
Abstract
Setting:
A private multispecialty hospital in Kakinada, Andhra Pradesh, India.
Methods:
A survey of knowledge, attitudes, and perceptions adapted from a pretested questionnaire was administered to 128 HIV-infected adults, from July to August 2008.
Results:
A total of 31% had not heard of tuberculosis (TB), with 15 (38%) currently receiving anti-TB therapy or had received it in the past. Of those familiar with TB, 70% could not list a method by which it was spread. Low education attainment, female sex, and less frequent television exposure were associated with low TB literacy.
Conclusions:
HIV-infected patients in southeast India have poor knowledge of TB and the methods by which it is spread. Scale-up of patient-directed educational programs is necessary to help control TB in India.
Background
India has an estimated 2.4 million people infected with HIV/AIDS, 1 with the 4 high-prevalence southern states of Andhra Pradesh, Maharashtra, Karnataka, and Tamil Nadu, accounting for 55% of all infections in the country. 2 The state of Andhra Pradesh has India’s largest absolute burden of disease, with 500 000 adults infected (0.90% prevalence), 2 and the East Godavari District has the state’s highest prevalence of HIV/AIDS (1.25%). 3 Furthermore, India has the world’s largest burden of tuberculosis (TB) and accounts for 26% of the global burden of disease. 4 An estimated 40% of India’s population is infected with the TB bacillus (latent infection), 5 with 3.1 million individuals estimated to have active TB disease. 4 Nationally, 9% of TB patients tested are coinfected with HIV, 4 and government data suggest the impact of HIV/TB c-infection is especially severe in the state of Andhra Pradesh and East Godavari district, with 13% and 22% of confirmed TB cases also HIV positive in the state and district, respectively. 5 Given that people living with TB/HIV coinfection are 21 to 34 times more likely to develop active TB disease than those who are HIV negative, 4 the HIV and TB epidemics are especially relevant in India, given the country’s enormous burden of both diseases.
Many of these individuals with HIV and TB access care in India’s vast, largely unregulated private sector. While studies elsewhere in Asia and Africa have documented inadequate TB knowledge, which in turn may contribute to low treatment success rate, 6 limited research has been conducted among private clinic attendees in southeast India despite the alarming HIV and TB epidemics. The studies that have been performed have found that low TB knowledge increases the delay by the patient seeking health care and contributes to TB transmission. 7,8 Therefore, our objective was to investigate TB knowledge, attitudes, and perceptions (KAP) among HIV-infected patients attending a high-volume private clinic in a high HIV prevalence region of India.
Methods
Setting
Between July and August 2008, a cross-sectional KAP survey was performed to investigate TB transmission and care among HIV-infected adult patients attending the private multispecialty Sai Sudha Hospital (SSH) in Kakinada, Andhra Pradesh, India. Sai Sudha Hospital, a high-volume 100-bed hospital, has an estimated 1300 HIV patient-visits/month.
Study Design
Given the high patient volume as well as clinical and clerical burden on counseling staff administering the survey, a convenience sample of patients was surveyed for 5 weeks between July and August 2008, with a target sample size of 120 patients. The HIV clinic was open 6 days/week (Monday through Saturday, 9
The enrollment approach taken by the trained study counselor was as follows: all patients visited the counseling room to obtain their chart and note any questions, concerns, or changes in symptomology prior to their visit with the on-site physician. During this initial counseling room visit, the counselor performed a chart review to identify and confirm inclusion criteria (HIV-positive status, adult age 18-65 years). Patients meeting inclusion criteria were approached and offered the opportunity to participate in the orally administered questionnaire while waiting to be seen by the physician. Consent was obtained from all study participants and of those approached, fewer than 5 people refused to participate.
The study was submitted to the Johns Hopkins University Institutional Review Board (JHU IRB) and SSH Institutional Review Board (IRB) and was deemed exempt from the review as no personal identifiers were taken and no clinical evaluation was performed as part of the study.
