
Abstract
Venovenous (VV) extracorporeal membrane oxygenation (ECMO) for severe acute respiratory distress syndrome (ARDS) is initiated in patients with high mortality as a potential lifesaving intervention. Hematologic malignancy (HM) is considered a relative exclusion criterion by the Extracorporeal Life Support Organization (ELSO). This case examines the relative contraindication and presents a successful outcome. A healthy 59-year-old male presented with respiratory distress. On arrival his S
Introduction
VV-ECMO for Severe ARDS: Historical Exclusion Criteria
Venovenous (VV) extracorporeal membrane oxygenation (ECMO) is a well-established therapy for severe acute respiratory distress syndrome (ARDS). This therapy requires considerable resources and is initiated in patients with high mortality as a potential lifesaving intervention. It is therefore vital to clearly define specific inclusion and exclusion criteria. Active malignancy was historically considered an absolute exclusion criterion by the Extracorporeal Life Support Organization (ELSO). 1 Evolving evidence has continued to suggest that there are subsets of patients with an active malignancy that may benefit from this therapy leading to use in select patients. Of note, pediatric ELSO centers generally do not consider malignancy to be an absolute contraindication to ECMO. 1 Pediatric ECMO indications will not be discussed in this article.
Several recent studies have examined the outcomes for patients with an active malignancy who were treated with VV-ECMO for severe ARDS. A retrospective multicenter study published in 2018 examined long-term outcomes for this population with data taken from 2008 to 2015. 2 This cohort study demonstrated a higher 6-month survival if malignancy had been diagnosed within the last 30 days compared with those with a more chronic diagnosis. 2 In fact, a malignancy diagnosed in the last 30 days was not a pre-ECMO predictor of mortality. 2 Hematologic malignancies (HMs) were demonstrated to have a lower survival at 60 days (27.4%. n = 62) compared with malignancies of other origin (33.3%, n = 39). 2 A smaller study done in 2014 demonstrated a 50% (n = 14) survival rate in patients with HMs. 3 A 2010 publication reported the survival rate to be 32% (n = 72). 4 The most recent 5-year data reported to ELSO demonstrated that overall, the survival in the oncologic population requiring VV-ECMO is 5% to 10% less than controls.1,5,6 Due to the increasing body of literature demonstrating potentially favorable outcomes, active malignancy is now considered to be a relative exclusion criterion by the ELSO.1,5,6
Hairy Cell Leukemia
Hairy cell leukemia (HCL) is a rare, small B-cell lymphoid neoplasm that gets its name from irregular cytoplasmic projections demonstrating a “hairy” appearance on electron microscopy. 7 The estimated annual incidence is 3 cases per one million people in the United States. 8 The prognosis with this disease is favorable. Asymptomatic individuals often do not require early therapy in any form. Treatment is reserved for patients meeting select criteria including severe cytopenia, symptomatic lymphadenopathy, or significant constitutional symptoms affecting the patient’s quality of life. 9 When treatment is indicated, a single cycle of the purine analogue cladribine has demonstrated a 10-year survival of 100% and a complete cure rate of 76%.10,11
HCL and Legionella Pneumonia
Immunosuppression is a known risk factor for Legionella pneumophilia infection. Htwe and Khardori in 2017 reported that HCL has the highest association with Legionella of the hematological malignancies. 12 Severe monocytopenia with reduced activation is thought to be the driving cause leading to increased risk for all intracellular pathogens.3,12 Literature review returned a single case of a patient with a new diagnosis of HCL that was treated with VV-ECMO for severe ARDS. This patient presented with severe ARDS secondary to L pneumophilia, was successfully treated, decannulated, and later reached hematologic remission. 13
Antibiotic Duration for Severe Legionella Pneumonia
With the evolution of available antibiotic therapies, the mortality rate of Legionella pneumonia has improved from 34% in 1980 to as low as 3.1% in one 2010 study. 14 In the United States, therapy is typically either with azithromycin 500 mg daily or levofloxacin 750 mg daily for a duration of 7 to 10 days if pneumonia severity index is greater than 2. 15 Azithromycin is generally the preferred adjunctive agent at our institution when a patient is treated for community-acquired pneumonia with broad-spectrum antibiotics based on the most recent guidelines. 16 A meta-analysis published in March 2021 did demonstrate superiority of fluoroquinolones over macrolides in hospitalized patients with Legionella 17 ; however, our case pre-dates this publication and societal guidelines have yet to adopt this finding into a recommendation.
