
Abstract
Objective
This study aimed to detect circulating microRNA (miR)-17 and miR-20a levels in patients with pulmonary arterial hypertension (PAH), and to investigate whether circulating miR-17 levels are associated with PAH.
Methods
Thirty-five PAH patients and 20 healthy controls were enrolled in the study. Circulating miR-17 and miR-20a levels were measured using real-time PCR analysis.
Results
miR-17 levels were significantly increased in PAH patients compared with healthy controls. They were also higher in PAH patients at World Health Organization functional class (WHO FC) III–IV than WHO FC I–II PAH patients. There was no significant difference in miR-20a levels between PAH patients and controls. miR-17 had a high area under the corresponding receiver operating characteristic curve. Further, we found that circulating miR-17 levels correlated with the 6-minute walk distance, mean pulmonary artery pressure, and mean right atrial pressure in PAH patients.
Conclusion
Circulating miR-17 levels may be associated with human PAH. Therefore, miR-17 could be used as a diagnostic index and prognostic factor for PAH patients.
Keywords
Introduction
Pulmonary hypertension (PH) is a pathophysiologic hemodynamic condition, historically defined as a resting mean pulmonary artery pressure (mPAP) ≥25 mmHg. 1 The 6th World Symposium on Pulmonary Hypertension proposed modifying the definition of PH as mPAP >20 mmHg. 2 Recent classifications identify five groups of PH: pulmonary arterial hypertension (PAH), PH due to left heart disease, PH due to lung diseases and/or hypoxia, PH due to pulmonary artery obstruction, and PH with unclear and/or multifactorial mechanisms. 3 Several advances have been made in the field of PH during the past decade; however, it remains a fatal disease, suggesting an urgent need for a better understanding of the pathogenesis of PH.
MicroRNAs (miRNAs) are small, non-coding endogenous RNA molecules that regulate target genes at the posttranscriptional level. Several studies have suggested that the expression profile of miRNAs in PAH patients is altered compared with healthy controls.4,5 Moreover, some miRNAs have been confirmed to function in the development of PAH in a variety of experimental models.6–11
The miR-17-92 cluster contains six mature miRNAs, including miR-17, miR-18a, miR-19a, miR-19b, miR-20a, and miR-92a. 12 This cluster was initially linked to tumorigenesis,13,14 but recent loss-of-function studies revealed that it is required for lung development. For example, miR-17-92 knockout caused severely hypoplastic lungs in mouse embryos, leading to death shortly after birth. 15 Emerging evidence has also suggested that the miR-17-92 cluster is linked to vascular pathogenesis, including coronary artery disease and PAH.16,17 The cluster was found to induce the proliferation of lung epithelial cells and pulmonary artery smooth muscle cells, making them resistant to apoptosis and resulting in PAH. Moreover, the smooth muscle cell-specific knockout of miR-17-92 attenuated hypoxia-induced PAH in mice. 18
miR-17 and miR-20a are two miR-17-92 cluster members in experimental PAH. Bone morphogenetic protein receptor type-2 (BMPR2) plays an important role in endothelial and vascular smooth muscle cells, as well as in the vascular remodeling of the pulmonary arterial circulation.19,20 Both miR-17 and miR-20a can target BMPR2 and inhibit its function. 21 Additionally, the functions of miR-17 and miR-20a in regulating the homeostasis of cardiopulmonary systems have been demonstrated in experimental PAH. However, clinical studies into the roles of miR-17 and miR-20a in PAH are lacking.
In the present study, we detected circulating miR-17 and miR-20a levels in patients with PAH, and investigated whether circulating miR-17 levels are associated with PAH.
Materials and methods
Study subjects
This study included 35 PAH patients and 20 healthy controls. All subjects gave their informed written consent for study participation, and the study was approved by the Ethics Committee of the Second Hospital of Shanxi Medical University. Patients diagnosed with precapillary PAH by right heart catheterization at the Second Hospital of Shanxi Medical University from April 2015 to December 2017 were recruited. The diagnosis of PAH used previous hemodynamic definitions (mPAP ≥25 mmHg). Among the 35 PAH patients, 12 had idiopathic PAH, 18 had PAH associated with congenital heart disease, and five had PAH associated with connective tissue disease. Exclusion criteria included infections, ischemic heart disease, hypertension, diabetes, malignant tumors, and liver disease.
