
Abstract
The Joint United Nations Programme on HIV/AIDS (UNAIDS) Treatment 2015 calls for expanded access to HIV care and treatment, including cotrimoxazole preventive therapy (CPT), for prevention of HIV-related morbidity and mortality. We review 115 national guidelines from 92 countries for recommendations on CPT for adults and adolescents and determine the level of consistency with the World Health Organization (WHO) guidelines. Of the 66 countries with recommendations, 5 (8%) countries recommend lifelong CPT for people living with HIV; 19 (29%) countries recommend a CD4 count threshold of ≤350 cells/mm3 or WHO clinical stages III and IV or II, III, and IV; and 19 (29%) countries recommend a CD4 count threshold of ≤200 cells/mm3. Of the 48 countries with recommendations on discontinuing CPT, 25 (52%) countries recommend discontinuation of cotrimoxazole when the CD4 count is >200 cells/mm3. World Health Organization guidelines offer countries flexibility on the use of CPT, and countries are recommending a wide range of CD4 counts and WHO clinical stage criteria for prophylaxis initiation and discontinuation.
Introduction
An estimated 35.3 million people are living with HIV globally. 1 At the end of 2012, nearly 9.7 million people in low- and middle-income countries were receiving antiretroviral therapy (ART). 1 Despite the historic gains in expanding treatment, countries are facing significant challenges in achieving universal treatment access and engaging HIV-diagnosed individuals not yet “eligible” for ART in care. 1,2 The Joint United Nations Programme on HIV/AIDS (UNAIDS) recently launched the Treatment 2015 initiative to support countries to provide a comprehensive package of HIV testing, care, and treatment, including cotrimoxazole preventive therapy (CPT) for prevention of HIV-related infections. 2
Cotrimoxazole is a simple and well-tolerated intervention for prevention of pneumocystis pneumonia (PCP), toxoplasmosis, malaria, and bacterial infections and can be administered along with ART and tuberculosis (TB) treatment. Randomized controlled trials from sub-Saharan Africa have demonstrated the efficacy of cotrimoxazole in reducing morbidity, mortality, and hospitalization among people living with HIV, regardless of their CD4 counts and TB status. 3 -5 A recent meta-analysis also showed that CPT decreases the incidence of deaths by 58% among HIV-positive people on ART. 6 Cotrimoxazole is inexpensive, and a 6-month daily course of CPT costs about US$4. 7
The 2006 World Health Organization (WHO) guidelines on CPT include a degree of flexibility on CD4 count threshold and clinical disease stage for CPT initiation among adults and adolescents, including pregnant women. 8 Cotrimoxazole initiation is recommended at CD4 count ≤350 cells/mm3 or the WHO clinical stage III or IV, irrespective of the CD4 count. If the CD4 count is not available, cotrimoxazole is recommended at the WHO clinical stage II, III, or IV. Also, countries may opt for a CD4 count threshold of ≤200 cells/mm3 or may provide CPT irrespective of the CD4 count and clinical staging (universal option). Countries may discontinue CPT based on ART-related immune recovery (CD4 count ≥ 200 cells/mm3 or 350 cells/mm3 after at least 6 months of ART). Cotrimoxazole preventive therapy may not be discontinued in settings where bacterial infections and malaria are common HIV-related events. Routine CPT in all HIV-positive people with active TB disease, regardless of the CD4 count, is also recommended as an integral TB/HIV collaborative activity. 9 This article reviews the CPT initiation and discontinuation criteria in published national guidelines from 92 countries and determines the extent of consistency with the current WHO recommendations.
Methodology
From the UNAIDS database of national guidelines on ART, opportunistic infections (OIs), and HIV/TB collaborative activities, 10 guidelines were available for 92 countries and we reviewed them for recommendations on CPT. Using a standard data collection form, we abstracted recommendations on (1) CPT initiation criteria for people living with HIV, including pregnant women, those with active TB, and key populations, and (2) CPT discontinuation criteria. The recommendations were compared with the 2006 WHO guidelines on cotrimoxazole prophylaxis for HIV-related infections among children, adolescents, and adults. 8
Results
We reviewed 115 guidelines from 92 countries, dating from 2002 to January 2014. Antiretroviral therapy guidelines from all countries, HIV/TB guidelines from 16 countries, and OI guidelines from 7 countries were available. Of the 92 countries, with approximately 87% of the global HIV burden, 1 36 are from Africa, 24 from North and South America, 20 from the Asia-Pacific region, and 12 from Europe.
