
Abstract
Background:
Tuberculosis (TB) remains the most common cause of death in people living with HIV/AIDS. The aim of the present study was to identify predictors of mortality in TB/HIV-coinfected patients.
Methods:
We conducted an unmatched case–control study among a cohort of TB/HIV-coinfected adults who were on antiretroviral therapy (ART). Cases comprised 69 TB/HIV-coinfected patients who died during this period. For each case, we selected 3 (207) TB/HIV-coinfected patients who were alive during the end of the follow-up period.
Results:
Male sex (odds ratio [OR] = 2.04, 95% confidence interval [CI]: 1.04-4.02), being bedridden at enrollment (OR = 2.84, 95% CI: 1.17-6.89), and cough of more than 2 weeks during initiation of ART (OR = 4.75 95% CI: 2.14-10.56) were the best predictors of mortality among TB/HIV-coinfected patients.
Conclusion:
Mortality among TB/HIV-coinfected patients accounted for a considerable number of deaths among the cohort. Patients with cough at ART initiation and with poor functional status should be strictly followed to reduce death.
Introduction
Tuberculosis (TB) remains the most common cause of death in people living with HIV (PLHIV). Compared to people without HIV, PLHIV have a more than 20-fold increased risk of developing TB. 1
TB/HIV coinfectioned remains the leading cause of mortality among PLHIV in sub-Saharan Africa. 2-4 In 2008, TB accounted for 23% of AIDS-related deaths and of the estimated 9.4 million incident cases of TB, and 1.4 million were PLHIV. 5-6 Tuberculosis has been identified consistently as one of the predictors of mortality among PLHIV. 1,7 In a study in Uganda, predictors of mortality among TB/HIV-coinfected individuals starting antiretroviral treatment (ART) included male sex, anergy to tuberculin skin test, and a positive serum cryptococcal antigen result. 8 In Ethiopia, TB is a leading cause of hospitalization and the third cause of hospital death. 9,10 The country is ranked seventh among the 22 high-TB-burden countries. 5,11 In 2009, the case detection rate of all forms of TB and smear-positive TB was 50% and 34%, respectively. 11 The low TB detection rate, 11 the high burden of TB/HIV coinfection, 9 and the emergence of multidrug resistance TB pose serious challenges for the TB control program in Ethiopia. 11 Since 2007, the country has been implementing TB/HIV collaborative activities such as screening of patients with TB for HIV, intensified TB case finding among HIV-infected patients, and joint coordination of the control of the 2 diseases. 11
According to a study conducted in southern Ethiopia among 185 patients in the pre–highly active ART (HAART) cohort and 180 patients in the HAART cohort, the mortality rate was 15.4 per 100 person-years of observation (PYO) in the HAART group and 58.1 per 100 PYO in the pre-HAART group. 12 In another study in Addis Ababa among patients taking HAART, the mortality rate was 6.9% (incidence 2.8 per 100 PYO) and 57% of deaths occurred in the first 6 months of HAART initiation. 13 In Eastern Ethiopia a recent study found a mortality of 5.9% among patients taking HAART. 14 In a study conducted among 6450 registered patients with TB, a 3.7% mortality rate was reported. More than 75% of these deaths occurred within 8 months of treatment initiation. 15
So far, in Ethiopia no study has investigated the predictors of mortality among TB/HIV-coinfected patients. Hence, an understanding of the predictors and prognostic factors would allow closer follow-up and more targeted interventions in high-risk patients, thus reducing excessive mortality. The aim of the present study was to identify the predictors of mortality among TB/HIV-coinfected patients who were taking ART in a hospital in Southwest Ethiopia.
