
Abstract
Objective
This study was performed to examine the suitability of transplantation in kidney transplant recipients (KTRs) with a high body mass index (BMI).
Methods
In total, 370 consecutive KTRs stratified according to the World Health Organization BMI categories were retrospectively analysed. The estimated glomerular filtration rate (eGFR) was used to assess allograft function.
Results
The mean BMI was 26.2 kg/m2. Among all patients, 148 (40.0%) were pre-obese, 47 (12.7%) were class I obese, 11 (3.0%) were class II obese, and 9 (2.4%) were class III obese. A linear trend for male sex and younger age was observed from the normal BMI group through the progressively higher groups. Overweight and obese KTRs had a significantly higher incidence of pre-transplant diabetes, but there was no difference in post-transplant new-onset hyperglycaemia. Obesity was not a significant risk factor for a lower eGFR at the 1-year follow-up, but it became significant at the 2- and 3-year follow-ups. Graft loss occurred in 28 patients, and 25 patients died during follow-up. No difference in all-cause allograft loss was found among the different BMI groups during follow-up.
Conclusion
Obesity affects the eGFR in the long term. Allograft survival was lower, but not significantly.
Keywords
Abbreviations
BMI: body mass index
KTR: kidney transplant recipient
eGFR: estimated glomerular filtration rate
Introduction
No consensus has been established in terms of the waitlist cut-off for a high body mass index (BMI) in kidney transplant candidates worldwide. The latest national guidelines in the United Kingdom 1 no longer recommend considering the BMI as a standalone criteria; however, controversy still exists among various institutions that adopt different immunosuppressive regimens in accepting bariatric patients with end-stage renal disease for transplantation. Aside from an increased perioperative risk for this subcategory of patients undergoing major surgery, 2 the justification of selecting kidney transplant candidates based on the World Health Organization definition of obesity 3 lies on optimisation of those patients who will benefit more from the limited organ donor resource. Some institutions have therefore introduced bariatric surgery as an effective bridge to increase the eligibility of obese kidney transplant candidates. 4 However, there is an argument against weight loss while on the waiting list for deceased-donor kidney transplantation although obesity negatively affects post-transplant outcomes. 5 One important consideration is that the muscle mass and protein storage levels are critical outcome determinants in dialysed patients; additionally, a high BMI cannot properly distinguish between patients with sarcopenia and those with adiposity. Furthermore, patients with a high BMI are often better respondents to the stress of deleterious infections than are other frail and poorly nourished patients; this is commonly called the ‘obesity paradox’. 6
The present study was performed to report our centre’s experience and the mid-term outcomes of a cohort of kidney transplant recipients (KTRs) who underwent treatment with a steroid-sparing immunosuppressive protocol. We compared patient and graft survival between obese and non-obese recipients in a stratified manner.
Methods
This study was performed in accordance with the principles of the Declaration of Helsinki. Data were prospectively collected on consecutive single KTRs who underwent transplantation from January 2014 to March 2016. All patients underwent treatment with a steroid-sparing immunosuppressive regimen (7-day course of steroids) with alemtuzumab induction and tacrolimus monotherapy (trough level, 5–8 ng/mL) or interleukin-2 induction with tacrolimus (trough level, 8–12 ng/mL) and mycophenolate mofetil. If a patient was not already being treated with steroids and mycophenolate mofetil, these drugs were only introduced to treat rejection. The BMI, measured as weight in kilograms divided by the square of height in meters, was grouped according to the World Health Organization classification. The patients were divided into three weight classes according to their BMI: underweight and normal (n = 154, 42%), overweight (n = 146, 39%), and obese (n = 70, 19%).
As a measure of allograft function, the estimated glomerular filtration rate (eGFR) calculated with the Modification of Diet in Renal Disease equation 7 was determined at 3, 6, 12, 24, and 36 months post-transplantation. Both in-hospital and outpatient clinic records were considered. Delayed graft function was defined as a need for dialysis within 1 week of transplantation with a perfused graft. Graft survival was measured by the composite endpoint of all-cause graft failure, including failure due to death.
