
Abstract
A 71-year-old Japanese woman presented to our hospital to consult for a gallbladder polyp detected on a routine ultrasound in 2024. We found a sized-up gallbladder polyp and a liver tumor. She underwent laparoscopic segment 8 subsegmentectomy and cholecystectomy for suspected malignancy. Pathology revealed aggressive follicular lymphoma of the liver and gallbladder. Immunohistochemical staining was positive for CD10, CD20, CD23, CD79a, BCL-2, and BCL-6, and negative for CD3, CD5, and cyclin-D1. Primary hepatic lymphoma and gallbladder polyp are accidental, and diagnosis is difficult without tissue biopsy or specimens. Laparoscopic hepatectomy facilitates accurate diagnosis and early postoperative recovery, enabling rapid chemotherapy administration.
Introduction
Primary hepatic lymphoma (PHL) is a primary liver tumor and an extremely rare malignancy with a difficult diagnosis.1-3 Differentiating between PHL and secondary hepatic lymphoma without invasive procedures is challenging. 4 PHL is a lymphoma localized in the liver and perihepatic lymph nodes, without distant lymph node enlargement, splenomegaly, splenic lesions, bone marrow, or blood diseases for at least 6 months after a liver tumor onset.3,5 Here, we report a case of PHL and follicular lymphoma (FL) diagnosed postoperatively and comprehensively describe its characteristics.
Case Report
A 71-year-old Japanese woman presented to our hospital with ultrasonographic findings of a gallbladder polyp. Routine ultrasonography revealed a gallbladder polyp and liver tumor. The patient’s medical and family history was unremarkable, without a history of malignancy. She reported no subjective symptoms.
Laboratory findings on admission, including blood tumor markers, were within normal limits (Figure 1). Abdominal contrast-enhanced computed tomography (CT) revealed a hypoenhancing hypodense lesion in segment 8 (S8) of the liver. The liver lesions measured 20 mm in diameter (Figure 2), while the gallbladder polyp was ~10 mm in diameter and was gradually progressive. Abdominal magnetic resonance imaging revealed a liver tumor measuring 18 mm in S8. The lesions showed a low signal on T1 images (Figure 3) and uneven internal enhancement post-contrast administration, with unclear edges. Fluorodeoxyglucose (FDG) positron emission tomography (PET) confirmed abnormal metabolic activity with no standardized uptake in the S8 lesion or intense metabolic activity (Figure 4). Heterogeneous diffuse FDG uptake in the liver did not appear, while normal homogenous FDG uptake was observed.

Laboratory findings.

Preoperative abdominal computed tomography. Contrast computed tomography indicated a hypoenhancing hypodense lesion in segment VIII of the liver (yellow arrow).

Preoperative abdominal MRI. MRI revealed a liver tumor that showed a low signal on T1 images and uneven internal enhancement after contrast administration with unclear edges. MRI, magnetic resonance imaging.