Duration of therapy is subject to debate in patients who are immunosuppressed. Most of the current literature on duration of antibiotic therapy in this population is based on retrospective review of transplant recipients and not specific to HMs. 18 To both treat active disease and prevent relapse, a duration of 14 days is typically recommended but there are some resources that recommended as long as 21 days of therapy. 19 The VV-ECMO has not been shown to have a significant effect on the pharmacokinetics of azithromycin; however, data are limited to a total of 3 patients. 20
Case
A 59-year-old male with no known past medical history presented to the Emergency Department (ED) with 5 days of worsening dyspnea, fever, nonproductive cough, and diarrhea. The patient reported that symptoms had been rapidly progressing since initial onset. He denied any past medical history and reported no daily medications or supplements. He had not seen a physician in several years. Three days prior to the ED visit, he was seen at an urgent care center where COVID-19 testing was reportedly negative. During the pandemic he worked as a bartender at a hotel close to the airport with multiple potential COVID-infected contacts but no confirmed exposures. He denied any household or close sick contacts. Recent travel included a trip to Florida where he had vacationed at a condo located on the beach. He described his cough as nonproductive and was increasing in frequency since initial onset. He reported that the shortness of breath had gotten to the point where he was no longer able to speak in full sentences which is what prompted his visit to the ED.
In the ED his initial vital signs were notable for pulse oximetry (S

Progression of pulmonary infiltrates during hospitalization: (A) Initial chest x-ray on Emergency Department presentation; multifocal airspace opacities, dense right lower lob opacity; (B) HD 0 following intubation for hypoxic respiratory failure—consolidation throughout middle and right lower chest, endotracheal tube 6.6 cm above carina (advanced at time of radiograph); (C) HD 1 following ECMO cannulation; multifocal airspace consolidation, right greater than left, ECMO cannulas at the superior vena cava atrial confluence and inferiorly at T10; (D) HD 2—near complete opacification of the right hemithorax; (E) HD 5—dense bilateral airspace disease, right greater than left; (F) HD 7—complete opacification of the left hemithorax; (G) HD 13—left greater than right pleural effusions, bilateral perihilar opacities; (H) HD 21—midlung opacities present bilaterally, improved pleural effusions; and (I) HD 30 following tracheostomy; increased airspace opacities throughout both lungs, slightly decreased right pleural effusion, tracheostomy tube now in place.

Axial and coronal slices of computed tomographic angiogram chest. Computed tomographic angiogram of the chest taken at time of admission. The study did not demonstrate a filling defect consistent with pulmonary embolism, but it did demonstrate multifocal pneumonia with complete opacification of right middle and lower lobes.
The patient was admitted to the intensive care unit (ICU) with a working diagnosis of community-acquired pneumonia in the setting of suspected immunodeficiency. Azithromycin was added to cefepime and vancomycin for atypical pneumonia coverage. He continued to decompensate requiring intubation for worsening hypoxia on hospital day (HD) 0 shortly after admission. Postintubation chest x-ray demonstrated rapidly progressing opacities now involving most of the right hemithorax (Figure 1). The initial postintubation arterial blood gas demonstrated a PaO2/FiO2 ratio of 54, and his Murray Score for lung injury was 2.8 indicating ARDS. He was treated with low tidal volume ventilation, neuromuscular blockade, and inhaled epoprostenol. These measures resulted in a small improvement in oxygenation with a new PaO2/FiO2 ratio of 74.
