
Abstract
Primary breast lymphoma (PBL) is a rare type of non-Hodgkin’s lymphoma, comprising less than 1% of all lymphomas and 0.5% of breast malignancies. The majority of PBL cases are of B-cell origin, with diffuse large B-cell lymphoma (DLBCL) being the most common subtype, though follicular lymphoma (FL) also occurs. We present a case of a 74-year-old woman whose routine mammogram revealed a 1.5 cm mass in the right breast. Ultrasound and biopsy confirmed the presence of classic follicular lymphoma, with B-cell markers CD20, CD10, Bcl-6, and Bcl-2. A PET scan and biopsy of the left periaortic lymph node identified additional disease, confirming stage III FL. The patient was asymptomatic and exhibited favorable prognostic factors, including normal beta-2 microglobulin and LDH levels. Due to the indolent nature of her disease and low tumor burden, the decision was made to pursue active surveillance rather than immediate treatment. This case highlights the diagnostic challenges of PBL and the importance of personalized management, particularly in asymptomatic patients with low disease burden.
Keywords
Introduction
Primary breast lymphoma (PBL) is an uncommon malignancy, representing less than 1% of non-Hodgkin’s lymphomas (NHL) and only 0.5% of malignant breast tumors. 1 It was first described by Dobrotina in 1959 2 and is defined by criteria established by Wiseman and Liao. 3 These criteria include the presence of lymphomatous infiltrates in close association with breast tissue, absence of previously known or disseminated lymphoma, yet allowance of simultaneous ipsilateral axillary lymph node involvement. 3 PBL is distinct from secondary breast lymphomas, which involve the breast as part of systemic disease.
PBL typically presents as a painless breast mass and often mimics breast carcinoma both clinically and radiologically, making biopsy essential for diagnosis. 4 Over 90% of PBL cases are of B-cell origin, with diffuse large B-cell lymphoma (DLBCL) being the most prevalent subtype, accounting for 40% to 70% of cases. Less common subtypes include marginal zone lymphoma, mucosa-associated lymphoid tissue (MALT) lymphoma, anaplastic large cell lymphoma (ALCL), particularly breast implant-associated ALCL (BIA-ALCL), and follicular lymphoma (FL).5-9 FL is believed to originate from follicular lymphocytes and is characterized by the presence of both centrocytes and centroblasts, which help classify it into Grades 1 to 3. 10 Primary FL of the breast has been documented in several cases, some of which have shown an association with ductal carcinoma in situ (DCIS) and invasive breast carcinoma.11,12
Here, we present a case report of a patient with classic follicular lymphoma of the breast, highlighting the clinical presentation, diagnostic challenges, and treatment approach to contribute to the growing understanding of this rare entity.
Case Presentation
A 74-year-old female presented for a routine screening mammogram, which showed a new mass lesion measuring 1.5cm in the mid-inner right breast. Ultrasound of the right breast demonstrated an oval, mildly lobulated hypoechoic mass at the 2:00 position 5 cm from the nipple measuring 1.1 × 0.9 × 0.6 cm (BI-RADS 4-suspicious) (Figure 1). Mammogram-assisted fine needle biopsy of the right breast mass was performed, and the tumor revealed a lymphoid infiltrate consisting almost entirely of abnormal B cells. Immunostaining revealed CD20 positivity, co-expressing CD10, BCL-6 and BCL-2. CD-5 and Cyclin D1 were negative. Ki-67 was approximately 40%. Pathology of the breast mass confirmed classic follicular lymphoma (Figure 2).

Right breast ultrasound of a rounded mass at the 2 o’clock position, 5 cm from the nipple.
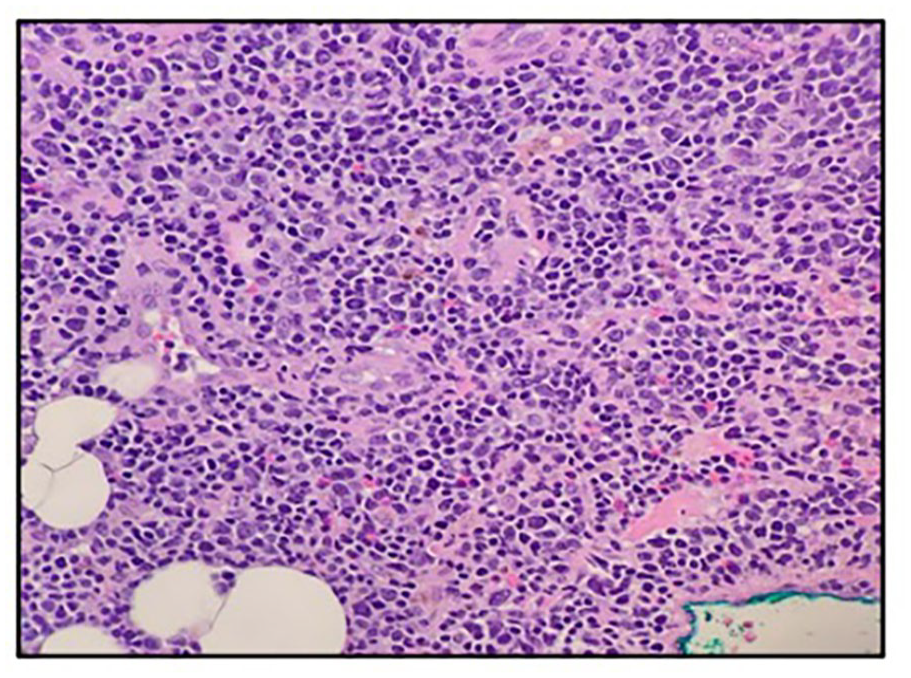
H&E sections showing multiple fragments of lymphoid infiltrate sheets in a benign breast parenchyma background. Diffuse lymphoid infiltrate is noted with small-to-medium lymphocytes with round/oval to curved nuclei, 1-3 nucleoli, clumped chromatin, and scant cytoplasm. The lymphoid infiltrate is almost entirely abnormal B cells expressing CD20, CD10, BCL6, and BCL2. CD5 and Cyclin D1 were negative. Ki 67 40%.