Healthy controls were recruited during physical check-ups. Body mass index (BMI) was calculated as body weight (in kilograms) divided by the height (in square meters). The 6-minute walk test (6MWT) was performed according to American Thoracic Society guidelines. 22 Hemodynamic data were assessed by right heart catheterization. Cardiac output (CO) and cardiac index (CI) were obtained using the Fick method 23 as the average of three cardiac cycles with <10% variation. Pulmonary vascular resistance (PVR) was calculated by the formula: PVR = (mPAP – pulmonary capillary wedge pressure (PCWP))/CO. The assessment of functional classification of PAH was performed according to World Health Organization (WHO) guidelines. 24
Collection of blood samples and real-time PCR
Ethylenediaminetetraacetic acid whole blood samples were collected through peripheral vein puncture. Total RNA was extracted from whole blood using the miRNeasy Mini Kit (Qiagen Inc., Valencia, CA, USA) following the manufacturer’s instructions. cDNA was reverse-transcribed using the TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems, Foster City, CA, USA). Real-time PCR was performed on an ABI 7300 Real-Time PCR system using the TaqMan miRNA Assay kit (Applied Biosystems) for 40 cycles of 95°C for 30 s, 58°C for 30 s, and 72°C for 30 s. The following primers were used: miR-17: forward, 5′-GCCGCCAAAGTGCTTACA-3′, reverse, 5-′AGAGCAGGGTCCGAGGT-3′; and U6: forward, 5-′CTCGCTTCGGCAGCACA-3′, reverse, 5′-AACGCTTCACGAATTTGCGT-3′. Primers and probes were used at a final concentration of 250 nM and 125 nM, respectively.
Statistical analysis
All statistical analyses were performed using GraphPad Prism Software (GraphPad Software, San Diego, CA, USA). Differences between two groups were compared with the Student’s t test, and differences among three groups were compared using one-way analysis of variance. The chi-square test was used to analyze count data. Receiver-operating characteristic (ROC) curve analysis was applied to evaluate diagnostic values. Pearson’s correlation test and linear regression analysis were used for correlation assessment. P values less than 0.05 were considered significant.
Results
miR-17 expression is increased in the blood of patients with PAH
Clinical characteristics of 35 PAH and 20 healthy controls are shown in Table 1. There were no significant differences in age, gender, or BMI between PAH patients and controls. PAH patients showed a significantly decreased 6-minute walk distance (6MWD) compared with controls (P < 0.01). Hemodynamic parameters, including mPAP, PCWP, PVR, and mixed venous oxygen saturation (SvO2), differed significantly between PAH patients and controls (P < 0.01).
Characteristics of PAH patients and healthy controls.

PAH, pulmonary arterial hypertension; BMI, body mass index; 6MWD, 6-minute walk distance; mPAP, mean pulmonary artery pressure; mRAP, mean right atrial pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; CI, cardiac index; SvO2, mixed venous oxygen saturation.
We next investigated miR-17 expression patterns, and observed significantly increased levels in PAH patients compared with controls (P < 0.01; Figure 1a). Subsequently, we tested whether circulating miR-17 levels differed among PAH patients grouped by WHO functional class (WHOFC). Significantly increased miR-17 levels were detected in WHO FC I–II (P < 0.05) and WHO FC III–IV (P < 0.01) patients compared with controls. Furthermore, miR-17 expression levels were significantly higher in WHO FC III–IV than WHO FC I–II patients (P < 0.05; Figure 1b).
