
Abstract
McCune-Albright syndrome (MAS) is a rare disorder, occurring in 1 in 100 000 to 1 in 1 000 000 live births, caused by post-zygotic somatic mutations in the GNAS gene. This leads to fibrous dysplasia (FD), café-au-lait (CAL) skin pigmentation, and hyperfunctioning endocrinopathies. We present a 32-month-old girl with recurrent vaginal bleeding, bilateral breast enlargement, and multiple irregular CAL spots crossing the midline. Imaging revealed ovarian cysts and skeletal lesions consistent with FD. Laboratory findings indicated gonadotropin-independent precocious puberty. A clinical diagnosis of MAS was made, and genetic testing was deemed unnecessary. MAS presents with variable severity, and early diagnosis requires clinical recognition of its hallmark features. Genetic testing can support the diagnosis, though its reliability may vary due to mosaicism. Management is symptomatic, focusing on controlling endocrine dysfunction and minimizing skeletal complications. Emerging therapies offer promise, but no definitive cure exists. Early recognition and management are crucial for optimizing outcomes.
Introduction
McCune-Albright syndrome (MAS) is a rare condition marked by the distinctive combination of fibrous dysplasia (FD) of bone, café-au-lait (CAL) skin spots, and hyperfunctioning endocrinopathies. 1 It is estimated to occur in 1 in 100 000 to 1 in 1 000 000 live births. 2 Severity varies based on tissue involvement. 3 Precocious puberty (PP) and painless vaginal bleeding are commonly the first signs of MAS. These symptoms occur because of the activation of gonadotropin receptors in the ovaries, despite the absence of gonadotropin stimulation. This leads to ovarian enlargement, cyst formation, and the secretion of estradiol, which triggers early puberty and abnormal vaginal bleeding. 4 Diagnosis is primarily clinical, requiring at least 2 features of the triad, supported by hormonal tests and imaging. Genetic testing for GNAS mutations can confirm the diagnosis but is not always necessary. 2 The goal of treatment is to block the production of sex steroids and reduce their peripheral effects, such as the development of puberty, menstruation, and the advancement of bone age. A multidisciplinary approach involving endocrinologists, orthopedic surgeons, and geneticists is essential for long-term management and monitoring. 1
Case Presentation
A 32-month-old girl presented with a 2-month history of mucoid whitish vaginal discharge that was mixed with fresh blood. She is a product of a full-term gestation and delivered by cesarean section, with a weight 2.4 kg. She had appropriate developmental milestones and vaccinations. She had bilateral breast enlargement from birth which was stable until she developed vaginal bleeding. There was no history of urinary tract infection (UTI) symptoms, trauma, or medication use.
On physical examination, she demonstrated normal growth and development. Multiple irregular border CAL spots were noted on her back with the biggest being 6 cm and crossing midline (Figure 1). She has bilateral breast enlargement (Tanner stage II) in the absence of axillary and pubic hair (Tanner stage I; Figure 2). There were no signs of organomegaly or skeletal deformity and her neurological assessment was normal.

Café-au-lait macules on the patient’s back. The lesions exhibit irregular borders and are distributed asymmetrically, with several extending across the midline.

Clinical photograph showing bilateral breast development consistent with Tanner Stage II in a 32-month-old girl.
Laboratory results including complete blood count showed a Hb level at 11.1 g/dL; additionally, her serum creatinine value was normal at 0.3 mg/dL. Her urinalysis indicated a presence of 8 WBCs and urine culture was positive for Escherichia coli. An endocrine evaluation, including luteinizing hormone, follicle-stimulating hormone, thyroid-stimulating hormone, and prolactin levels, was conducted, with the results summarized in Table 1.
Results of Endocrine Evaluation Showing Serum Levels of LH, FSH, TSH, and Prolactin.
