
Abstract
Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) is a rare intracranial tumor that arises from pericytes surrounding the blood vessels. Solitary fibrous tumor/hemangiopericytoma accounts for less than 1% of primary brain tumors and is classified as grades I, II, or III based on mitotic count. These tumors often masquerade as meningiomas. Histologically, SFT/HPC is vascular with high cellularity and often surrounded by connective tissue. Immunohistochemistry is positive for stat 6, vimentin, and CD34. Although aggressive surgical resection is the mainstay of treatment, close long-term follow-up is necessary as recurrence or extra cranial metastasis can present several years after resection.
Keywords
Introduction
Solitary fibrous tumor/hemangiopericytoma (SFT/HPC) accounts for less than 1% of primary brain tumors. SFT and HPC were classified as the same central nervous system (CNS) tumor by the World Health Organization (WHO) since 2016 due to the overlap in STAT6 expression. 1 It is easily mistaken and occasionally misdiagnosed as meningioma which proves to be a critical error considering SFT/HPC is a more aggressive tumor, metastasizing in 20% of cases and recurring in 60%. 2 Aggressive surgical resection is the mainstay of treatment; however, because recurrence or extra cranial metastasis can present several years after resection, close long-term follow-up is needed with regular clinical and imaging studies.2,3 In this case report, we present a patient with an intracranial SFT/HPC with subtotal resection who succumbed to the illness 8 years later due to unresectable liver metastasis after failing to follow-up.
Case Presentation
A 59-year-old male presented to the emergency department with progressively worsening headache for several months and new onset right hemiparesis. Computed tomography scan of the head without contrast revealed a dense left frontal mass with vasogenic edema. Magnetic resonance imaging of brain was obtained which demonstrated a large, 6 cm x 6 cm, necrotic left frontal mass with associated midline shift but without significant peritumoral edema (Figure 1). He underwent subtotal resection of the intracranial mass. Histology was positive for cellular neoplasm with many thin- and thick-walled blood vessels. The neoplastic cells were randomly oriented with slit-like branching and irregular vascular spaces. Multifocal areas of necrosis, hypercellularity, and moderate nuclear atypia were consistent with anaplastic hemangiopericytoma (WHO grade 3). The patient received adjuvant radiation and was subsequently lost to follow-up. Eight years later, he was evaluated in the emergency department for right upper quadrant pain after sustaining a fall. Ultrasound showed a sub-capsular solid density in the ventral aspect of the right lobe of the liver. Computed tomography scan of the liver with contrast demonstrated multiple round masses in various stages of enhancement. The largest of these lesions was noted in the anterior segment and inferior margin of the right lobe showing rim enhancement while the other lesions were completely opacified (Figure 2). At that time, magnetic resonance imaging of brain showed no evidence of intracranial recurrence (Figure 3). Computed tomography guided liver biopsy demonstrated ovoid spindle cell proliferation with indistinct cell borders arranged haphazardly and dilated, branching, staghorn blood vessels (Figure 4). Immunohistochemistry was positive for STAT6 (Figure 5), CD34, vimentin, CD99, and BCL-2. Histology was similar to that of his resected intracranial tumor 8 years prior, thus the diagnosis of metastatic SFT/HPC. Liver disease was deemed unresectable therefore the patient was started on palliative chemotherapy with oral temazolamide and intravenous bevacizumab. Unfortunately, within 2 months of starting chemotherapy, the patient’s performance status declined and he was referred to hospice. Within 6 months after diagnosis of recurrent SFT/HPC, the patient succumbed to his illness.

Magnetic resonance imaging of brain at initial presentation.
