximately 25% of the variance in viral status. In this fully adjusted model (ie, age, education, gender, race, albumin, liver function tests, anemia, TCP, CD4 count, CDC stage, years living with HIV, ART, and adherence), BDNF alterations and being an HAU were significantly associated with virological status during treatment. Low CD4 counts at baseline were also significant predictors of VL at the end of the study. As depicted in the Table 3, the interaction between HAU and BDNF was not significant.
Discussion
The present investigation began by demonstrating that the changes in the T-cell compartment are generally widely variable and confirmed that HAU are more likely to exhibit poor immunological responses. Yet, the mechanisms underpinning these differences remain to be fully elucidated. In this regard, this article is unique in demonstrating the role of BDNF over a wide range of key immunological parameters in PLWH receiving ART. First, our analyses support the hypothesis that reduced levels of BDNF may be a risk factor for incomplete immunological responses to ART. Furthermore, it contributes new pieces of information by demonstrating that the effects are not global, as we observed significant effects on CD3, CD4, and B cell counts, but not on CD8 counts. Second, our data also demonstrated that in vivo BDNF plays an important role in viral control. These findings may contribute new insights into our understanding of the immune alterations associated with HIV. They are clinically relevant, given that a sizable proportion of individuals receiving highly active ART (HAART) do not fully respond to treatment. 21 In our opinion, our results are also significant because they open a potential therapeutic avenue to be targeted mainly to address poor virological and immunological responses. Hence, BDNF can be seen as a potential therapeutic immune agent and not only neuroprotective.
Data also demonstrated that women achieved better immune response to ART. Notably, analyses demonstrated that BDNF is also significantly higher among females, suggesting that this biological difference may indeed be a factor mediating gender differences. The gender-based difference in immune reconstitution has been inconsistently described in previous studies. Some studies are showing a better female immune reconstitution, 22,23 whereas 2 literature reviews concluded that there are no gender differences regarding virological and immunological responses to ART. 24 -26
Our data, indicating a close relationship between BDNF and immune status, are in accord with laboratory experiments, suggesting that BDNF could be involved in promoting the resilience of T cells. Given our results, and the well-known antiapoptotic effect of the neurotrophins for T cells, 28 we may speculate that a decrease in BDNF could be one of the pathological mechanisms used by HIV-1 to induce the apoptosis of T cells. Although our data suggest that recovery of CD4 counts in individuals receiving HAART is related to BDNF status, the study focused only on quantitative analyses. Functional assays will be needed in future research to ascertain whether the quantitative recovery of the CD4 T-cell compartment that we observed by phenotypical measures also leads to improvements in T-cell function. Results from the multivariate model indicating that BDNF is related to VL are congruent with BDNF’s known effects.
During ART, patients in the low-BDNF group had higher VL compared to those in the high-BDNF group. This is in line with the experimental studies in which BDNF downregulates CXCR4 and 5 expressions, the 2 coreceptors implicated in HIV infection. 9 -11,27 These findings explain why blunted response to HAART was observed in these individuals.
Nevertheless, our results had 2 limitations: participants were restricted to those followed at University of Miami/Jackson Memorial facilities and we cannot establish causality. Nonetheless, these results may have important research, clinical, and therapeutic implications. They improve our understanding of the neuroimmune system. By identifying those HIV-infected individuals at risk for incomplete ART responses, such as HAULWH and those with decreased BDNF levels, the study may permit early clinical follow-ups and interventions. The findings may also guide the development of future adjuvant therapies.

Levels of brain-derived neurotrophic factor (BDNF) by amounts of alcohol consumption.
Footnotes
Authors’ Note
The study was run at the Clinical Research Center, University of Miami Miller School of Medicine, Miami, FL 33136, USA. This research was presented at the International Conference on HIV/AIDS, STDs and STIs during October 24-25, 2013 at Holiday Inn Orlando International Airport, Orlando, FL, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article: The grant was funded by the NIAAA R01 AA018095-01A1 and the NIAAA 1U24AA022002-01 grants.