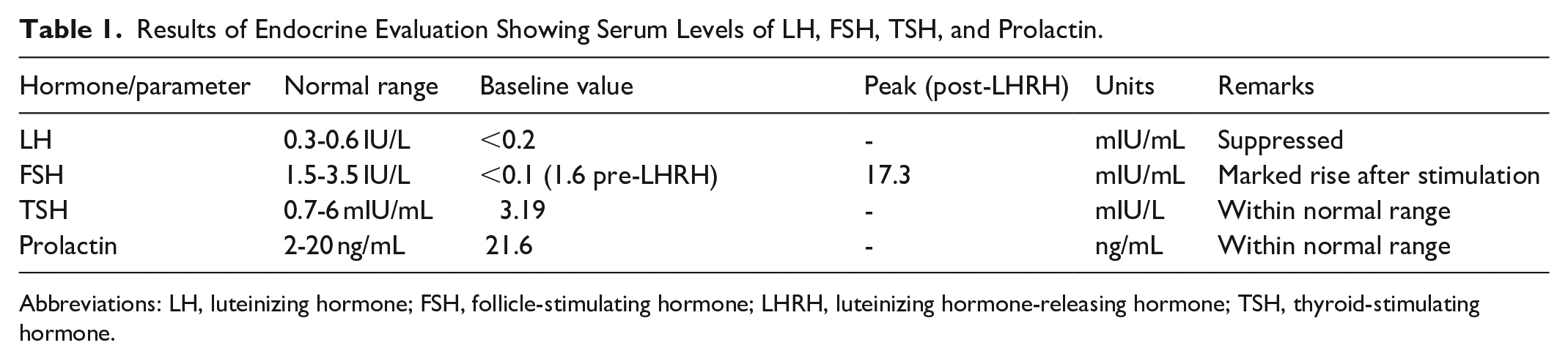
Abbreviations: LH, luteinizing hormone; FSH, follicle-stimulating hormone; LHRH, luteinizing hormone-releasing hormone; TSH, thyroid-stimulating hormone.
Breast ultrasound showed bilateral gynecomastia, and the pelvic ultrasound identified a 3.4 × 3.2 cm left ovarian cyst. Computed tomography scan confirmed a 3.0 × 4.5 cm cyst located posterior to the uterus (Figure 3). A magnetic resonance imaging of the brain showed no remarkable features while a bone age X-ray matched the chronological age of 2.9 years. On skeletal imaging, there were multiple lytic and sclerotic lesions of the distal radius as well as FD with a “copper beaten” skull (Figure 4).

Axial CT scan of the pelvis showing a well-circumscribed, hypodense cystic lesion posterior and lateral to the bladder (red circle), consistent with a left ovarian cyst. CT, computed tomography.

X-ray of the patient’s left forearm demonstrating a lytic lesion in the distal radius with a ground-glass matrix and cortical thinning (red circle), characteristic of fibrous dysplasia associated with McCune-Albright syndrome.
The patient was started on Cefixime for the treatment of UTI, which resulted in resolution of the vaginal bleeding. However, the symptoms returned after the antibiotics were stopped. With the combination of PP and CAL spots, FD was diagnosed along with MAS. Genetic testing for GNAS mutation was not carried out because of the costs and minimal benefits.
She continues to be followed up by endocrinology and orthopedics and is being tracked for her hormone levels, ovarian cysts, and bone lesions as they progress to determine further treatment.
Discussion
MAS was described by McCune in 1936 and Albright in 1937, with FD defined by Lichtenstein and Jaffe in 1942.5,6 Mutations in the GNAS gene impair the subunit’s GTPase activity, leading to continuous receptor activation and excessive cAMP production, contributing to MAS. 3 Mosaicism accounts for the diverse of clinical manifestations of MAS. 7
MAS present variably, with FD being one of its hallmark features. FD is a progressively bone disorder in which normal bone is replaced by immature fibrous tissue, leading to skeletal fragility and deformities. It can affect a single bone (monostotic) or multiple bones (polyostotic) and often presents with localized bone pain, swelling, pathological fractures, and skeletal abnormalities. Studies indicate that bone pain occurs in up to 81% of adults and 49% of children with FD. 8 In our case, the patient did not report significant bone pain at the time of presentation. Skeletal imaging showed lytic and sclerotic lesions in the radius, and a “copper beaten” skull, more linked with increased intracranial pressure rather than FD.