The ECMO service was consulted for VV-ECMO evaluation shortly after intubation on HD 0. Given his preserved static compliance on the ventilator, decision was made to attempt continued ventilator optimization and prone positioning prior to cannulation. However, there was minimal improvement overnight, thus patient was cannulated on VV-ECMO on HD 1. The patient is 5′6″ and weighed approximately 70 kg at the time of admission. Cannulation was done using a single lumen 20F return cannula in the right jugular vein and a 25F multistage drainage cannula in the right femoral vein.
On HD 0 the initial blood smear was reviewed by pathology and demonstrated atypical lymphocytes with irregular cytoplasmic projections concerning for HCL. HIV testing was negative. The initial blood smear and subsequent flow cytometry returned the diagnosis, so further investigation into immunodeficiency was not pursued. On further discussion with the patients’ spouse, the patient had been demonstrating increasing fatigue with any exertion over the past 2 years. However, the spouse denied other constitutional symptoms prior to this illness. Flow cytometry was performed confirming the presence of mature, kappa-restricted B cells, CD 20+, CD5−, CD23−, with additional hairy cell testing confirming CD11c+, CD25+, and CD103+. B-lymphoid cells comprised 93% of all lymphoid cells. All these findings confirming a diagnosis of HCL on HD 1. While diagnosis was confirmed by cytometry on HD 1, this resulted following the decision to initiate VV-ECMO. The HCL was considered highly likely at time of cannulation based on peripheral blood smear. Molecular testing later in the admission confirmed BRAF mutation V600E. Oncology was consulted for new diagnosis of HCL and followed during hospitalization. While there was no indication for acute treatment of the malignancy, the patient was started on filgrastim for severe neutropenia.
This initial ICU course was complicated by intermittent atrial fibrillation with rapid ventricular response (AF with RVR) requiring chemical and electrical cardioversion, acute renal failure requiring continuous renal replacement therapy, recurrent pulmonary hemorrhage, and vasodilatory shock. The patient required vasopressor support with norepinephrine shortly after intubation on HD 0 with dosing increased to as high as 26 μg/min. Vasopressin was added at 0.03 u/min. After initiation of VV-ECMO, the patient required additional vasopressor support and phenylephrine was added. Tachyarrhythmias improved with the addition of phenylephrine and subsequent decrease in norepinephrine dosing. Hemodynamic instability quickly resolved, and the patient was weaned off all vasopressors by HD 4. Distributive shock state was attributed to severe infection, metabolic acidosis from renal failure, and the secondary inflammatory response commonly seen with the initiation of ECMO.
Broad-spectrum antibiotics were continued including atypical coverage with azithromycin during the first week of hospitalization. On HD 5, L pneumophilia serogroup 1 urine antigen resulted positive confirming diagnosis. Azithromycin was continued for a total of 14 days. The indication for extended duration was severe infection in the setting of immunocompromised state.15,19-22 After 14 days of therapy, the patient continued to be afebrile, without leukocytosis, with minimal secretions, and hypoxia was largely attributed at that point to pulmonary hemorrhage and not secondary to active infection.
The first week of hospitalization was complicated by an acute decompensation with increasing hypoxemia secondary to pulmonary hemorrhage on HD 6. The patient had a dramatic decrease in oxygenation requiring increasing VV-ECMO flow rates to a near critical level of 6.5 lpm and then 7 lpm overnight into HD 7 (Table 1). Bronchoscopy confirmed the presence of extensive blood clots with debris in all segments of the tracheobronchial tree. Cryotherapy was performed with large volume extraction of clots and subsequent improvement in oxygenation. During the hospitalization the patient required 5 total bronchoscopies (HD 6, 17, 21, 23, and 27) with cryotherapy for similar episodes which continued to impede his pulmonary recovery.
Evolution of Pertinent Laboratory Data During ICU Course.