Inclusion/Exclusion Criteria and Informed Consent
Confirmed HIV-positive adult patients between 18 and 65 years attending SSH were given an opportunity to anonymously complete the HIV/TB KAP survey with a trained on-site study counselor in the local language of Telugu. A detailed informed consent form approved by the JHU IRB and SSH IRB outlining study purpose, objectives, and methods as well as risks, benefits, and practices to maintain confidentiality was translated into the local language of Telugu and provided and read orally to all study participants. It was explained that no compensation would be awarded and survey completion or lack thereof would not affect on-site care. Patients were excluded if they did not meet adult age (>18 years) criteria, if they were HIV negative, or if they did not consent to participate.
Data Collection
A 95-question survey, which took roughly 30 minutes for a counselor to complete, and respondent profile (completed by the on-site clinician, investigator, or counselor) were primarily adapted from 2 surveys, respectively, (1) a pretested survey utilized on-site in 2005 9 and (2) a validated questionnaire utilized in 2007. 10 Tuberculosis-specific questions were adapted from a survey administered by the Indian government. 11 Questions included TB and HIV KAP, TB contact tracing, health care–seeking behavior, treatment satisfaction, and demographics. Tuberculosis awareness was defined as a yes/no response to the question, “have you ever heard of TB”? Clinical examination and CD4 counts were abstracted from patient medical records to create a respondent profile. Materials were prepared in English and translated to Telugu by local physicians and counselors using local phrases and language. Back translation was performed to ensure accuracy. The study was piloted on 5 patients and minor changes were made to refine local terminology.
Analysis
General characteristics of participants who had heard of TB versus those who had not were compared using χ 2 tests. Univariate odds ratios for TB awareness were obtained using simple logistic regression. Based on the results of the univariate analysis, multiple logistic regression analysis was used to identify factors independently associated with TB awareness. Variables that were significant at P < .1 or had previously been associated with TB awareness were assessed in the multivariate model. Analysis was performed using STATA version 9 (Cary, North Carolina).
Results
Demographics
Participant data are presented in Table 1. Of the 128 HIV-infected patients surveyed, 72% were male, the median age was 35 years, and all were from the state of Andhra Pradesh, with 65% from the East Godavari district, 25% from West Godavari, and 10% from other districts. A total of 65 (51%) were rural residents, 36 (28%) had primary education or less, 102 (80%) were married or had a live-in partner, and 11 (9%) were widows. A total of 59 (59%) had a monthly income of 5000 INR (∼US$110) or less. Patients predominantly traveled by bus (63%), bicycle (15%), or train (12%), with 26%, 27%, and 8% traveling 50 to 99 km, 100 to 200 km, and over 200 km, respectively, to reach the hospital. The median CD4 count was 216 cells/mm3 (interquartile range [IQR], 132-385 cells/mm3).
Tuberculosis Awareness by Patient Characteristics.

Abbreviations: ATT, anti-TB therapy; TB, tuberculosis.
aUnskilled labor: agricultural, migrant, housewife, etc; semiskilled: truck driver, community sex worker, shopkeeper, etc; skilled: professional, government employee, small business, etc.
HIV and TB KAP
The HIV and TB KAP data are presented in Table 2. HIV and TB knowledge and awareness were limited. When asked what the most common diseases were in their neighborhood, 88 (69%) did not know, and of those who did respond, 68% did not mention HIV or TB. In all, 40 (31%) had not heard of TB, of whom 15 (38%) had received anti-TB therapy (ATT) in the past or were currently receiving ATT. Among the 88 patients who had heard of TB, 47 (53%) were not familiar with ATT and 62 (70%) could not list a correct method of TB transmission. However, 51 (59%) felt patients with TB should wear a mask and 92 (82%) believed it to be advantageous or permissible for hospital staff to wear masks. A total of 20 (24%) familiar with TB did not know or did not think a person with TB could become cured and 45 (54%) did not know or did not think TB medications could prevent further sickness.
