
Abstract
Empyema is a complication of pneumonia, characterized by pus accumulation in the pleural space. It is more common in patients with comorbidities such as older age, diabetes, cancer, or immunocompromised states. Aspiration or oral cavity infections are more common in older adults with significant risk factors; therefore, the pathogen Streptococcus constellatus is usually rare. S. constellatus is mainly known for its ability to produce abscesses and pyogenic invasive infections, with most of the infections being found in the orofacial and gastrointestinal regions. The patient is a 58-year-old female who presented with weakness, fatigue, nausea, anorexia, diarrhea, and subjective fever for two weeks. Investigation revealed that there was left-sided empyema, and the pleural fluid grew S. constellatus on culture. The management included antibiotics, chest tube drainage, and finally decortication. The patient’s recovery further demonstrates how rare and complex empyema caused by S. constellatus is in a healthy person.
Introduction
Empyema refers to infection and pus accumulation in the pleural cavity and is a well-known complication of pneumonia. It usually develops in patients with predisposing factors such as old age, diabetes, cancer, or immunodeficiency.1,2 Empyemas are usually polymicrobial and depend on the clinical scenario; however, oral bacteria are involved in aspiration-related ones. 3 Streptococcus constellatus is a member of the Streptococcus anginosus group (SAG) that resides in the oral, gastrointestinal, and genitourinary tracts; it can cause abscesses and invasive pyogenic infections. S. constellatus is rarely isolated as the only pathogen in empyema and is mainly associated with immunosuppressed patients3,4 or those with significant comorbidities, differentiating from the presented patient.
This article describes a case of a 58-year-old previously healthy immunocompetent female who developed a left-sided empyema due to S. constellatus. The case underscores the need to consider SAG infections in patients without conventional risk factors and the importance of early recognition and escalation of management when conservative therapy fails. 5
Case Presentation
A 58-year-old woman with no known past medical history was admitted to the emergency room with a 2-week history of presenting weakness, fatigue, anorexia, nausea, as well as diarrhea. She also complained of occasional subjective fevers without rigor, with no shivering. Her overall health status has worsened in the last 48-72 hours, which prompted her to seek medical attention. She worked as a jeweler with frequent exposure to dust and reported that a coworker had recently been diagnosed with pneumonia. She denied tobacco use, alcohol use disorder, intravenous drug use, or other risk factors for immunosuppression. HIV and diabetes testing were not performed during this admission.
Her initial vital signs included a temperature of 98.2 °F, heart rate of 117 bpm, blood pressure of 169/93 mmHg, and SpO₂ of 85% on room air, which improved to 98% on 3L nasal cannula. Laboratory results revealed a white blood cell count of 29.5 × 103/µL, normocytic anemia with a hemoglobin level of 10.3 g/dL, sodium level of 134 mmol/L, and potassium level of 3.5 mmol/L. Computed tomography (CT) of the chest (Image 1) demonstrated a substantial, loculated pleural fluid accumulation on the left side, strongly consistent with empyema. S. constellatus was the only bacteria detected in pleural fluid cultures. No polymerase chain reaction (PCR)-based methods were performed.
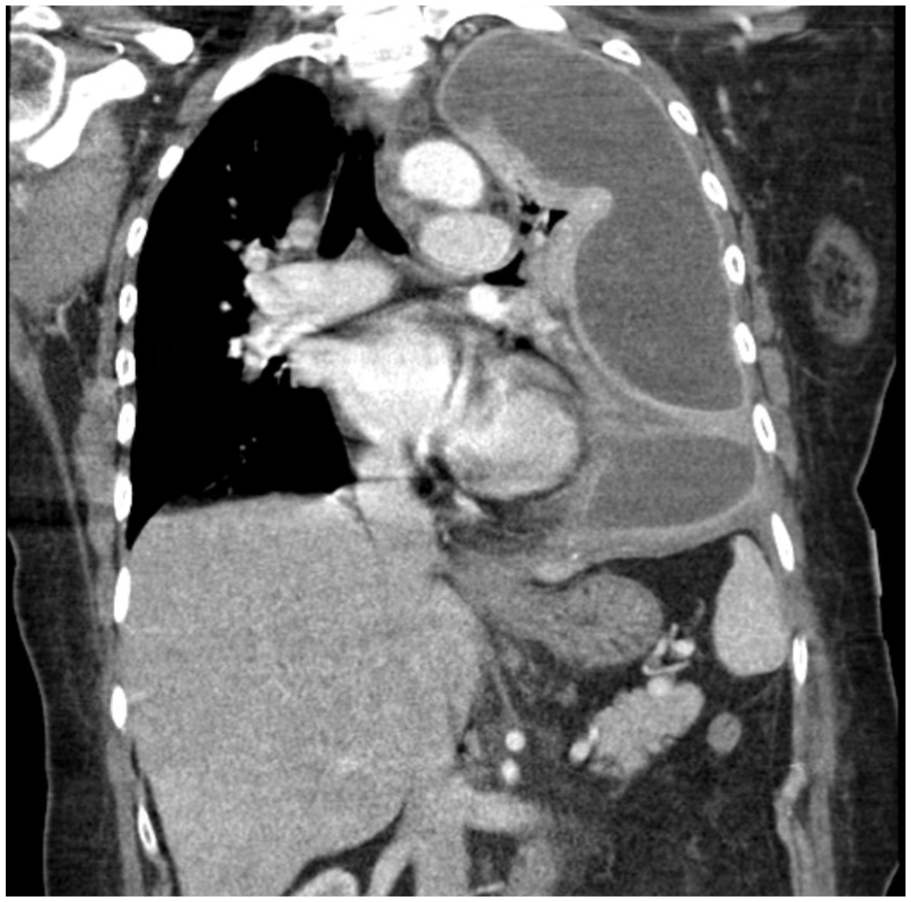
CT chest of empyema preoperatively.