Continuous variables are presented as mean ± standard deviation. Analysis of variance and the t test were used to compare continuous variables between groups. Pearson’s χ2 test was performed for nominal or nonparametric variables. The Kaplan–Meier method was applied for survival analysis. The confidence interval was set to 95%, and P was considered significant at <0.05. Analysis was performed using IBM SPSS Version 20.0 (IBM Corp., Armonk, NY, USA).
Results
In total, 370 patients underwent kidney transplantation during the study period. The mean BMI of the overall cohort was 26.2 kg/m2. The study population comprised 148 (40.0%) pre-obese, 47 (12.7%) class I obese, 11 (3.0%) class II obese, and 9 (2.4%) class III obese patients. Table 1 shows the differences in baseline characteristics among the six weight classes. Although there were statistically significant differences in all variables assessed among the groups, only male sex and younger age demonstrated a linear trend from the normal group moving through the progressively heavier groups. Overweight and obese KTRs had a significantly higher incidence of pre-transplant diabetes (p = 0.021). No difference was found in post-transplant new-onset hyperglycaemia among the groups.
Patients’ demographic characteristics.

BMI is given in kg/m2.
Data are presented as n (%) or mean ± standard deviation.
BMI, body mass index.
Immunosuppression induction with interleukin-2 versus alemtuzumab did not differ according to BMI class (Table 1). Obesity was a significant risk factor for a lower eGFR at 3 and 6 months post-transplant; interestingly, however, while this was not a persistent finding at the 1-year follow-up, it became significant again at the 2- and 3-year follow-ups (Figure 1). Delayed graft function was not significantly different among the BMI classes. Additionally, no significant difference was found in the hospital length of stay between the non-obese and obese groups (Table 2).

Kidney function during follow-up.
Transplantation outcomes.
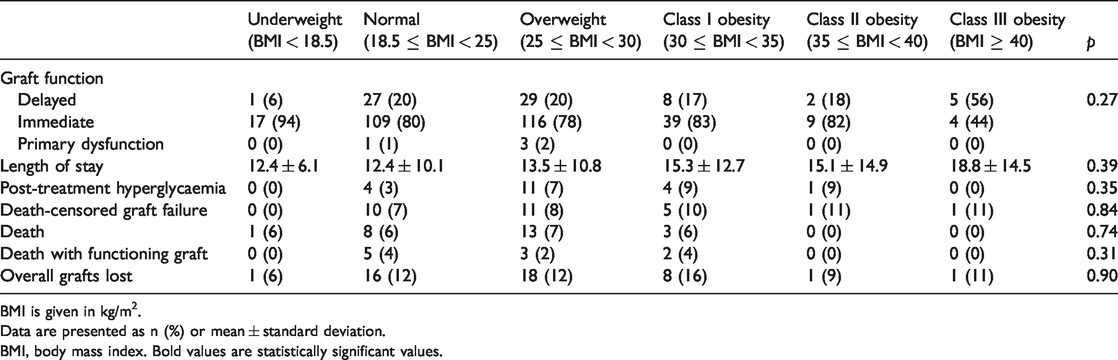
BMI is given in kg/m2.
Data are presented as n (%) or mean ± standard deviation.
BMI, body mass index. Bold values are statistically significant values.
Overall, 28 patients experienced graft loss and 25 patients died during follow-up. Forty-five allografts were lost in total; among these patients, nine died after allograft failure. To examine all-cause allograft loss, the patients were stratified into three groups: underweight and normal (n = 164, 41.3%), overweight (n = 152, 38.3%), and obese (n = 72, 18.1%). As shown in Figure 2, Kaplan–Meier analysis showed no difference in all-cause allograft loss among the different BMI groups during a mean follow-up of 42 months (range, 0–58 months). The allograft survival rate was lower in obese patients, but not significantly. Regression analysis revealed no added risk for graft loss in overweight patients (hazard ratio, 1.261; p = 0.51; 95% confidence interval, 0.63–2.53) and obese patients (hazard ratio, 1.089; p = 0.84; 95% confidence interval, 0.48–2.45) compared with recipients of normal weight when controlled by recipient ethnicity, age, sex, living versus deceased donors, and total number of mismatches.