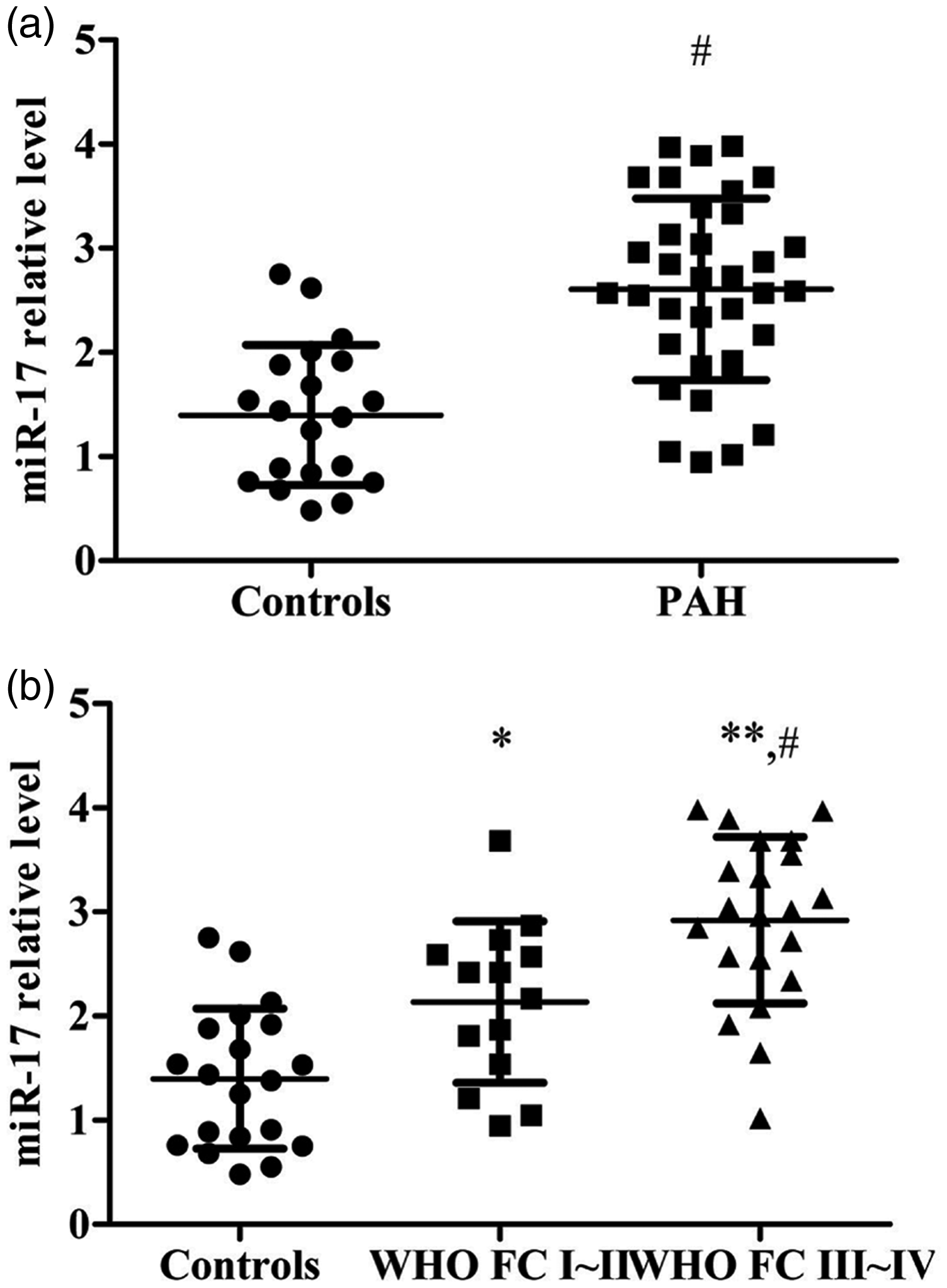
Circulating miR-17 expression is increased in patients with PAH. (a) Circulating miR-17 levels in PAH patients and healthy controls. (b) Circulating miR-17 levels in PAH patients grouped by WHO FC. PAH, pulmonary arterial hypertension; WHO FC, World Health Organization functional class. *P < 0.05 and #P < 0.01 vs. Control; **P < 0.05 vs. WHO FC I–II.
Diagnostic value of miR-17 in PAH
Using ROC analysis, we observed that circulating miR-17 expression levels could be used to distinguish between PAH patients and healthy controls. The area under the curve for single-factor diagnosis of PAH was 0.8571, which had diagnostic significance (P < 0.001; Figure 2).

ROC for the diagnostic value of miR-17 in PAH. PAH, pulmonary arterial hypertension; ROC, receiver operating characteristic.
miR-17 expression levels correlated with 6MWD, mPAP, and mRAP in PAH patients
As shown in Figure 3, a significant inverse correlation was observed between miR-17 expression levels and the 6MWD (P = 0.02). Additionally, we found that levels of miR-17 were positively correlated with mPAP (P = 0.003) and mRAP (P = 0.014) in PAH patients (Figure 4a and 4b). No significant correlations were found between circulating miR-17 levels and PCWP, PVR, CI, or SvO2 (Figure 4c–f).

