
Abstract
Background:
Renal insufficiency has been shown to be a significant, independent risk factor for mortality among HIV-infected patients. Unfortunately, little is known about the prevalence and nature of renal impairment in African populations initiating antiretroviral treatment. This study aims to find the prevalence of abnormal renal function among antiretroviral therapy (ART)-naive, HIV-infected patients in the South Eastern geopolitical zone of Nigeria.
Method:
This is a cross-sectional hospital-based study, involving 300 ART-naive HIV-positive patients, seen over a 1-year period, aged from 18 years and older, presenting to the clinic for the first time.
Results:
A total of 300 patients were included in the study, 104 (34.7%) males and 196 (65.3%) females. The prevalence of significant renal disease was 24.3% (73 of 300), while 38.3% (115 of 300) had mild renal impairment. Using logistic regression, age, CD4 count, urea, creatinine, and hemoglobin were significantly associated with renal impairment.
Conclusion:
The authors observed a high prevalence of significant renal impairment among HIV-infected patients at the time of ART initiation.
Keywords
Introduction
Long-term infection with HIV is associated with numerous renal complications. It can cause HIV-associated nephropathy (HIVAN) or other disease states as a result of opportunistic infections, intercurrent illnesses, or other side effects related to treatment of HIV infection. 1 –6
Studies from several sub-Saharan Africa have reported a variable prevalence of these diseases in HIV-infected patients: 6% in South Africa, 38% in Nigeria, 26% in Côte d'Ivoire, 28% in Tanzania, 25% in Kenya, 20%-48.5% in Uganda, and 33.5% in Zambia. 7 Results from these studies also suggest that a broader spectrum of histopathological lesions in HIV-associated kidney disease exists in the African populations than was previously thought. 7 Regardless of the underlying cause, however, renal insufficiency has been shown to be a significant, independent risk factor for mortality among HIV-infected patients. 8
Despite the high burden of both HIV and renal disease in sub-Saharan Africa 9,10 and the rapid progression to end-stage renal disease (ESRD) in the absence of highly active antiretroviral therapy (HAART), few studies to date have tried to determine the true prevalence of abnormal renal function among antiretroviral therapy (ART)-naive patients. 11 This study therefore aims to determine the prevalence of abnormal renal function among ART-naive, HIV-infected patients in the South Eastern geopolitical zone of Nigeria.
Methods
Ethical approval was obtained from the research and ethical committee of the University of Nigeria Teaching Hospital (UNTH), Ituku Ozalla, Enugu.
In this cross-sectional study, patients with confirmed HIV infection, with no previously documented risk factors for renal insufficiency, were consecutively recruited and studied over a 1-year period. Study participants included patients presenting for the first time at the HIV clinic of the UNTH Ituku Ozalla, a referral center that receives patients from south eastern and south—south states of Nigeria. All patients were ART naive and aged 18 years and older.
Patients with conditions known to be associated with kidney abnormalities, sickle cell disease, acute infection, pregnancy, previously diagnosed diabetes, systemic hypertension, or previously known renal disease were excluded.
Baseline medical information was obtained from eligible patients using a structured pretested questionnaire. Information on HIV-associated conditions was also obtained. Blood pressure, weight, and height were documented, and CD4 count (Roche Monitor 1.5 test kit; Becton-Dickinson FACS Count), hemoglobin, blood urea nitrogen, creatinine (fixed time kinetic assay by Human) were obtained. Serum electrolytes and viral load were also carried out at this first contact.
Creatinine clearance was calculated using the Cockroft and Gault (CG) formula, which studies have shown to be comparable to other formulae for estimating estimated glomerular filtration rate (eGFR) in HIV-infected patients.