Preoperative fluorodeoxyglucose PET-CT. Fluorodeoxyglucose PET confirmed abnormal metabolic activity with no standardized uptake in the segment VIII (S8) lesion (white arrow). PET-CT, positron emission tomography-computed tomography.
The patient was diagnosed with a gallbladder polyp and was scheduled for hepatic resection of S8 and cholecystectomy. She underwent laparoscopic S8 subsegmentectomy of the liver and cholecystectomy for a suspected malignancy. The total operative time and intraoperative blood loss were 313 min and 150 mL, respectively. Specifically, the resected specimen was 1.8 × 1.6 cm and we suspected it to be mixed-type hepatocellular carcinoma (HCC; Figure 5). The patient had an unremarkable postoperative course and was discharged on postoperative day 13. Pathological examination revealed aggressive FL of the liver (Figure 6a) and gallbladder (Figure 6b). Immunohistochemical staining was positive for CD10, CD20, CD23, CD79a, BCL-2, and BCL-6 (Figure 7a and b), and negative for CD3, CD5, and cyclin-D1. The patient refused a bone marrow biopsy after the final diagnosis. After 18 months of follow-up, she showed no signs or symptoms of recurrence without chemotherapy.
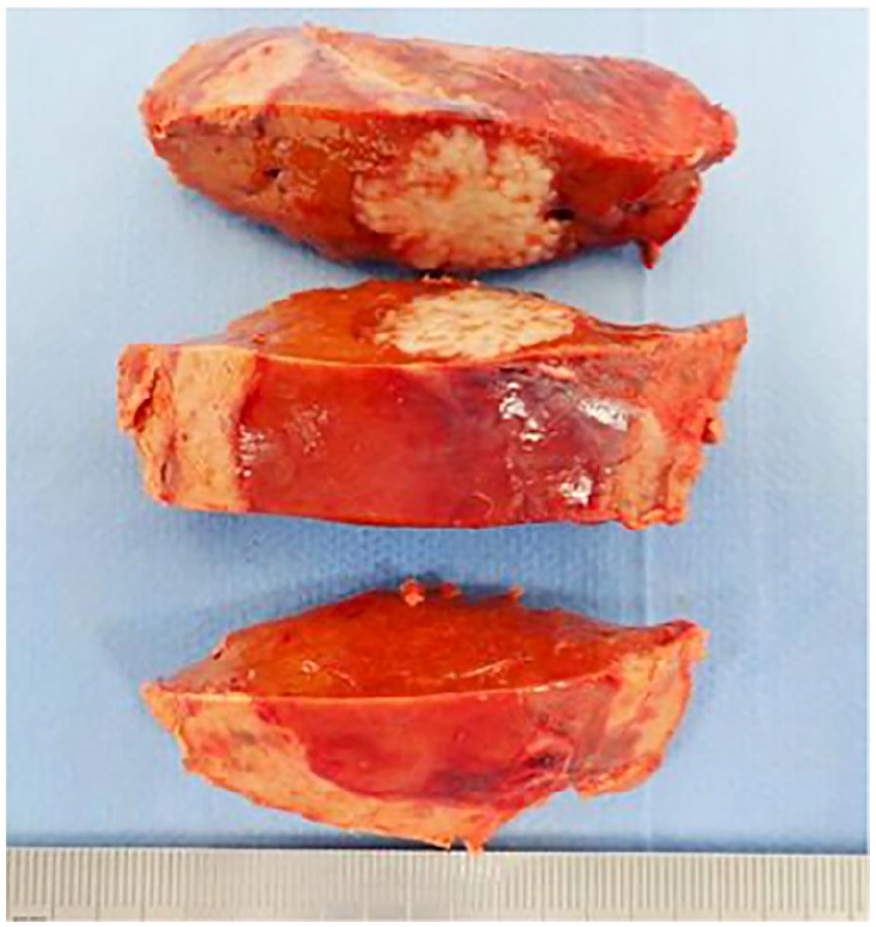
Resected specimen. The resected specimen was 1.8 × 1.6 cm and we suspected it to be a mixed-type hepatocellular carcinoma.

Histological appearance (hematoxylin and eosin staining ×40). Pathological examination revealed aggressive FL of the liver (a) and gallbladder (b), which showed a tumor-like structure mimicking the normal germinal center of a lymphoid follicle. FL, follicular lymphoma.