Overall graft survival during follow-up.
Discussion
In the present study, we investigated the effect of the BMI on kidney transplant outcomes. We previously demonstrated that allograft survival was not affected by the recipient being obese or of normal weight at the 1-year follow-up 8 ; we further enhanced the prospective of transplantation rather than dialysis with the results reported herein. Allograft survival was not significantly lower at 2 and 3 years (Figure 2); therefore, obese patients benefit from kidney transplantation to the same extent as patients with a normal BMI. The eGFR was significantly lower in obese patients after the first year, as shown in Figure 1, but this should be interpreted under consideration of the general concept that an elevated BMI, waist circumference, and waist-to-height ratio are independent risk factors for a decline in the eGFR in individuals with a normal or reduced eGFR. 9 The post-transplant scenario is therefore a highly recommended time period during which to encourage weight loss and discuss the pros and cons of different strategies to achieve this. 10 If avoiding steroids is beneficial in the first year after transplant, the outcomes in the mid and long term will be influenced by the other concomitant conditions that obesity induces, namely metabolic syndrome and diabetes, hypertension, and increased risks of cardiovascular and chronic kidney disease. 11
What strategies can be implemented to preserve graft function? In KTRs, lifestyle and nutritional interventions have lower costs and reduced aggressiveness; therefore, all patients are eligible. Dietary advice should be individualised and include meal plans, exercise plans, and specific goals 12 ; this is significantly associated with weight loss in the short term, but a high dropout rate and substantial weight regain have been described. Most importantly, no cases of drug malabsorption or complications have been reported to date. This cannot be said for bariatric surgery, which is the best treatment option for severe obesity. 13 Furthermore, the long-term results significantly increase the impact of any dietary interventions, although malabsorptive procedures can impact the KTR’s immunosuppression dose, and there is uncertainty about possible effects on kidney function (e.g., enteric oxalate nephropathy). 14
Although there are surgery-related risks when choosing a weight loss strategy, we believe that bariatric procedures should be more strongly recommended in the post-transplant than pre-transplant scenario for patients with end-stage renal disease.15,16
We have shown that using a BMI cut-off is not reasonable in terms of transplant survival, and in fact our hospital does not rely on this parameter for the whole kidney transplant program. 17 However, some centres might be reluctant to adopt broader acceptance criteria. 18 Therefore, a possible way to increase transplant eligibility would be the use of robotic kidney transplantation. This technique has been proven to allow surgery in patients with extremely high BMIs with less postoperative pain and fewer wound complications, such as surgical site infections and hernia. This could be particularly advantageous in terms of overall costs and rehospitalisation, although there are initial capital costs associated with this procedure. 19
Finally, we believe that tailored immunosuppression is key. Our centre’s policy is to withdraw steroids early, within the first week after transplantation. This might contribute to ameliorating the outcome in the high-BMI population because in fact there is no difference in the incidence of post-transplant diabetes (Table 2), given that obesity is associated with an increased risk of steroid-induced diabetes. 20 In our view, a possible way forward would be the use of new drugs as belatacept, which has a better metabolic risk profile and may thus reduce drug-induced toxicities such as hypertension and diabetes. 21
Meeting presentations
Association of Surgeons of Great Britain and Ireland, 7–9 May 2019, Telford, UK 22 ; European Society Organ Transplantation Congress, 15–18 September 2019, Copenhagen, DE. 23
Footnotes
Authors’ contributions
Maria Irene Bellini designed the study, analysed the data, and wrote the paper. Kostas Koutroutsos analysed the data and wrote the paper. Hanna Nanapragasam collected the data. Emily Duerloo participated in writing the article. Jack Galliford and Paul Elliot Herbert reviewed the article and provided clinical input.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This research was supported by Imperial College London.
Informed consent
For this type of study, formal consent is not required.