Cotrimoxazole Preventive Therapy Initiation Criteria
Of the 92 countries, guidelines from 66 countries have recommendations on CPT for people living with HIV (Table 1). Five (8%) countries with generalized HIV epidemics (Kenya, Malawi, Rwanda, Swaziland, and Uganda) recommend lifelong CPT for all people living with HIV, irrespective of their CD4 counts. A total of 19 (29%) countries recommend a CD4 count threshold of ≤350 cells/mm3 or the WHO clinical stages III and IV or II, III, and IV as the criteria for CPT initiation. Madagascar recommends CPT for people living with HIV with a CD4 count threshold of ≤350 cells/mm, 3 irrespective of the WHO clinical stage.
Recommendations on Cotrimoxazole Prophylaxis Eligibility Criteria for People Living With HIV (66 Countries).
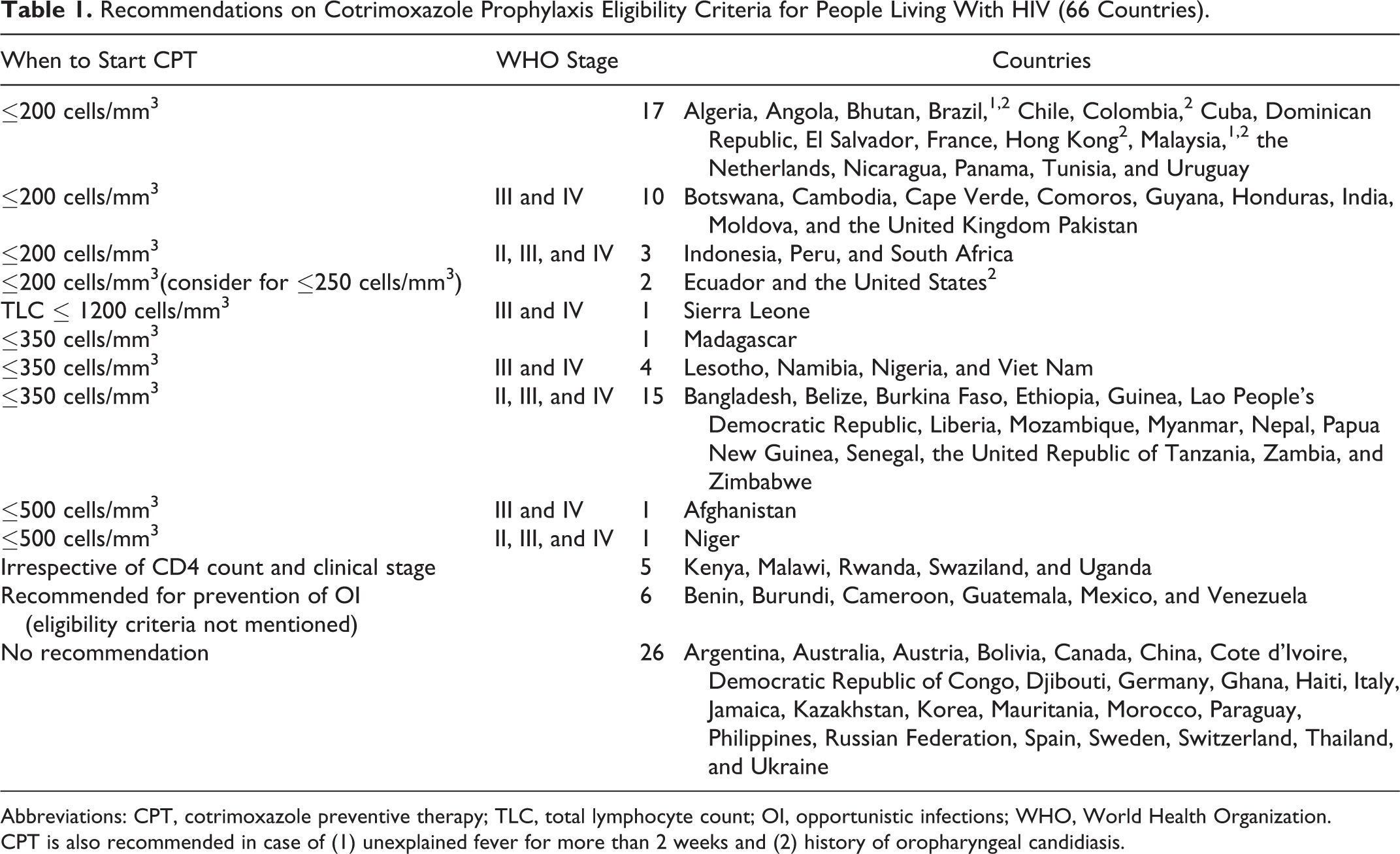
Abbreviations: CPT, cotrimoxazole preventive therapy; TLC, total lymphocyte count; OI, opportunistic infections; WHO, World Health Organization.