HIV and Tuberculosis Knowledge, Attitudes, and Perceptions among 128 HIV-Infected Patients Attending the Sai Sudha Hospital.
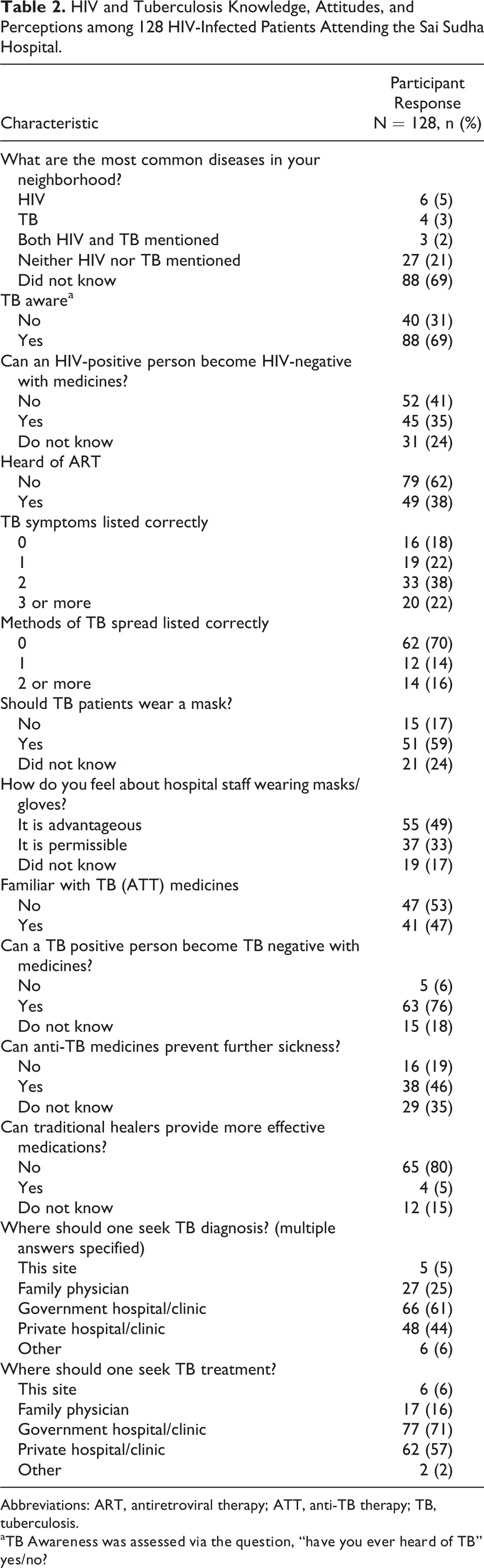
Abbreviations: ART, antiretroviral therapy; ATT, anti-TB therapy; TB, tuberculosis.
aTB Awareness was assessed via the question, “have you ever heard of TB” yes/no?
HIV knowledge was limited as well, as 79 (62%) had not heard of antiretroviral therapy (ART) and 45 (35%) thought a person can become HIV negative (cured) with medications. An additional 31 (24%) did not know whether medications could cure HIV.
A univariate analysis was performed to examine TB awareness based on age, sex, education levels, and other demographic groups within our study. Based on their statistical significance, these 3 variables as well as 2 others, prior ATT and television (TV) watching frequency, were examined in a multiple logistic regression. In this analysis, decreased likelihood for TB awareness was associated with female sex (adjusted odds ratio [AOR] 0.33, 95% CI 0.12-0.94) and irregular TV watching (AOR 0.29, 95% CI 0.11-0.77) compared with those who watch TV regularly. Increased likelihood for TB awareness was also associated with increasing educational levels (AOR 3.61, 95% CI 1.37-9.52 and 8.53, 95% CI 2.27-32.00 for 4th-10th standards and greater than 10th standard, respectively, compared with 4th standard and below).