Methods
Setting
This study was conducted at Jimma University Specialized Hospital in Southwest Ethiopia. The hospital serves as a teaching and referral center for a population of 10 million people in Southwest Ethiopia. The hospital has a separate unit for the ART program since June 2003. This study included all adult patients with HIV infection ever enrolled for ART since June 8, 2003, to August 14, 2009. During the study period, a total of 4499 adults were enrolled for HIV care at the ART clinic and 188 of them died. In all, 2355 patients were put on HAART. All patients in HIV care are screened for TB regularly, and in the same period, 919 patients were identified to be TB/HIV coinfected. Among 919 TB/HIV-coinfected patients, 69 deaths were registered. Diagnoses of TB and HIV at baseline were based on national guidelines. 16 Smear microscopy was the major diagnostic tool for pulmonary TB. Tuberculosis lymphadenitis was diagnosed based on clinical parameters and cytological examination obtained by fine needle aspiration. TB is screened among HIV-infected patients by a thorough symptom screening. During each clinic visit, patients were thoroughly assessed by trained nurses for drug side effects, general health status, and presence of symptoms of opportunistic infection including TB.
This study was approved by the ethical committee of Jimma University. All the data accessed in the course of the study were kept confidential, and no names or other individual identifiers were obtained during data collection.
Design, Population, and Data Collection
We conducted an unmatched case–control study. Cases were 69 TB/HIV-coinfected adults (≥15 years) who were on ART and died during the study period. For each case, we selected 3 TB/HIV-coinfected patients who were on ART and alive by the end of the follow-up period. The controls were selected by random sampling technique using the unique identification number of the ART clinic. Data were collected using a structured and pretested questionnaire by 5 trained resident physicians. The questionnaire was adopted from the nationwide and uniformly used patient registration and follow-up form of HIV-infected clients in Ethiopia. The content of the questionnaire included sociodemographic information, clinical characteristics of patients, and TB/HIV status and outcomes of therapy.
Data Analysis
Data were edited, cleaned, coded, and entered into a computer and analyzed using Statistical Package for the Social Sciences version 16.0 for Windows. Descriptive statistics was done to determine the specific mortality rate. Bivariate analysis was done to determine associations between explanatory variables and the outcome variable (death). Logistic regression models were performed to identify predictors. New TB diagnosis at each follow-up was also measured. All explanatory variables that were associated with the outcome variable in bivariate analyses with a P value of .05 or less were included in the multivariate logistic models.
Results
Of the total cohort of patients on ART (n = 2355), 919 were diagnosed to be TB/HIV coinfected. Of the 188 deaths registered in the study period, 69 (36.7%) were TB/HIV-coinfected. All 69 deaths and 207 controls were included in the study. Of the 69 TB/HIV-coinfected deaths, 43 (62.3%) had pulmonary TB, 14 (20.3%) had extrapulmonary TB, 3 (4.3%) had disseminated TB, and for 9 (13.0%) the type of TB was not recorded.
Of the 69 deaths, 33 (47.8%) occurred in the first 3 months of ART initiation, 19 (27.5%) between 4 and 6 months, and the remaining 17 (24.6%) between 7 and 48 months. Of the 69 TB/HIV-coinfected deaths, 57 (82.6%) were diagnosed with TB before ART initiation, 11 (15.9%) were diagnosed with TB in the first 6 months of ART initiation, and 1 case was diagnosed afterward. Of the 69 deaths, 20 had a previous history of TB treatment before their current TB disease.
Cases were slightly but not significantly older than controls (P = .067; Table 1). The percentage of men was higher among cases than controls (P = .015). More cases were married compared to controls (P = .009). There was no significant difference in the educational status of cases and controls.
Comparison of the Sociodemographic Characteristics of Cases with TB/HIV-Coinfection and Controls in Southwest Ethiopia.