CPT is also recommended in case of (1) unexplained fever for more than 2 weeks and (2) history of oropharyngeal candidiasis.
In 19 (29%) countries, the main prophylaxis targets for CPT are PCP and toxoplasmosis, and these countries have adopted a CD4 count threshold of ≤200 cells/mm3 for which CPT is recommended. Of them, Ecuador and the United States recommend “considering” CPT for people living with HIV with CD4 count ≤250 cells/mm3. In the United States along with Brazil, Colombia, Hong Kong, and Malaysia, CPT is also recommended for those with a history of oropharyngeal candidiasis. Brazil and Malaysia additionally recommend CPT for people with unexplained fever for more than 2 weeks. In 13 (20%) other countries, CPT is recommended when the CD4 count threshold is ≤200 cells/mm3 or the WHO clinical stages III and IV or II, III, and IV.
Although the CD4 count testing is used as a standard to determine the eligibility for CPT, Senegal recommends CPT when the total lymphocyte count (TLC) is ≤1200 cells/mm3. Uruguay also recommends CPT initiation when the TLC is ≤1000 cells/mm3 in settings where the CD4 count testing is not available.
Initiation of CPT for pregnant women
Cotrimoxazole preventive therapy eligibility criterion for HIV-positive pregnant women is the same as that for other people living with HIV in all the 66 countries with CPT recommendations, except Liberia that recommends CPT for all HIV-positive pregnant women unless their CD4 counts are known to be ≥350 cells/mm3 consistently. Guinea, Mozambique, Niger, Nigeria, Senegal, Sierra Leone, and the United Republic of Tanzania recommend CPT for the eligible HIV-positive pregnant women after the first trimester.
Initiation of CPT for people coinfected with HIV and TB
A total of 39 countries recommend CPT for all people living with HIV having WHO stage III and IV illnesses, which include pulmonary and extrapulmonary TB. The HIV/TB guidelines from 12 of these countries have recommendation on CPT initiation, irrespective of the CD4 count, for HIV-positive patients with TB as a collaborative TB/HIV activity. Although the HIV/TB guidelines from Indonesia and the United Republic of Tanzania do not include specific recommendations on CPT, their ART guidelines recommend CPT against WHO stage III and IV illnesses.
Initiation of CPT for key populations
Malaysia recommends considering CPT, irrespective of the CD4 count, for high-risk populations (injecting drug users and sex workers) who typically present late with advanced disease and are less likely to have access to facilities with CD4 count testing capabilities.
Cotrimoxazole Preventive Therapy Discontinuation Criteria
Of the 92 countries, 48 have recommendations on discontinuing cotrimoxazole as prophylaxis among people with documented immune recovery (Table 2). Although 7 (15%) countries recommend continuing CPT indefinitely, other countries recommend a CD4 count-guided discontinuation for people living with HIV who are asymptomatic. Guidelines from 25 (52%) countries recommend discontinuation of cotrimoxazole when the CD4 count is >200 cells/mm3. A total of 19 (40%) countries recommend stopping CPT when the CD4 counts are more than 200 (9 countries) or 350 cells/mm3 (10 countries) on 2 separate measurements at least 6 months apart and are consistent with the WHO guidelines.
Criteria for Discontinuation of Cotrimoxazole Prophylaxis (48 Countries).

Abbreviations: CPT, cotrimoxazole preventive therapy; TLC, total lymphocyte count.