Immunohistochemical findings (both staining ×40). Immunohistochemical staining was positive for CD10, CD20, CD23, CD79a, BCL-2, and BCL-6, and negative for CD3, CD5, and cyclin-D1. BCL-2 and CD10 were positive for B-cell lymphoma.
Discussion
PHL is an extremely rare malignancy that constitutes ~0.016% of all non-Hodgkin lymphomas. 6 It remains localized in the liver at an early stage without infiltrating other sites, accounting for 0.4% of extranodal non-Hodgkin lymphomas. 7 The histological type is diffuse large B-cell lymphoma, 1 followed by FL, predominantly affecting individuals aged 50 to 62 years, with a male-to-female ratio of 2.3:1. 8 PHL can be subcategorized into nodular (39%-42%), multinodular (50%-55%), and diffuse (6%-8%) types.3,9 Its pathogenesis is believed to be primarily related to infectious factors, particularly hepatitis C virus (HCV) infection. 9 Some studies have reported an association between PHL and hereditary melanosis. 10 Our case involved a 71-year-old HCV-negative female patient diagnosed with FL, making her older than patients reported in any previous cases. In addition, the lymphoma was of the nodular subtype. 8
Yamazaki et al 11 showed that the diagnosis of PHL was difficult without tissue biopsy, and its criteria included (1) nodules or diffuse lesions of malignant lymphoma (ML) in the liver, (2) pathological evidence of ML in the lesions, and (3) no ML lesions in other organs such as the systemic lymph nodes or spleen. 11
Our case fulfilled all the criteria of PHL (1-3); PET-CT scan findings were negative.
Our patient underwent laparoscopic S8 subsegmentectomy of the liver.
Laparoscopic hepatectomy allows accurate diagnosis and early postoperative recovery, enabling rapid chemotherapy administration for malignant tumors. After laparoscopic surgery, PHL was eventually diagnosed through pathological examination, which showed positive immunohistochemical staining for CD10, CD20, CD23, CD79a, BCL-2, and BCL-6. Incidentally, this patient was diagnosed with FL of the gallbladder.
We could easily diagnose the FL of the gallbladder at first glance (Figure 6b), which was a coincidence. Our case is extremely rare, as both PHL and FL of the gallbladder were diagnosed simultaneously. FL is the second most common type of non-Hodgkin lymphoma, accounting for ~35% and 70% of all non-Hodgkin and indolent lymphomas, respectively. It represents the malignant counterpart of normal germinal center B-cells. Approximately 85% of patients with FL have t(14;18) translocations, which results in BCL-2 protein overexpression.12,13
Most patients with PHL have high lactate dehydrogenase and beta-2 microglobulin levels and abnormal liver enzymes, including aspartate transaminase and alanine aminotransferase, although these levels may be normal (Figure 1) in this patient.
Radiographic imaging characteristics of PHL, 14 include a low apparent diffusion coefficient value, bilateral/vascular floating sign, multinodular sign in the arterial phase, and double-ring sign in the delayed phase of dynamic enhancement. In non-Hodgkin lymphoma, 57% of cases show hepatic infiltration on autopsy. FDG PET-CT findings, which are a useful imaging technique, showed hepatic accumulation in 15% of cases.15-17 Therefore, as in this case, PET-CT confirmed abnormal metabolic activity with no standardized uptake or false-positive findings at the liver lesion.
However, distinguishing PHL from mixed-type HCC preoperatively is difficult. Laboratory findings, particularly tumor markers, including carcinoembryonic antigen, alpha-fetoprotein, and protein induced by vitamin K absence or antagonist-II, were within normal limits. We preoperatively diagnosed HCC, mixed-type or intrahepatic cholangiocarcinoma.
Regarding the prognosis of PHL 13 , a recent analysis of United States and French cohorts reported improved overall survival (OS) in the rituximab era, with a 10-year OS of ~80%. However, lymphoma, particularly histologic transformation, remained the primary cause of death, with disease-specific mortality of 10% at 10 years. 18
In conclusion, PHL is extremely rare, especially in the liver and gallbladder, and its diagnosis is difficult without tissue biopsy or specimens. However, laparoscopic hepatectomy allows for an accurate diagnosis and early postoperative recovery, enabling rapid administration of chemotherapy.
Footnotes
Acknowledgements
The authors would like to thank Dr Emoto from the Department of Hematology at Shiroyama Hospital for his valuable guidance and insightful comments throughout the course of this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to publish this case report was obtained from the ethics committee of Shiroyama Hospital (approval number: SH 2018-004).
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.