Craniofacial FD is one of the most commonly affected area, often associated with diffuse thickening of the craniofacial bones and poor gasification of the sinuses, which can lead to facial deformities, hearing impairment, and nasal congestion. 2 However, in this case, there was no evidence of craniofacial FD, and the patient did not present with symptoms such as increased intracranial pressure, diplopia, or hearing loss at the time of diagnosis.
CAL spots typically have irregular borders, commonly found in the neck and buttocks, rarely cross the midline, and often are the first sign to appear. 1 In this case, an examination revealed that the patient’s CAL spots were located on the back and extended across the midline. It is important to remember that CAL are not particular symptoms of MAS; rather, they are also associated with other syndromes. Table 2 summarizes syndromes associated with CAL.
Syndromes associated with Café-au-lait.
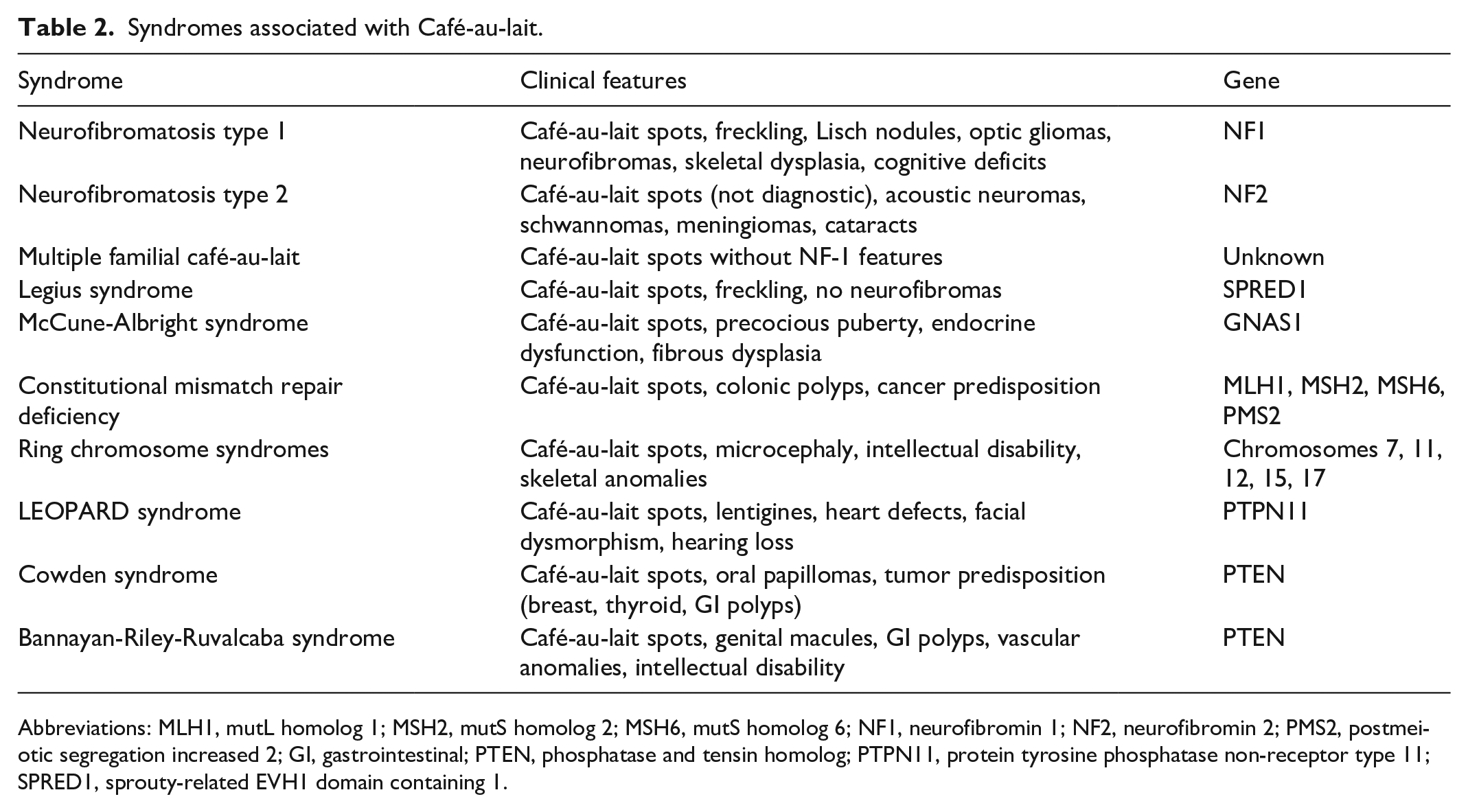
Abbreviations: MLH1, mutL homolog 1; MSH2, mutS homolog 2; MSH6, mutS homolog 6; NF1, neurofibromin 1; NF2, neurofibromin 2; PMS2, postmeiotic segregation increased 2; GI, gastrointestinal; PTEN, phosphatase and tensin homolog; PTPN11, protein tyrosine phosphatase non-receptor type 11; SPRED1, sprouty-related EVH1 domain containing 1.