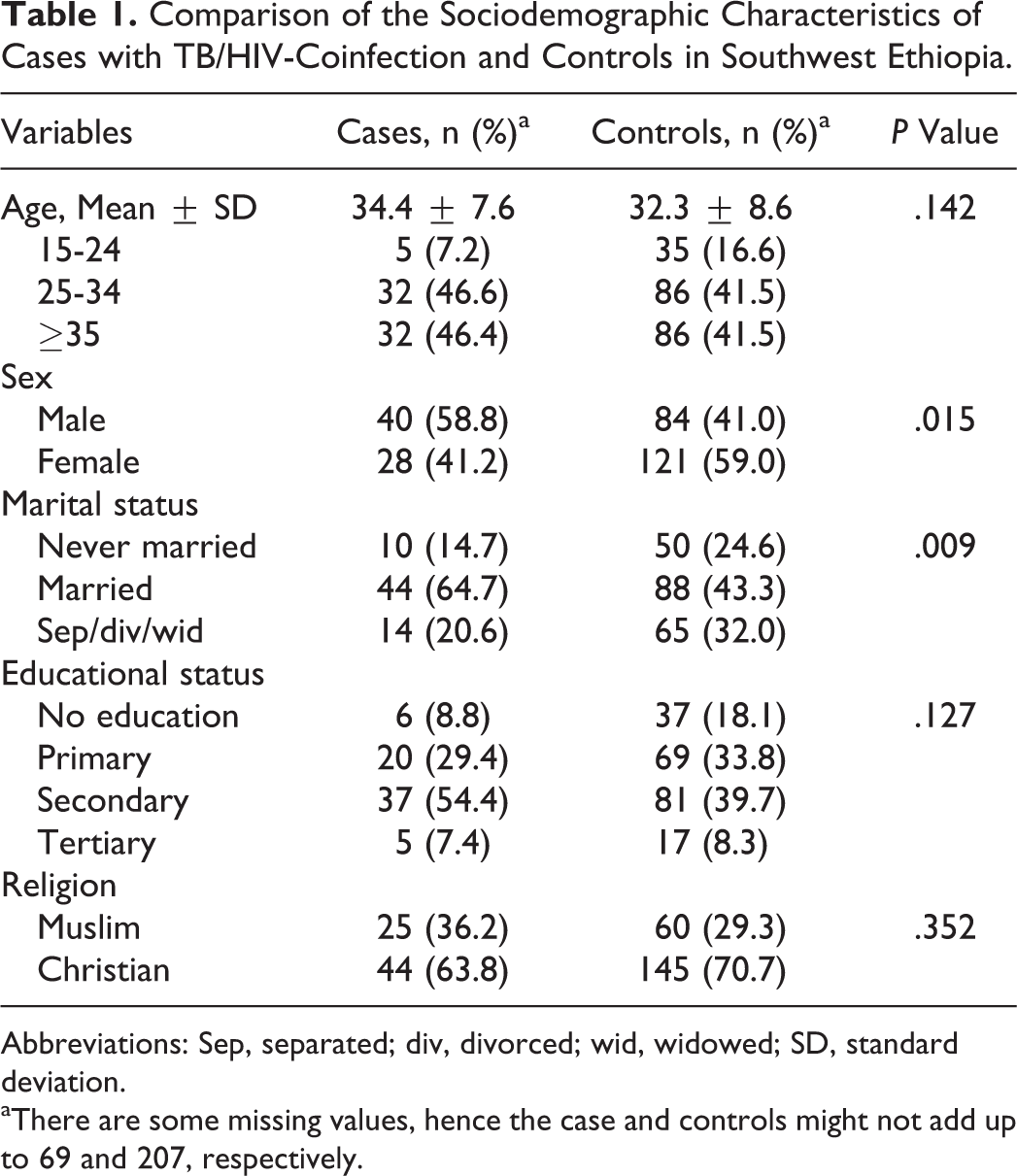
Abbreviations: Sep, separated; div, divorced; wid, widowed; SD, standard deviation.
aThere are some missing values, hence the case and controls might not add up to 69 and 207, respectively.
At ART initiation, there was no difference in mean CD4 count between cases and controls but cases were more bedridden (P = .002), had cough for more than 2 weeks (P < .001), reported more night sweating (P = .005), and were in later disease stage (World Health Organization [WHO] stage III and IV) than controls (P = .013; Table 2).
Comparison of Clinical Characteristics of Cases with TB/HIV Coinfection and Controls in Southwest Ethiopia.

Abbreviations: TB, tuberculosis; WHO, World Health Organization.
aThere are some missing values, hence the cases and controls might not add up to 69 and 207 respectively.