Discussion
In our study of 128 HIV-infected patients attending a private clinic in southeast India, low knowledge levels and awareness of HIV, ART, TB, and ATT were observed. The majority of patients could not list common diseases in their neighborhoods, and if they had heard of TB, many did not know the disease is curable and had difficulty naming symptoms and modes of transmission. Furthermore, ATT awareness and knowledge was limited, even among some of the patients who were receiving ATT or had received it in the past. This may be explained by the social stigma associated with HIV/AIDS and TB in India, which in some cases results in scenarios in which a family member manages a patient’s medical care and protects the patient from knowing his or her condition or the reason for taking medicine. 12,13
This lack of health education is concerning, as systematic reviews have suggested that low TB knowledge levels contribute to the spread of the disease and increase the delay by the patient seeking health care, in India and elsewhere. 14,15 These barriers to accessing care result in increased TB transmission to family members and community as well as poor patient outcomes. The case of increased TB literacy is warranted if we are to improve treatment adherence and reduce the burden of TB in persons with HIV. Health education for at risk patients in the form of awareness and advisory materials/protocols, education by social workers, broadcasting HIV/TB issues in media, and increased patient counseling by physicians/staff are all strategies worthy of further implementation. 16,17
Limitations
While our study did utilize previously validated questionnaires and questions from national surveys, the authors acknowledge that the terminology used in the survey may not have captured all of the local understanding, despite translation by local physicians and counselors in addition to back translation. Other limitations of the study include the convenience sampling method, however, the study team approached patients during a 5- to 6-hour time frame daily, and our findings corroborate published reports on low TB literacy in India. 18 As such the study may have been limited by sampling bias and social desirability bias, in that patients visiting the study site may have participated wanting to disclose information. Since the study looked at patients attending a high-volume private clinic in Kakinada, it may be difficult to extrapolate or generalize to other types of smaller private sector clinics and clinics that see few HIV patients.
Recommendations
Results of this study indicate that TB literacy campaigns targeting specific populations, including women, those with low educational levels, and those who have limited access to TV, are warranted. Women in particular may require targeted educational interventions, as other studies within India and elsewhere in Asia have found women to be less knowledgeable of specific TB symptoms than men. 19,20 Other studies have also found TV to be a significant source of TB-specific information, more commonly in men than in women. 21 A specific strategy worthy of further exploration and implementation in the Indian context and elsewhere is the use of cell phone communication and audio/text messaging to improve health education and medical adherence. India has the world’s greatest cell phone growth, with over 1.1 billion users projected by 2013, 22 and efforts utilizing cell phones to promote adherence to ART and lifelong learning among illiterate and semi-literate rural women in South India have demonstrated success. 23,24 While our study did not investigate this parameter directly, it was observed that counselors at the study site utilized cell phones and audio/text messaging to communicate directly with patients or caretakers regarding appointments, treatment regimen, or medical inquiries with apparent success.
Furthermore, since insufficient health systems and health care infrastructure have contributed to the inability to effectively control TB in the region, opportunities such as public–private partnerships should continue to be further implemented and emphasized. 25 Patient commitment to travel significant distances indicates the importance of private sites for prevention, diagnostic, and treatment efforts. Pooling resources and engaging private sector clinics may be of benefit to provide enhanced patient care and control of TB, as such sites may offer unique and well-equipped diagnostic technologies, educational programming opportunities, and physicians and support staff.
Ultimately, these findings demonstrate the necessity of implementing effective health education programs that emphasize the modes of TB and HIV transmission, treatment options, and curability, as the social and economic burden of HIV/AIDS and TB in southeast India is significant.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The primary author received travel funding from the Johns Hopkins University Homewood Department of Public Health Studies while he was affiliated with the institution as an undergraduate student. The authors received no financial support for the authorship and/or publication of this article.