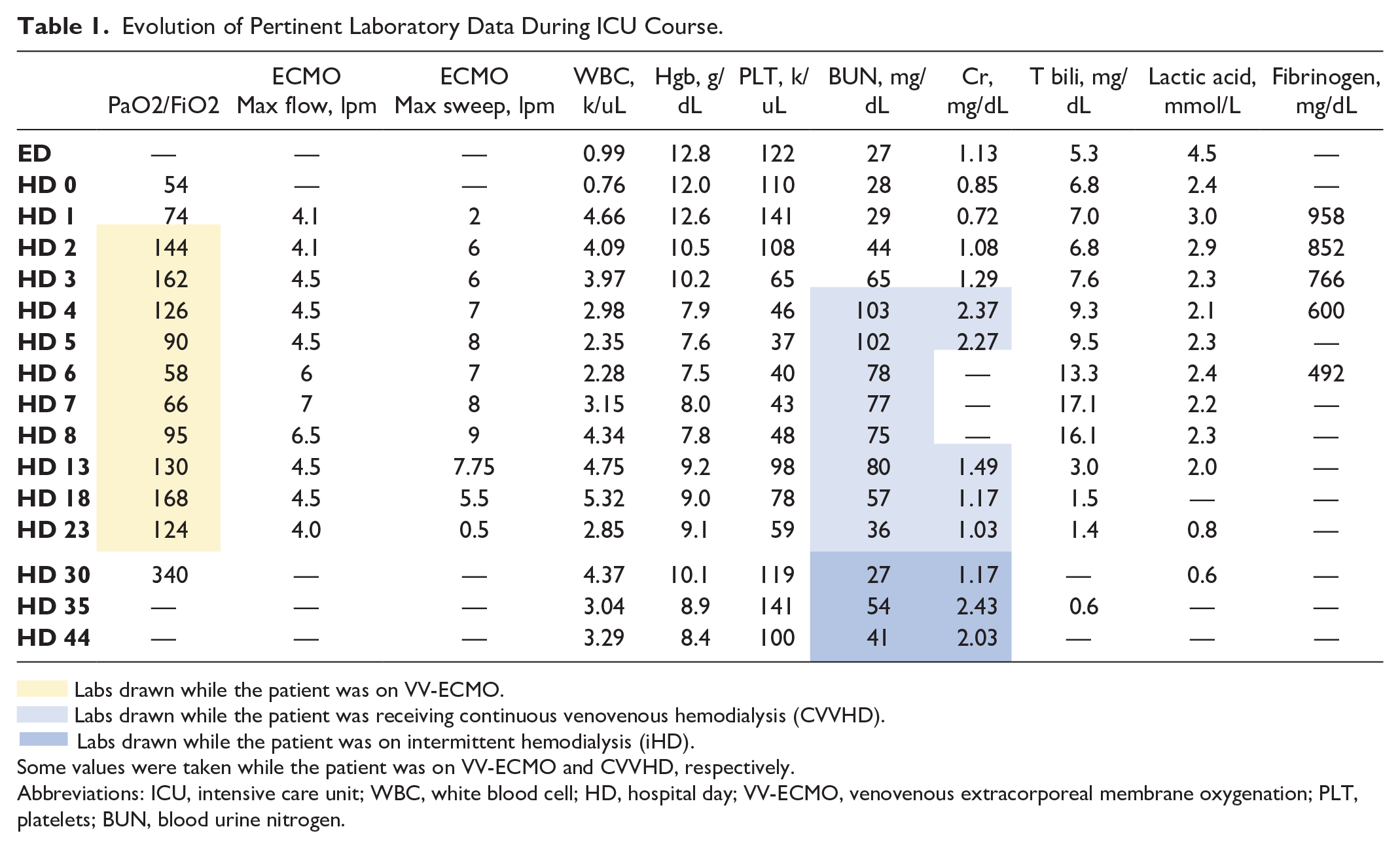

 Labs drawn while the patient was on VV-ECMO.
Labs drawn while the patient was on VV-ECMO.
 Labs drawn while the patient was receiving continuous venovenous hemodialysis (CVVHD).
Labs drawn while the patient was receiving continuous venovenous hemodialysis (CVVHD).
 Labs drawn while the patient was on intermittent hemodialysis (iHD).
Labs drawn while the patient was on intermittent hemodialysis (iHD).
Some values were taken while the patient was on VV-ECMO and CVVHD, respectively.