12,13

Clinical guidelines from the US National Kidney Foundation’s Kidney Disease Outcome Quality Initiative (K/DOQI) to categorize renal insufficiency were used to grade renal impairment. 14 Creatinine clearance of >90 mL/min per 1.73 m2 was considered normal; creatinine clearance of 60 to 89 mL/min per 1.73 m2 (K/DOQI stage 2) was categorized as mild renal insufficiency; 30 to 59 mL/min per 1.73 m2 as moderate insufficiency (K/DOQI stage 3); and <30 mL/min per 1.73 m2 as severe insufficiency (K/DOQI stages 4 and 5). For the purposes of this study, GFR of below 60 mL/min per 1.73 m2 was used as the cutoff point for significant renal impairment. 15
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences version 15. Independent sample t test was used to compare the means of variables, and Pearson chi-square cross-tabulation was used to test the significance of association. Correlation statistics was also done to test the associations. Risk factors for renal impairment were determined with binary logistic regression. Significant renal impairment (defined above) was the outcome variable. Results were expressed as mean (standard deviation [SD]). P values <.05 were considered significant.
Results
Patient Characteristics
Three hundred patients with HIV infection were studied. Of this, 104 (34.7%) were male and 196 (65.3%) were female. The age distribution of the patients showed that 201 (67.7%) were <40 years. The mean height of the patients studied was 1.64 m (SD = 0.08).
Among the patients with renal impairment, chronic kidney disease stage 5 was shown to be the most prevalent stage of presentation in the study population (Figure 1). Renal disease, as manifested by significant azotaemia (GFR of <60 mL/min per 1.73m 2 ), was present in 73 (24%) patients, while 115 (39%) patients had mild renal impairment, that is, GFR < 90mL/min per 1.73 m2 but not as low as 60 mL/min per 1.73 m2. The mean weight of the patients with significant azotaemia was 53.42 kg (SD = 9.51 kg) compared to 63.42 kg (13.49 kg) for the others. The mean body mass index (BMI) of patients with significant azotaemia was 20.06 kg/m2 (5.60 kg/m2) compared to 23.5 kg/m2 (13.49 kg/m2) for the others. There was no statistical difference in the gender of patients with and without significant renal impairment (Table 1).
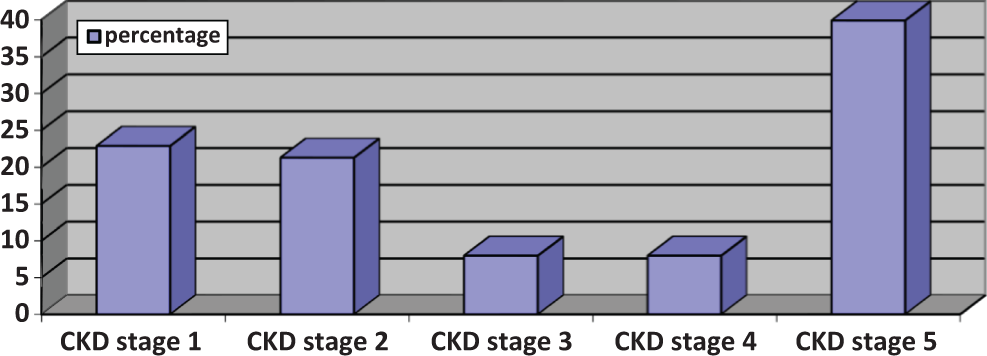
Frequency of patients who presented with renal impairment in the study population.
Characteristics of Study Population by Degree of Renal Impairment.