The patient was started on empiric ceftriaxone, metronidazole, and linezolid, chosen to provide broad-spectrum coverage against community-acquired, anaerobic pathogens, and methicillin-resistant Staphylococcus aureus (MRSA), given her severe presentation. When her clinical status failed to improve, the regimen was escalated to cefepime to expand Gram-negative coverage, including for Pseudomonas. A chest tube was placed to drain the empyema, and intrapleural fibrinolysis with tPA-DNase was initiated, but these did not result in adequate drainage. As a result, the patient underwent a left thoracotomy accompanied by surgical decortication. Postoperationally, antibiotics were switched to only oral amoxicillin-clavulanate. Additional supportive care encompassed hypertension treatment with amlodipine, iron, and folate supplementation for anemia, dietary enhancement, and physical therapy. Her postoperative CT scan 4 days postadmission (Image 2) showed significant improvement compared to initial imaging. She was discharged to her home in stable condition with arrangements for outpatient follow-up and home health assistance.

Postresolution CT chest.
Discussion
An empyema develops when infection spreads from the lung parenchyma into the pleural cavity, progressing through the stages of exudative, fibrinopurulent, and organized. S. constellatus is a member of the S. anginosus group (SAG), a collection of facultative anaerobic bacteria that constitute the typical flora of oral cavity, gastrointestinal tract, and genitourinary system. These organisms are characterized by their ability to create abscesses due to their heightened mucosal invasiveness. 3 While pleural fluid cultures in this case detected only S. constellatus, conventional methods cannot fully exclude other pathogens; many fastidious organisms fail to grow in these cultures. Gram stain or molecular testing would provide stronger evidence for monomicrobial infection, but these were not performed.
High-resolution CT imaging is conventional for assessing pleural infections and planning for interventional therapy. Diagnostic thoracentesis is crucial, as pleural fluid usually exhibits low pH, low glucose, and elevated LDH levels in empyema cases. Conventional cultures, unfortunately, may not always identify causal organisms, while newer diagnostic techniques such as next-generation sequencing have demonstrated potential in certain contexts. 6
Empiric therapy should initially be broad spectrum, covering both aerobic and anaerobic organisms, then narrowed based on susceptibilities. S. constellatus typically exhibits a favorable response to beta-lactam antibiotics, 6 such as ceftriaxone and ampicillin/sulbactam. Antibiotic protocols should be customized with the availability of susceptibility data. Drainage upon recognition is critical, whether via chest tube insertion or surgical methods. Intrapleural fibrinolytics, such as tPA-DNase, can enhance results in loculated empyema, but this method requires more research backing. Surgical decortication is the final treatment for organized empyema that is resistant to the other conservative measures mentioned above. 6
Delayed diagnosis and management of empyema may lead to significant consequences, such as chronic fibrothorax, sepsis, bronchopleural fistula, and respiratory failure. Mortality may reach up to 20% 5 in patients with substantial comorbidities or postponed therapy. In our patient’s case, early identification, commencement of antibiotics, and appropriate surgical intervention led to clinical improvement and discharge in a stable state.
Conclusion
This case underscores the necessity of preserving a comprehensive differential diagnosis when assessing pleural infections, especially in individuals lacking traditional risk factors. Streptococcus constellatus, while an infrequent cause of empyema in immunocompetent individuals, necessitates prompt identification and care due to its aggressive characteristics and association with abscess formation. Prompt diagnosis, antibiotic therapy, and timely surgical intervention when warranted can markedly enhance outcomes, even in unusual presentations such as this. Management must still be individualized to the severity of infection, symptoms, and patient risk factors.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for Publication
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.