Endocrine dysfunction in MAS includes PP, Cushing syndrome, hyperthyroidism, excess growth hormone (GH), in addition to other manifestations. The most distinctive of these is PP, which is common in female patients, typically presents with vaginal bleeding, and breast development. However, it is rare in male patients. The primary reason for seeking medical attention is the sexual organ maturation that patients with MAS usually experience during childhood. 9
The diagnosis of MAS is based on clinical findings, requiring at least 2 key features such as FD, CAL, or PP. Additional manifestations may include ovarian or testicular lesions, thyroid dysfunction, excessive GH production, and neonatal hypercortisolism. While genetic testing for GNAS mutations can provide confirmation, its reliability varies due to mosaicism. Since a negative genetic result does not exclude MAS, diagnosis is primarily guided by clinical presentation. 3
MAS management is symptomatic, requiring a multidisciplinary team. 1 PP is treated with aromatase inhibitors, estrogen receptor modulators, and anti-androgens in girls, while boys may receive androgen receptor blockers and steroidogenesis inhibitors. Hyperthyroidism is initially managed with thionamides, though thyroidectomy is often preferred for long-term control. GH excess responds to somatostatin analogs or GH receptor antagonists. Neonatal hypercortisolism is treated with metyrapone, with ketoconazole or mitotane as alternatives before considering adrenalectomy. 3 FD management focuses on pain relief with analgesics and bisphosphonates, administered at the lowest effective dose. 10 A recent study suggests that denosumab may be beneficial in patients unresponsive to bisphosphonates. 1 In reported cases, denosumab (commonly administered at 60 mg subcutaneously every 3-6 months) has been associated with decreased bone turnover markers, improvement in pain, and radiological signs of lesion stabilization or regression. However, these findings are based on small, non-randomized studies. Given the risk of rebound hypercalcemia and bone turnover acceleration upon discontinuation, denosumab use should be carefully monitored, with a clear plan for cessation and possible transition back to bisphosphonates. Emerging therapies such as denosumab and burosumab show promise, but further studies are needed. 1 Due to the mosaic nature of MAS, no definitive targeted treatment currently exists.
Conclusion
This case highlights the importance of recognizing MAS in young children with FD, CAL, and PP. Diagnosis was based on clinical features, with long-term multidisciplinary management essential for monitoring endocrine and skeletal complications. While treatment remains symptomatic, ongoing research into targeted therapies may improve outcomes. Early recognition and intervention are crucial for optimizing patient care and quality of life.
Footnotes
Acknowledgements
The authors express their gratitude to the patient and their family for their great contribution. Also, the authors express profound gratitude to the Polytechnic Medical Students’ Research Association (PMRA) for their invaluable contributions and unwavering support that significantly enriched every stage of the research journey.
Ethics Approval
Our institution does not require ethics approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient’s family for publication of this case report and any accompanying images. A copy of the written consent form is available for review by the editor of this journal if requested.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used to support the findings of this study are included in the article.