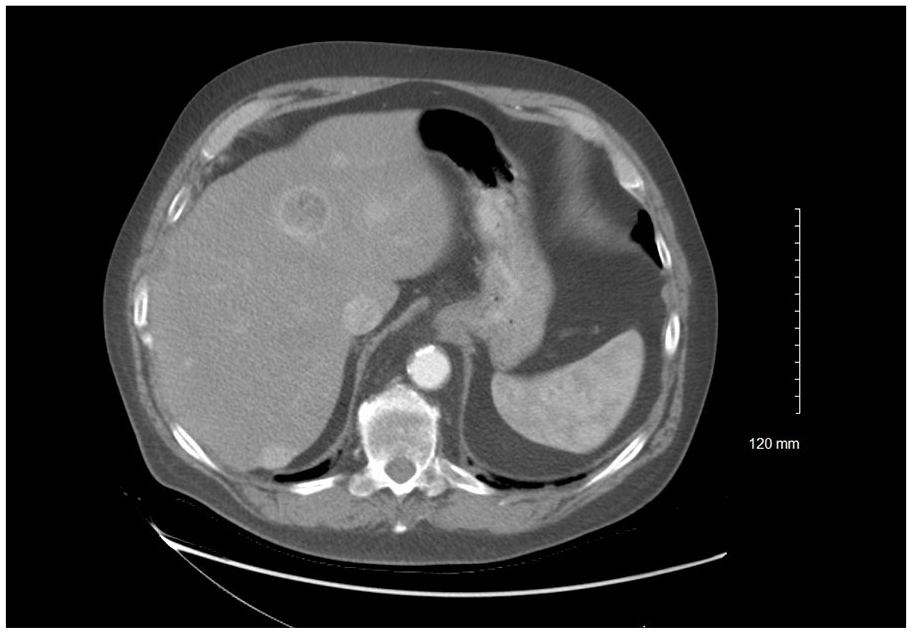
Computed tomography of the liver showing multiple liver lesions.

Magnetic resonance imaging of brain at recurrence post surgery.
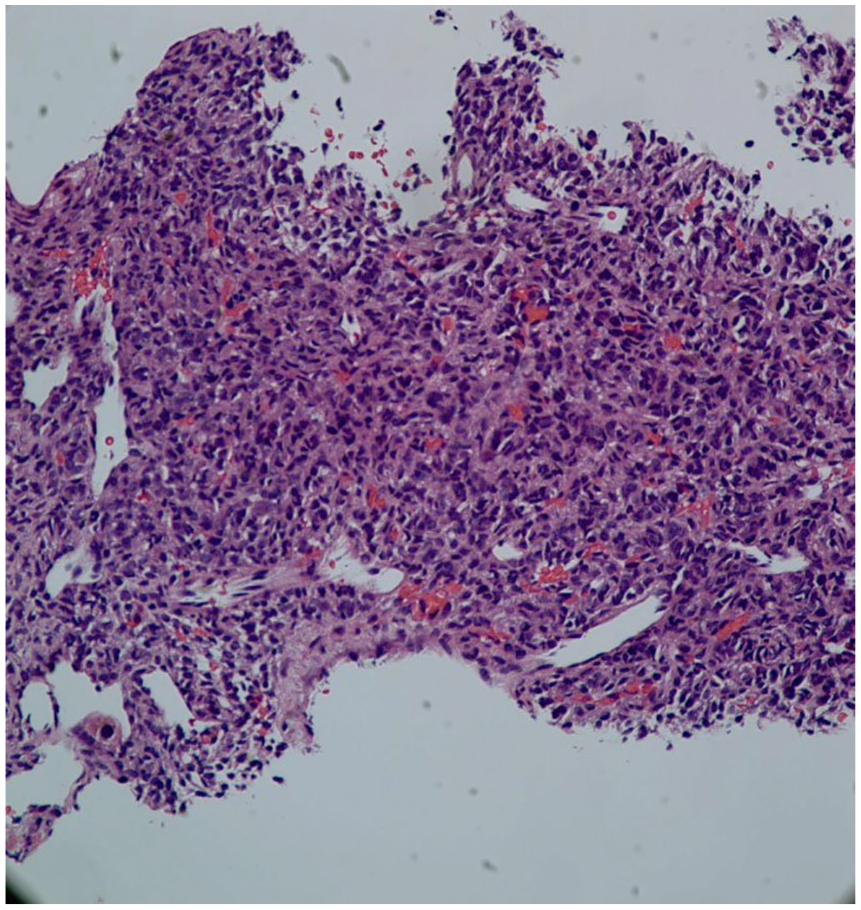
Hematoxylin and eossin tain of liver biopsy.