Abbreviations: ICU, intensive care unit; WBC, white blood cell; HD, hospital day; VV-ECMO, venovenous extracorporeal membrane oxygenation; PLT, platelets; BUN, blood urine nitrogen.
The initial episode of pulmonary hemorrhage resulted in the decision to hold systemic anticoagulation. Coagulopathy was thought to be multifactorial in the setting of thrombocytopenia, uremia, severe sepsis, as well as systemic anticoagulation. At the time of the initial pulmonary hemorrhage, the platelet count was 40 k/uL and BUN (blood urine nitrogen) was 78 mg/dL (Table 1). Following the initial hemorrhagic episode, the patient remained off anticoagulation for 22 of the total 27 days on VV-ECMO. The patient did not experience any thrombotic complications in vivo, within the ECMO circuit, or within the dialysis circuit.
On HD 7 ventilation was transitioned to airway pressure release ventilation from pressure control with improvement in oxygenation and lung compliance. On HD 10 the patient developed a maculopapular, erythematous, blanching, rash on neck, chest, and lower abdomen (Figure 3) which was later attributed to either the Legionella infection itself or a drug reaction secondary to filgrastim. Filgrastim was discontinued after resolution of neutropenia.

Maculopapular rash.
On HD 21 he developed increasing midlung opacities compared with previous radiographs (Figure 1). At that time the patient was started on empiric cefepime as well as vancomycin to cover for potential ventilator-associated pneumonia. However, both respiratory and blood cultures remained negative. The midlung infiltrates improved with volume removal on hemodialysis so the infiltrates were thought to be cardiogenic over infectious and antibiotics were discontinued after 3 days of empiric coverage. The patient did not experience any secondary infectious complications during his extended hospitalization.
The patient’s respiratory recovery was blunted by continued intermittent episodes of pulmonary hemorrhage. However, gradually lung mechanics and oxygenation began to normalize. The patient was decannulated on HD 27 for a total of 26 circuit days. Tracheostomy was performed on HD 28 and the patient was successfully weaned from mechanical ventilation.
On HD 44 he was transferred to the medical floor. Ongoing medical problems at that time included renal failure requiring continued intermitted hemodialysis, HCL, thrombocytopenia, physical deconditioning secondary to prolonged immobilization, A-Fib, and intermittent encephalopathy as expected with a prolonged ICU course. The HCL was not treated during this acute hospitalization in accordance with oncology recommendations. The continued thrombocytopenia was attributed to both active HCL as well as bone marrow suppression secondary to severe infection.
The patient’s oxygen requirement was approximately 10L via tracheostomy collar at time of transfer to the medical floor. Generalized muscle weakness continued to improve with aggressive physical therapy. Following continued management on the medical floor he was transitioned to an acute rehabilitation facility. At time of discharge, he was consistently requiring less than 4L oxygen via tracheostomy collar. After a brief stay at rehabilitation, he was transitioned home without the requirement of home oxygen.
At follow-up visits with oncology as well as with this provider, he was noted to have made a complete neurologic recovery. He returned to the hospital for one cycle of cladribine which was started 4 months after the initial presentation to the hospital. Repeat bone marrow biopsy following chemotherapy demonstrated no gross evidence of disease with tentative plan to repeat testing at the 12-month time interval.
Discussion
VV-ECMO in the Setting of HCL
This case demonstrates an example of a patient with severe ARDS secondary to Legionella pneumonia that was successfully treated with VV-ECMO in the setting of newly diagnosed HCL. It has been demonstrated historically that HMs generally portray worse outcomes in the setting of VV-ECMO, leading to the previous absolute and more recently relative contraindication of active malignancy. As more patients are treated with this resource-intensive therapy, the body of evidence continues to evolve. The ECMO clinician should adjust practice patterns accordingly with new literature, especially when evaluating trajectory and potential outcomes. With such a wide spectrum of disease, it is important to prognosticate each patient individually.
