
Abstract
Background:
CD4 counts vary in different populations. The present study was conducted to determine CD4 counts in different World Health Organization (WHO) clinical stages in antiretroviral therapy naïve individuals and to find out optimum CD4 cutoffs.
Method:
Data of adult HIV seropositive patients who underwent CD4 count and total lymphocyte count (TLC) testing were included for analysis. The severity of immunosuppression was graded based on WHO criteria. To establish optimum CD4 cutoff values, receiver–operator characteristics (ROC) curves were generated.
Results:
Of 754 patients, 52.2% had CD4 counts <200 cells/mm3, but only 2.3% belonged to WHO stage IV. Newer CD4 cutoffs generated were 280, 120-280, <120 cells/mm3. Spearman rank correlation between CD4 counts and TLC was found to be weak (r = .32).
Conclusion:
The cutoff values of CD4 counts for HIV disease may need to be revised for India. Regular CD4 count estimation is a must for monitoring disease progression in people living with HIV/AIDS.
Introduction
The HIVs are cytopathic viruses. The hallmark of HIV disease is profound immunodeficiency resulting primarily from a progressive quantitative and qualitative deficiency of the CD4 T cells. 1 The quantification of these has therefore been used for monitoring HIV disease progression.
In 1993, the US Center for Disease Control and Prevention, Atlanta proposed a revised classification system of HIV disease based on CD4 count estimation and clinical condition of the patient. 2 Initially, this classification was used to identify HIV-positive patients. The same classification was then used to identify patients requiring treatment.
Antiretroviral therapy (ART) has substantially decreased morbidity and mortality in HIV-infected persons. The optimal timing of initiation of ART has been difficult to determine because clinicians and patients have to weigh the benefits versus adverse effects of therapy. The World Health Organization (WHO) initially proposed a classification system based on clinical performance of the patient and basic laboratory investigations like total lymphocyte counts (TLCs). 3 At present, initiation of ART is based on clinical and immunological staging (absolute CD4 count). 4
Seth G. S. Medical College and K.E.M. Hospital, Mumbai, India is a 2288-bedded tertiary care public hospital and teaching institute that has been managing HIV-positive patients since 1989. It is one of the free ART centers in India. The Integrated Counseling and Testing center (ICTC) caters to more than 20 000 clients/patients annually. It also has facilities for estimating CD4 counts in HIV-seropositive patients.
The present study was conducted to determine the CD4 counts in different WHO clinical stages in ART-naive individuals to find out optimum CD4 count cutoffs for our population and to correlate between CD4 counts and TLCs.
Methods
Data of patients attending ICTC, K.E.M. Hospital over a period of 1 year were analyzed after obtaining institutional ethics committee approval. From the records, patients diagnosed as HIV-seropositive according to WHO HIV testing strategy III, coming for the first time during the study period, who were older than 15 years of age, and ART naive and whose WHO clinical stage was determined by the physician were included for analysis. The CD4 count estimation was done by flow cytometry (Beckton Dickinson, Franklin Lakes, NJ). Patient details such as sex, CD4 counts, and TLCs were noted. The severity of immunosuppression was graded based on WHO criteria. 5 For each WHO clinical stage, mean CD4 count and TLCs were determined. To establish the optimum CD4 cutoff values, receiver–operator characteristics (ROC) curves were generated for each WHO clinical stage. The CD4 count and TLCs were correlated by Spearman rank correlation.
Results
A total of 754 patients were included in the study. The CD4 counts in these patients ranged from 20 to 992 cells/mm3 with a mean of 241.20 cells/mm3 (±183.44). In all 65.8% were men, and when the patients were stratified by sex, though the women had higher counts than men, there was no significant difference (P > .05) in the CD4 counts in different WHO stages. Hence, stratification by sex was not further followed for analysis.
As per WHO clinical staging of HIV/AIDS, 5 51.8% were classified as belonging to stage I, 26.1% to stage II, 19.8% to stage III, and only 2.3% belonged to stage IV (Table 1). Mean CD4 counts showed a progressive decrease as the clinical stage increased. Mean CD4 count in stage III patients was observed to be 137.80 cells/mm3, which was significantly lower (P ≤ .05) when compared with patients in stage I (273.68 cells/mm3) and stage II (256.54 cells/mm3). The mean CD4 count in stage IV patients was 50.17 cells/mm3 and it was lower than all stages.
Laboratory Parameters in WHO Clinical Stages.
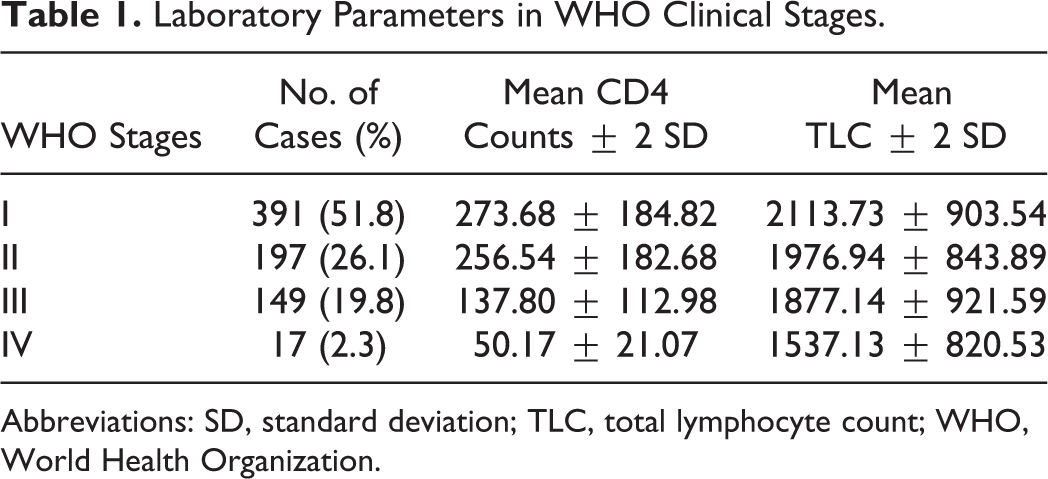
Abbreviations: SD, standard deviation; TLC, total lymphocyte count; WHO, World Health Organization.