Strong STAT 6 positivity on liver.
Discussion
Solitary fibrous tumor/hemangiopericytoma can occur in patients of any age but is most common in males ranging from 20 to 39 years of age.4,5 Patients with SFT/HPC typically present with neurological signs and symptoms secondary to mass effect of the tumor.2,4 Magnetic resonance imaging, the preferred modality for visualizing SFT/HPC, may exhibit similar radiographic features [such as “dural tail” sign] as those of high-grade meningiomas. Because of the similarities on imaging, histology, and tumor marker expression obtained after surgical resection of the mass are used to differentiate between the tumors. 2 In particular, STAT6 and CD34 have a high sensitivity and specificity for SFT/HPC. In a study performed by Macagno et al, 6 STAT6 was positive in 96% of SFT/HPCs as opposed to 0% in meningiomas. In Bouvier et al’s 7 study, CD34 was positive in 83% of SFT/HPC cases as opposed to 4.9% in meningioma. Due to the combination of solitary fibrous tumor and hemangiopericytoma as a single diagnosis, 3 grades of tumor were created: grade 1 marked by low cellularity, grade 2 marked by high cellularity, and grade 3 marked by at least 5 mitoses per high-power field.1,8 After diagnosis is confirmed, gross total removal of the tumor is the gold standard treatment. Although radiation therapy has been shown to increase the recurrence-free interval and provide local control of the primary tumor, studies indicate that radiation has no effect on survival and is thus used as a means to improve quality of life rather than longevity.3,9 Multiple chemotherapeutic agents have been tried; however, none are approved presently due to lack of effectiveness. One common chemotherapeutic regimen used includes traditional cytotoxic agents such as doxorubicine, ifosfamide, and taxane but has limited effectiveness. Another regimen, temozolomide plus bevaizumab is more effective in maintaining stable disease with lesser side effect profile. 10 The other options are tyrosine kinase inhibitors like sunitinib and sorafenib. 10 Close long-term follow-up has the potential for improving mortality due to the tumor’s aggressive and invasive nature leading to recurrence and distant metastasis. 8 Immunostaining of Fascin-1, a protein involved in cell migration and invasion, has also shown great potential in predicting patient prognosis. In a study performed by Yamamoto et al, 11 Fascin-1 has a strong association with tumor recurrence (P < .05). Metastasis of SFT/HPC can occur several years after the initial diagnosis, even after total gross resection of the tumor, with a mean time of 7.5 years.4,5,12 After 10 years, given appropriate patient follow-up, there is up to a 70% chance of recurrence or metastasis with the most common sites being bone, liver, or lung.2,13 Although prognosis is generally poor with recurrence or metastasis, there are several factors affecting the surgical treatment’s effectiveness. The most important factor is tumor size and thus how soon the diagnosis is made. 3
Conclusion
Solitary fibrous tumor/hemangiopericytoma does not cause specific symptoms but can cause symptoms secondary to mass effect as are seen in other brain tumors. Solitary fibrous tumor/hemangiopericytoma most commonly occurs in the third decade of life with a slightly higher rate in males. Metastasis or local recurrence can be delayed up to 2 decades from initial diagnosis thus long-term follow-up is warranted. Common sites for extracranial metastasis include lung, liver, and bones. Although there is no approved chemotherapy regimen, because these are highly vascularized tumors with high expression of angiogenic markers multiple retrospective single institutional studies have explored the use of antiangiogenic drugs such as pazopanib and combination temozolomide-bevacizumab. 12 In advanced disease, these drugs have shown promising results and may soon be considered first line treatment. Referral to high-volume center with availability of clinical trial is encouraged.
Footnotes
Author’s Note
The case was presented at American College of Physicians Kentucky Chapter conference on September 12, 2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient is expired and no immediate family members are available. Authors have carefully excluded patient identifiers per HIPAA guidelines.