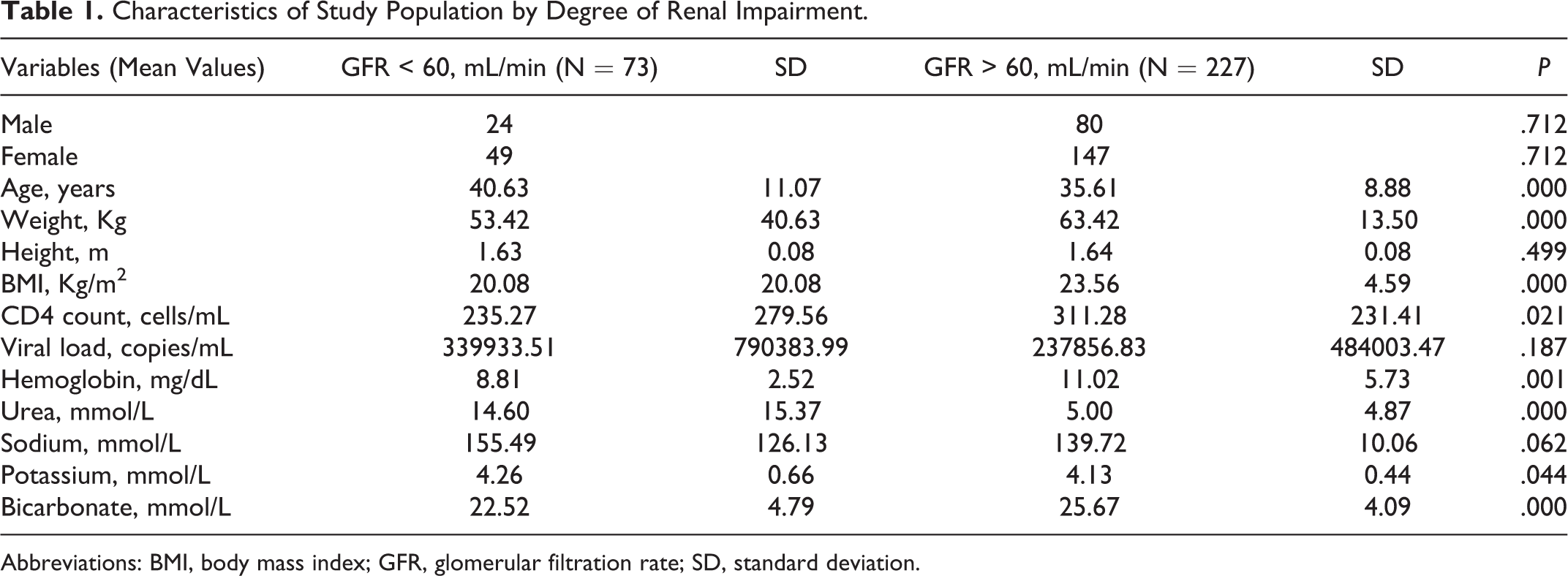
Abbreviations: BMI, body mass index; GFR, glomerular filtration rate; SD, standard deviation.
For logistic regression, significant renal impairment was used as the outcome variable. The covariates were age, gender, CD4 count, viral load, urea, creatinine, sodium, potassium, bicarbonate, and hemoglobin. Age (odds ratio [OR] 0.942, 95% confidence interval [CI] 0.915-0.970; P < .01), CD4 count (OR 1.002, 95% CI 1.000-1.003; P = .020), urea (OR 0.945, 95% CI 0.902-0.991; P = .020), creatinine (OR 0.953, 95% CI 0.939-0.967; P < .01), and hemoglobin (OR 1.416, 95% CI 1.241-1.616; P < .01) were significantly associated with the outcome (Table 1).
CD4 count was stratified to show the effect on the degree of renal impairment (Figure 2). The clinical features of all the patients used for the study was evaluated to assess any differences in presentation between HIV-infected patients, with significant renal impairment and those without significant renal impairment. The findings are as represented in Table 2.

Effect of CD4 count on the degree of renal impairment.
Frequency of Clinical Features in Patients by Severity of Renal Impairment.

Abbreviation: GFR, glomerular filtration rate.
Discussion
This study found the prevalence of significant renal impairment to be 24%, while mild renal impairment was found to be present in 39% of the patients. The high incidence of significant renal impairment found in this study correlates well with that found in a similar study in Zambia (33.5%) using the same formula. 7 However, these values are higher than what have been found in the previous studies. 11,14,16 In the study by Wools-Kaloustian et al, 11 in Western Kenya, the authors used 3 methods to estimate the GFR: CG, abbreviated modification of diet in renal disease, MDRD, and the full MDRD. 11 They recorded a prevalence of 11.5% for patients with eGFR < 60 mL/min, compared to 24% in this study. One of the reasons for this difference could be due to the smaller sample size of this study compared to the other studies referred to. It could also be because of the different methods used to estimate the GFR in these studies. The study by Roe et al was an indirect study of baseline renal function. 16 The authors calculated the eGFR, using CG formula, and found a low incidence of 5.7% among HIV-infected patients studied. This study, however, centered on the development of acute renal failure among early users of HAART. Although many researchers used the MDRD method for GFR estimation, this study and the Zambian study used the CG method and obtained high prevalence of renal impairment. There might therefore be a need to revalidate and synchronize the methods the authors use to calculate eGFR in this population.