Correlation between miR-17 levels and 6MWD in PAH patients. PAH, pulmonary arterial hypertension; 6MWD, 6-minute walk distance.

Correlation between miR-17 levels and hemodynamic parameters in PAH patients. PAH, pulmonary arterial hypertension; mPAP, mean pulmonary artery pressure; mRAP, mean right atrial pressure; PCWP, pulmonary capillary wedge pressure; PVR, pulmonary vascular resistance; CI, cardiac index; SvO2, mixed venous oxygen saturation.
miR-20a expression was not altered in the blood of patients with PAH
Finally, we investigated the expression pattern of miR-20a in PAH patients and healthy controls. As shown in Figure 5, no significant difference was detected between the two groups.

Circulating miR-20a levels in PAH patients and healthy controls. PAH, pulmonary arterial hypertension.
Discussion
Several circulating biomarkers have previously been shown to be associated with PAH, including markers of neurohormonal activation, inflammation, oxidative stress, vascular damage, and remodeling. However, none of these shows all the characteristics of an ideal biomarker such as non-invasion, ease of measurement, low cost, and high sensitivity and specificity. 21 Therefore, a multiparameter approach is desirable to not rely on a single biomarker. 21
This report showed that circulating miR-17 levels are increased in patients with PAH compared with healthy controls. We also observed increased miR-17 in PAH patients with a higher WHO FC. Because WHO FC is associated with outcomes in PAH, this suggests that miR-17 has the potential to indicate disease severity.
miR-17 was previously reported to be upregulated in various cancers and to control cell proliferation and migration.7,25–27 It also plays important roles in regulating homeostasis of the cardiopulmonary system, while miR-17 overexpression was found to increase lung epithelial proliferation. 28 Additionally, miR-17 is involved in the induction of PAH. Hypoxia upregulates the transcription of miR-17, and miR-17 was reported to contribute to hypoxia-induced pulmonary artery smooth muscle cell proliferation and migration. 29 A study by Pullamsetti et al. 30 demonstrated that miR-17 inhibition improves heart and lung function in experimental PAH by interfering with lung vascular and right ventricular remodeling. miR-17 overexpression represses BMPR2, and the downregulation of BMPR2 leads to remodeling of the pulmonary vascular bed associated with PAH. Because advanced pulmonary hypertensive vascular disease is characterized by the development of pulmonary vascular remodeling, increased circulating miR-17 levels in PAH may reflect vascular remodeling. However, although miR-20a was shown to affect endothelial cell proliferation and angiogenesis, 31 and to be involved in the development of PAH in vitro, 20 we found no significant difference in circulating miR-20a levels between healthy controls and PAH patients.
In the present study, ROC curve analysis was used to evaluate the diagnostic value of miR-17 levels in PAH. miR-17 showed a high area under the corresponding ROC curve, suggesting that it could be used as a diagnostic index for PH patients.
The 6MWT is commonly used in PAH patients for the objective assessment of exercise capacity, 24 providing information about functional status, disease prognosis, and the efficacy of therapy in clinical trials.32,33 In the present study, a significant negative linear relationship was observed between 6MWD and circulating miR-17 levels in PAH patients. PVR is important for the clinical classification of PH, while PCWP is required for the differential diagnosis of PH due to left heart disease, with PCWP >15 mmHg excluding a diagnosis of precapillary PAH. Moreover, SvO2 is of prognostic importance in PH, and mPAP, mRAP, and CI were closely associated with survival in patients with primary PH.24,34 PAH patients with poor survival were previously shown to have elevated mRAP and mPAP, and decreased CI. 24 In this study, analysis of hemodynamic parameters in PAH patients revealed an association between increased circulating miR-17 levels and higher mPAP and mRAP. These results indicate that miR-17 could be used to predict disease progression and prognosis.
A limitation of this study is that we did not perform a sample size calculation, and that the limited number of samples may affect the statistical significance of the results. Further limitations include that we did not perform multivariate analyses, and we only provided data from a single time point. Additional studies are therefore needed to address the temporal course of miR-17 expression, and its correlation with hemodynamic parameters and classic biochemical indicators of PAH.
In conclusion, this study provides clinical evidence that circulating miR-17 levels may be associated with human PAH, and suggests its potential application as a new biomarker in clinical PAH.