In the final logistic regression model, we kept baseline CD4 in the final model as it consistently predicted mortality, although it was not significantly associated in our study. Male sex (OR = 2.04; 95% CI: 1.04-4.02), being bedridden (OR = 2.84; 95% CI: 1.17-6.89) or in ambulatory status but unable to do daily routine activities (OR = 3.01; 95% CI: 1.30-6.98), and presence of cough of 2 weeks at ART initiation (OR = 4.75; 95% CI: 2.14-10.56) were found to be the independent predictors of morality among TB/HIV-coinfected patients (Table 3).
Predictors of Mortality Among TB/HIV-Coinfected Patients in Southwest Ethiopia.

Abbreviations: COR, crude odds ratio; CI, confidence interval; AOR, adjusted odds ratio; TB, tuberculosis; Sep, separated; div, divorced; wid, widowed; WHO, World Health Organization.
aThere are some missing values, hence the cases and controls might not add up to 69 and 207, respectively.
Discussion
Of the 188 deaths in the cohort, 36.7% were TB/HIV-coinfected individuals, highlighting the continued mortality risk among persons with HIV infection due to TB. This study identified the risk factors for mortality among TB/HIV-coinfected patients in a hospital setup. Male sex, weak functional status of patient at enrollment, and presence of cough were independent risk factors for mortality. The time of death was not investigated in our study. However, previous studies from Uganda documented that 68% of deaths occurred within the first 6 months of TB diagnosis. 8
In the current study, most of the deaths among TB/HIV-coinfected patients occurred in the first 6 months of ART. This is also consistent with previous studies. 3,8,17,18 Most of the patients who died had pulmonary TB and cough for more than 2 weeks during enrollment. More than 95% of the cases came to the health institution with WHO stage III or IV, indicating that patients seek health care at the end stage of TB/HIV disease. However, one cannot rule out inconsistent screening of patients, which might lead to missed opportunity for early initiation of treatments. This indicates the importance of strengthening efforts of screening for TB using adapted and validated tools.
Similar to previous studies, 2,8,19 male sex was a predictor of mortality among TB/HIV-coinfected patients. Earlier health- seeking behavior of women 20 might explain the discrepancies of death among men and women. Furthermore, some studies have found that women are more likely than men to be asymptomatic when accessing treatment for the first time. 20
Finally, functional status of patients was found to be a predictor of mortality. As a result of stigma and delay in diagnosis, patients could stay long without treatment and hence have poor functional status and prognosis. Thus, priority must be given to identify TB/HIV-coinfected individuals and start treatment earlier.
Our study has several weaknesses. First, mortality might be underestimated since patients lost to follow-up probably included individuals dying at home without being reported. Second, due to many missing values, we were not able to include possible predictors of death such as hemoglobin (anemia) and malnutrition. 21-25 In addition, the exact time of death was not registered therefore we could not perform a survival analysis to identify predictors, taking into consideration the time factor. Finally, the time of ART initiation from the diagnosis of HIV infection was not known, which might be a possible predictor.
In summary, mortality among TB/HIV-coinfected patients accounted for a considerable number of deaths among the cohort. Most of these deaths were among patients diagnosed with TB before ART initiation or at start of ART. Almost all deaths among TB/HIV-coinfected cases occurred in the first 6 months of ART initiation, thus implying the importance of intensified follow-up of patients during this period. Patients with cough at ART initiation and with poor functional status should be strictly followed to reduce death.
Footnotes
Acknowledgments
We would like to thank all staff members of the Jimma University Hospital ART clinic and the medical team of Jimma University Hospital for taking care of the patients.
Authors’ Note
KD and AY conducted the study, participated in the analysis of the data, and wrote the article. All authors contributed to the design of the study, assisted with data interpretation, participated in the preparation of the manuscript, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received support from Jimma University and University of Copenhagen Alliance for Nutrition (JUCAN) for the research. The funders had no role in the preparation and decision to publish this article.