For staging workup, a positron emission tomography (PET) scan was performed and confirmed hypermetabolic activity within the medial right breast at the site of the biopsy, with additional hypermetabolic activity in the left periaortic lymph node, left axillary nodes, right gluteal region, and right thyroid lobe. Thereafter, the patient was seen by Medical Oncology for further evaluation of classic follicular lymphoma of the breast, and it was recommended that the patient undergo biopsy of the left periaortic lymph node to confirm the diagnosis. Initial lab work at the Medical Oncology visit showed white blood cell (WBC) count 6.74 k/cmm, platelet count 205 k/cmm, hemoglobin 13.0 gm/dL, and lymphocytes 21.2%. CT-guided biopsy of the left periaortic lymph node revealed lymphocytes with round to curved nuclei, clumped chromatin, and scant cytoplasm. A vague nodule/germinal center was present. Immunostaining showed that most of the lymphocytes were B cells, highlighted with CD20, expressing BCL6, a vague germinal center, positive for BCL2, and CD10. CD21 highlighted the follicular dendritic meshwork in the nodules. B cells were negative for CD5, Cyclin D1, and MUM1-1. Ki-67 low: 20% to 30%. The pathologic findings of the periaortic lymph node were similar in morphology and immunophenotype to those of the patient’s initial diagnostic biopsy from the right breast mass shown in Figure-2. Flow cytometry of the periaortic lymph node showed 50% B cells: monotypic with an abnormal immunophenotype, expressing CD19, CD20, CD10, FMC7, and kappa light chain restriction. They were negative for CD5, CD23, CD34, and lambda light chain. Flow cytometry further confirmed the diagnosis of classic follicular lymphoma. Based on the distribution of the lymphoma both above and below the diaphragm, the patient was diagnosed with Stage III classic follicular lymphoma. According to the Groupe d’Etude des Lymphomes Folliculaires (GELF) criteria, the decision was made to hold off on systemic treatment and instead, pursue surveillance with repeat follow-up in 3 months.
Discussion
In this case, we present a primary breast lymphoma of the right breast that was incidentally detected with routine mammographic screening. Once the mass was detected, the first impression was suspected breast malignancy. However, the initial mass contained features that are unusual in breast malignancy, such as nonspiculated margins (had a rounded appearance) and lack of micro-calcifications. Regardless, the primary lesion was promptly biopsied and sent for pathology, which confirmed follicular lymphoma with B-cell markers CD20, CD10, and lymphoma markers Bcl-2 and Bcl-6. Additional biopsy of the left para-aortic lymph nodes also demonstrated histological and molecular findings similar to the primary lesion. Since the patient had lesions both above and below the diaphragm, the follicular lymphoma was classified as stage III. This patient did not exhibit symptoms and had several favorable prognostic indicators, as per the Follicular Lymphoma International Prognosis Index (FLIP-2). Her beta 2 microglobulin was normal, LDH was normal, the tumor was less than 6 cm, and she did not have cytopenia on her blood work. Therefore, proceeding with the “watchful waiting approach” with close follow-up was the most appropriate course for this patient. 13 Although the patient in this case did not require treatment, it stimulates an interesting discussion regarding the development of new approaches for those with primary breast lymphoma.
A review of nine articles highlighted the clinical heterogeneity of primary breast lymphoma cases. Patient ages ranged from 46 to 80 years, with a predominance of female patients (Table 1). The initial presentations varied widely, from incidental, asymptomatic findings to more overt manifestations such as palpable breast masses or systemic symptoms, including shortness of breath. The histopathological diagnoses predominantly included diffuse large B-cell lymphoma (DLBCL), mucosa-associated lymphoid tissue (MALT) lymphoma, and other lymphoma subtypes, with immunohistochemical markers such as CD20, BCL6, and CD10 playing a pivotal role in confirmation.14-22 The treatment plan typically involved chemotherapy, most commonly R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), with some cases incorporating radiotherapy or surgical interventions. Clinical outcomes were generally favorable, with the majority of patients achieving remission or remaining disease-free following treatment. A small proportion of patients were reported to be undergoing ongoing treatment at the time of publication. Notably, no mortality was recorded in any of the cases reviewed, suggesting that with appropriate management, the prognosis for this rare malignancy is favorable.14-22
Summary of Case Presentations of Primary Breast Lymphoma.