Patients with severe ARDS secondary to Legionella pneumonia have a high chance of survival when treated early with VV-ECMO. One large ECMO center in the United Kingdom reported a survival rate of 84% over a 10-year period in this subgroup. 23 In 2014, a large ECMO center in the United States reported a survival to discharge rate of 67% with similar methodology over a 10-year period. 24
The HCL, while relatively rare, has high rates of cure and portrays an excellent prognosis. A single dose of cladribine has been demonstrated to cause complete remission in 91% of patients with a 10-year survival as high as 100%.10,11,25 This specific form of HM should not be considered a relative contraindication to ECMO based on prognosis alone. However, as this is only the second case from this specific population reported in the literature, more data are needed to confirm this hypothesis. The ECMO clinicians should additionally be reassured if HCL is a new diagnosis within the last 30 days, as this has been previously demonstrated to not be associated with increase mortality. 2 It should be noted that confounding thrombocytopenia, anemia, and coagulopathy often co-exist with HCL which places patients in a higher risk category regarding the cannulation and maintenance on the ECMO circuit.
A multidisciplinary discussion was had prior to the initiation of VV-ECMO in this case. The decision was ultimately made to proceed due to the high rates of cure of HCL, excellent prognosis, and lack of additional comorbidities. As more cases similar to this one are reported, recommendations regarding ECMO will likely adapt and grow to support its use in this patient population.
Severe Legionella: Risk Factors and Treatment Duration
The COVID-19 pandemic has changed the way people live. With changing behaviors comes changing epidemiologic risk factors for all disease, particularly those that are infectious. Outbreaks of Legionella are known to be associated with contaminated water systems including those found in hotels, hospitals, cruise ships, and apartment buildings. This patient had 2 potential sources of exposure having both worked at a hotel during a pandemic as well as briefly living at a condominium while traveling to Florida. Literature has started to emerge about the increasing prevalence Legionella and potential exposure risk of stagnant water systems related to the COVID-19 pandemic and systemic lockdown.26,27
The duration of antibiotic therapy indicated for severe Legionella infection in the setting of immunosuppression is based on low-level evidence. The patient in this case was treated for 14 days with 500 mg IV azithromycin. Based on best available evidence and overall clinical improvement, the decision was made to not extend therapy past 14 days. While difficult to quantify compared with other patients presenting with severe disease, this patient had a postintubation PaO2 to FiO2 ratio of 54, an absolute neutrophil count of 0.46 k/uL, and an absolute monocyte count of 0.00 on admission. While his hospitalization was extended and complicated, 14 days of therapy was sufficient to treat the Legionella infection without any infectious recurrence or extrapulmonary manifestations. This would support a 14-day course of therapy being sufficient for treatment of severe Legionella in an immunosuppressed state. The VV-ECMO did not appear to impact the efficacy of azithromycin therapy based on clinical response including defervescence, lung mechanics, and lack of disease recurrence.
HCL and Severe Legionella
The association between HCL and Legionella pneumonia has been previously hypothesized to be related to impaired monocyte activation.3,12 This patient presented with an absolute monocyte count of 0.00 leaving him at an increased risk for intracellular pathogens. While the association is purely speculative based on physiology, this presents another example to a growing body of evidence.
Conclusion
This case represents a patient who presented with severe ARDS secondary to Legionella pneumonia in the setting of a newly diagnosed HCL. He presented in an immunocompromised state with an absolute monocyte count of 0 and severe leukopenia. While his initial hospital course was tenuous as his disease progressed, he was successfully treated with VV-ECMO, decannulated, weaned from mechanical ventilation, and eventually discharged to acute care rehabilitation. Following a brief stay at rehabilitation he was discharged home having made a complete neurologic and respiratory recovery. He presented to oncology 4 months after discharge for inpatient chemotherapy and is in full remission.
The VV-ECMO is a resource-intensive treatment modality for those meeting specific criteria but reserved for patients with the highest probability of survival. This case is an example of a good outcome in a patient who would not have been considered for this lifesaving modality had he been evaluated purely based on guidelines. This report emphasizes the need to evaluate each case individually. While active malignancy remains a relative exclusion criterion listed by the ELSO, those with a high chance of remission should not be considered a contraindication. It is important to analyze the disease process for each patient individually and make decisions based on evolving bodies of evidence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.