Of note in this study is the very high prevalence of mild renal impairment in the study population. Although dose adjustment of medication or additional monitoring may not be necessary in HIV patients with mild renal impairment, and they may improve on antiretroviral therapy, it is important that such patients be identified. 14,17 Mild renal insufficiency has been reported to be associated with increased mortality risk. 7 Hence the high incidence of mild renal impairment found in this study is very significant. There is an urgent need for further study of criteria for commencing ART, bearing in mind the early onset of renal impairment in some HIV-infected patients, without any overt renal symptoms similar to those found in this cohort. The current practice, in some centers, of screening, by serum creatinine measurement, all HIV-infected patients should be encouraged or improved to include calculation of GFR using the above-mentioned equation and documenting it. For resource-poor settings, screening for renal impairment could be limited to individuals who do not immediately qualify for ART. This will detect those that will commence ART due to renal impairment, as studies have shown that in settings where renal insufficiency is diagnosed but the etiology is unknown, provision of ART in itself improves renal function. 18 This is very important considering the rapid and severe clinical course associated with HIVAN, 19 which can improve, with preservation of long-term renal function, by a trial of empiric ART. 20
Increasing age was associated with a higher incidence of significant renal impairment. This association with increasing age is similar to what other studies in Africa have described. 7,14,21
Weight and BMI were also associated with a higher incidence of significant renal impairment. Patients with renal impairment were found to have significantly lower BMI. It is unlikely that low BMI predisposed to the renal impairment, as high BMI (obesity) is what has been clearly described as a risk factor for renal impairment. 22 Low BMI associated with renal impairment in this study, though predictive of altered renal function in HIV-positive patients, is more likely to be a result of the reduced intake of calories (reduced appetite, vomiting) seen in such patients.
As expected, low CD4 counts were associated with significant renal impairment. 11,14,21 Unlike many other studies, this study evaluated the effect of viral load on the development of renal impairment. However, there was no statistical difference between the viral loads seen in the 2 groups of patients. This may not be strange, since renal impairment in HIV is not a factor of a patient’s viral load. Infact, renal involvement in HIV-infected patients can occur in the setting of undetectable viral load. 23
Low hemoglobin, bicarbonate, and high urea and potassium levels were all significantly associated with renal impairment. This is similar to what is obtained in any form of renal derangement, irrespective of the cause. It may therefore not represent a deviation from what is expected. However, in centers where serum electrolytes are not done routinely, the presence of low hemoglobin can be an added indication for electrolyte evaluation in such patients.
Of note in this study is the absence of statistical differences in the clinical presentation of patients with significant renal impairment (most of them are patients with stage V disease) compared with all the other patients. Only vomiting was found to be more associated with significant renal impairment. It therefore means that waiting for the classical symptoms of renal impairment to appear before carrying out renal function test in HIV-infected patients could be misleading, even in first time presenters.
In conclusion, the authors report a high prevalence of significant renal impairment among ART-naive patients in south-east Nigeria. The result buttresses the fact that screening for renal function should be instituted as part of the ART expansion programs. This is even more so now that some of the medications incorporated into HIV treatment have been found to be nephrotoxic. Algorithms for more aggressive assessment and management of renal insufficiency should also be developed, specifically for settings with limited diagnostic capabilities, and these should form part of the management guidelines for HIV-infected patients.
Limitations
The authors were not able to revalidate the eGFR using other methods, like the MDRD method or 24-hour urine collection for creatinine clearance. The authors were also unable to carry out protein or albumin estimation in urine, which would have been another form of kidney function assessment. The study was unable to distinguish between acute renal impairment and chronic renal impairment. Estimation of GFR and creatinine clearance is affected by medications, diet, protein intake, circulating cortisol levels, and muscle wasting, factors that this study did not explore.
Other limitations of this study include the absence of viral load data; as such, the authors were unable to correlate renal function with HIV viral load. Furthermore, as the authors enrolled only patients at a single institution in eastern Nigeria, it would be difficult to generalize these findings to other international treatment settings. However, the authors believe that with the delicate efforts made to carry out all the assessments with the utmost care, the findings of this study can form a basis for further studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.