A comparison of the severity of immunosuppression in patients in the different WHO stages (Table 2) revealed that 42.2% of the patients in stage I, 46.2% in stage II, and 82.6% in stage III could be classified as severe immunosuppression and 30.18% in stage I and 26.4% in stage II could be classified as advanced immunosuppression as per WHO criteria.
Immunosuppression in WHO Clinical Stages.

Abbreviation: WHO, World Health Organization.
Because of the disparity seen between clinical condition and severity of immunosuppression, the ROC curves were generated for WHO stage I, stage II, and combined stage III and IV to establish the optimum cutoff values for our population. The CD4 cutoff values of >280, 120 to 280, and <120 cells/mm3 were deduced from these curves.
To compare CD4 counts with TLCs, Spearman rank coefficient correlation was applied and was found to be weak (r = .32). A definite decreasing trend in TLC with disease progression as per WHO clinical stages was seen (Table 1), but it was not significant since the standard deviation was found to be scattered (P > .05).
Discussion
The CD4 count estimation in HIV-infected individuals is essential to help make decisions regarding disease staging, initiating opportunistic infections prophylaxis and ART, and in assessing the outcome of treatment. The National AIDS Control Organization (NACO), Government of India with WHO has started free ART centers across the country. Initiation of ART is recommended based on WHO staging and/or CD4 counts (<350 cells/mm3). 5
Of the 754 patients whose data were analyzed, 51.8% of the patients belonged to WHO stage I, thus indicating that asymptomatic patients are also availing ICTC services. In the years following the report of the first AIDS case from Mumbai in 1986, 6 mainly symptomatic patients came forward for diagnosis and treatment. But, because of increased awareness about the disease, more and more people with high-risk behavior are now coming forward in the asymptomatic period itself. This may denote a change in the health-seeking behavior in the community.
As per the WHO classification, 5 a total of 77.32% (583 of 754) of patients had advanced or severe immunosuppression (CD4 counts < 350 cells/mm3), and a majority (73.07%) of these belonged to stage I or II where advanced or severe immunosuppression was not expected. The ART is started for WHO clinical stage I or II only if CD4 counts are less than 350 cells/mm3. Being asymptomatic, without proper follow-up these patients would have been lost and would have missed on ART. Hence, the importance of regular CD4 count estimation in all HIV-positive patients irrespective of their WHO clinical stage should be stressed upon.
As some of the asymptomatic patients had advanced/severe immunosupression, ROC curves were generated and newer CD4 cutoff values, that is, >280, 120 to 280, and ≤120 cells/mm3, were inferred for stage I, stage II, and combined stage III and IV, respectively. These cutoffs had a significantly higher sensitivity and specificity compared with the existing cutoffs. Similar findings have also been reported by other Indian authors, such as Attili et al from North India (>280, 120-280, and ≤120 cells/mm3) 7 and Ramalingam et al from South India (>300, 81-300, and ≤ 81 cells/mm3) 8 and from authors in Asia and Africa. 9,10 There have also been reports of lower CD4 counts in the Indian population 7,8,11–13 and HIV-uninfected ethnic groups. 9,10 Also, India has a high burden of people living with HIV/AIDS (PLHA). 14 Considering these factors, lower cutoffs may be better for classifying immunosuppression in HIV-infected patients in our country.
Authors across the globe have reported contrasting findings on the association between TLCs and CD4 counts. 15 –21 In the present study, though a definitive decreasing trend in TLC was seen with disease progression, only a weak correlation was seen between CD4 counts and TLCs by spearman rank correlation (r = .32). The TLC, though economical, therefore cannot be used to monitor HIV-positive patients even in resource-limited settings. In their 2010 guidelines, the WHO no longer recommends TLC to guide treatment decisions in adults and adolescents. 4
A limitation of our study was its cross-sectional nature. Staging at a single visit may not adequately capture events that might have occurred prior to the study evaluation. Also, the WHO clinical staging depends a lot on gathering relevant clinical information from the patient and is therefore subjective. Hence, a prospective study is required wherein progression of HIV disease in all these asymptomatic patients is carried out.
Initiation and continuation of free ART in resource-limited settings presents a challenge. The majority of PLHA presenting at ICTC belong to the poor socioeconomic strata. Many of them are daily-wage laborers and every visit to the hospital is a loss of wage to them. According to USAIDS case study report of slums in India, the urban poor lack access to health care because they lack the means to pay for it. Also, the poor in India have great difficulty in comprehending the nature of their illness and understanding their course of treatment. 22 As the majority of the patients in our study had very low CD4 counts even in the asymptomatic stages they may miss out on treatment if CD4 counts are not estimated. The availability of regular CD4 counts estimation in PLHA, free of cost under the ART program initiated by NACO, is therefore a step in the right direction. 23
Footnotes
Acknowledgments
The authors wish to acknowledge Dr Amar Pazare, Professor and Head, Department of Medicine, Seth G.S.M.C. and K.E.M. Hospital, Dr M.H. Ansari, Associate Professor, Department of Pathology, Seth G.S.M.C. and K.E.M. Hospital, and Dr Kailash Gandewar, Biostatistician and Mumbai Districts AIDS Control Society.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.