Discussion
The Treatment 2015 initiative is designed to support countries to expand access to HIV testing, care, and treatment as a stepping-stone to reaching the 15 million on treatment by 2015 target. Treatment 2015 identifies the importance of translating scientific evidence to new policy and practice and the necessity of speed to do so as a high priority for treatment expansion. 2 According to the recently released WHO 2013 ART guidelines, approximately 28.6 million people will be eligible for treatment, 1 many of whom will also be eligible for cotrimoxazole and isoniazid preventive therapies for prevention of HIV-related infections and tuberculosis, respectively. Reaching the treatment target will make a significant impact in preventing HIV-related illness and death and reducing HIV transmission. However, a considerable number of people living with HIV are lost to follow-up at each stage along the treatment cascade, resulting in substantial morbidity and premature mortality. 1,11,12 Cotrimoxazole as prophylaxis provides an important opportunity to not only reduce HIV-related morbidity and mortality but also improve retention rates and assess an individual’s adherence to treatment before ART initiation. 6,13,14
The WHO guidelines on cotrimoxazole prophylaxis include a degree of flexibility to enable countries to determine the most appropriate CPT initiation and discontinuation criteria depending on the local context. Indeed and perhaps not surprisingly, our review found that countries recommend a wide range of CD4 counts and WHO clinical stage criteria for prophylaxis initiation and discontinuation. Most countries are recommending CPT when the CD4 count is ≤200 or 350 cells/mm3 or irrespective of the CD4 counts and are consistent with the WHO guidelines. National policies, while reflecting WHO and other guidelines, are also influenced by operational and programmatic considerations. Although some countries recommend CPT when the CD4 count is ≤500 cells/mm3 or for people living with HIV having unexplained fever or a history of oropharyngeal candidiasis, CPT eligibility criterion is based on TLC in a few resource-limited settings/countries. More than 50% of countries recommend that people living with HIV receiving ART discontinue cotrimoxazole when their CD4 count is ≥200 cells/mm3. Although studies from resource-limited settings have reported no cases of PCP or toxoplasmosis, a recent study in Uganda showed that this discontinuation criterion increased the incidence of malaria and diarrhea in a malaria-endemic area. 15 -17 As part of its role of providing normative guidance, the WHO is in the process of systematically reviewing the evidence on when to start and stop CPT in different settings. This information is expected to be published in the 2014 update of treatment guidelines. The WHO is also considering fixed-dose combination of isoniazid, pyridoxine, and cotrimoxazole (sulfamethoxazole and trimethoprim) for inclusion in the essential medicines list. 18
Although there are clear national policies on the use of cotrimoxazole as prophylaxis, limited data are available to evaluate the status or impact CPT implementation. In 2012, an estimated 80% of identified HIV-positive TB patients were receiving CPT 19 ; however, data on CPT coverage among people living with HIV are not systematically collected. A cross-sectional survey in 69 countries found several gaps in nationwide implementation of CPT policies due to erratic supply and lack of stocks of cotrimoxazole, lack of awareness among health care workers, and perceived low priority of CPT because of the absence of reporting requirement. 20
Our policy review has a few limitations. Although we conducted a thorough search for the latest published national guidelines, some might be outdated or may be in the process of being updated. Also, other guidelines on cotrimoxazole may exist, but we failed to identify them. We used the 2006 WHO CTP guidelines as the reference point, and the epidemiologic, clinical, and public health situation has changed in many of the countries over the past 7 years. The study does not assess the effectiveness of policy implementation and the gap between policy and country reality.
Efforts to reduce HIV morbidity, mortality, and incidence through expanding access to treatment will require considerable efforts to improve all aspects of the treatment cascade, from HIV diagnosis to viral load suppression. Cotrimoxazole is of low cost and has significant individual and public health impacts including helping people living with HIV to remain healthy and in care. Our review of policy adaptation highlights some of the gaps in our evidence base and suggests that successful dissemination, speedy application, and monitoring implementation of CPT policies are needed to increase the uptake of this valuable intervention in most high burden settings as part of a comprehensive and strengthened response to HIV. The revision of national treatment targets and national ART policies to conform to the 2013 WHO consolidated guidelines on HIV treatment 21 offers a great opportunity to review the national CPT policy and the HIV/TB coinfection and HIV/hepatitis coinfection-related issues toward a more integrated approach to treatment.
Footnotes
Acknowledgments
The authors appreciate the contribution of experts from UNAIDS and WHO regional offices, the US Centers for Disease Control and Prevention, and Ministries of Health in providing them with the latest guidelines and valuable inputs on the policy recommendations.
Authors’ Note
RG and SG contributed to the development of conceptual framework. SG contributed to data abstraction and analysis. RG, PL, BH, and BS contributed reagents and materials. SG, RG, BH, PL, and BS were involved in drafting and writing the article; SG, RG, BH, PL, and BS contributed to the review of the final version. The opinions and statements in this article are those of the authors and may not represent the official policy, endorsement or views of the Joint United Nations Programme on HIV/AIDS (UNAIDS).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.