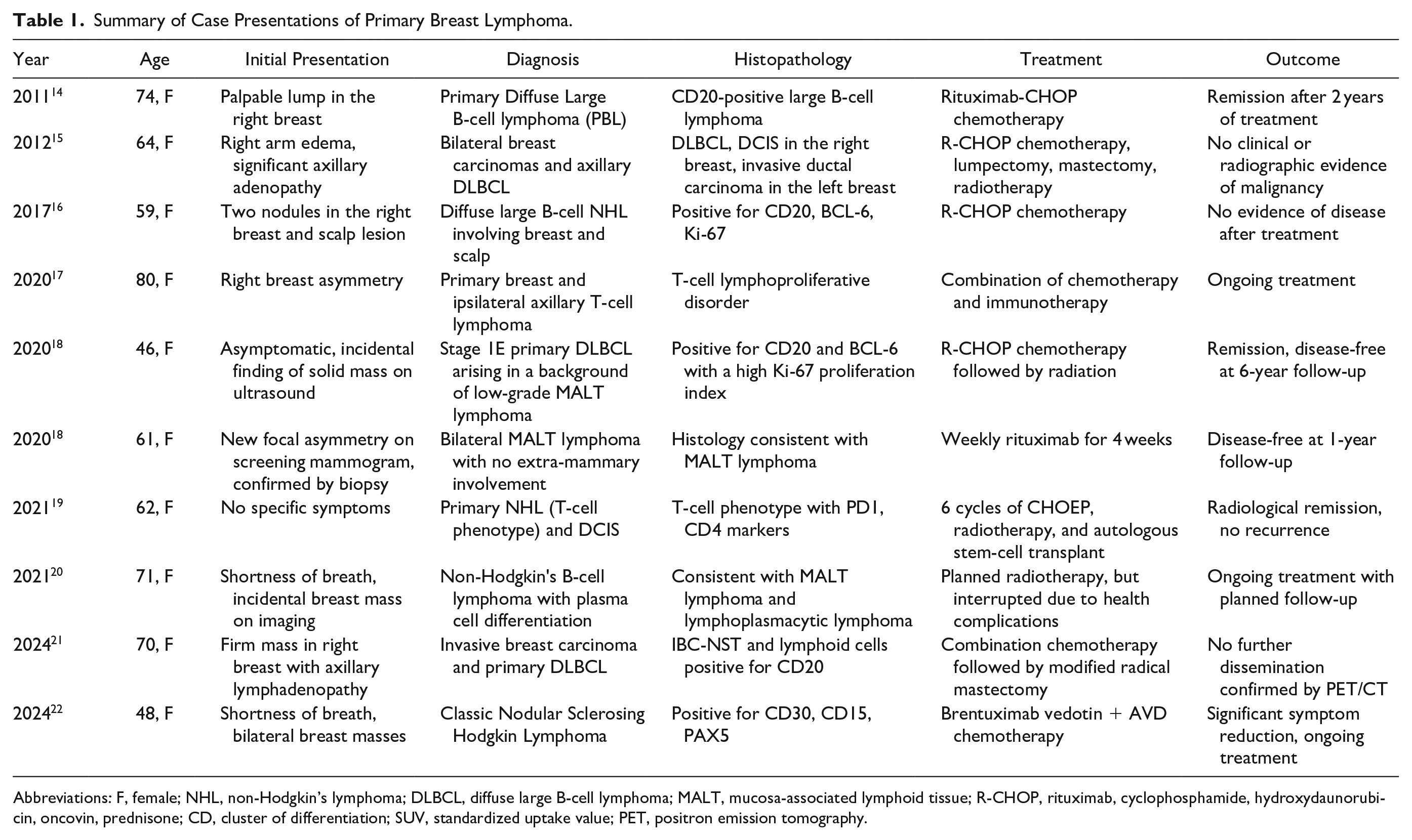
Abbreviations: F, female; NHL, non-Hodgkin’s lymphoma; DLBCL, diffuse large B-cell lymphoma; MALT, mucosa-associated lymphoid tissue; R-CHOP, rituximab, cyclophosphamide, hydroxydaunorubicin, oncovin, prednisone; CD, cluster of differentiation; SUV, standardized uptake value; PET, positron emission tomography.
There is limited evidence regarding targeted therapy for breast lymphoma. One study demonstrated higher overall survival and progression-free survival in follicular lymphoma patients that expressed high amounts ER-alpha in follicular dendritic cells. 23 Perhaps the proliferation in this subtype of follicular lymphoma patients is confined to areas of the body where mitogens such as estrogen are abundant (ie, breast) and, therefore, confers a prognostic advantage. In a way, this can be viewed as analogous to breast cancers with hormone receptor positivity, which favors a good prognosis as compared to the triple negative subtype. 24 More studies are needed to investigate the clinical significance and treatment utility of high-expressing ER-alpha follicular lymphoma. Additionally, mechanistic studies have evaluated the phosphorylated form of ER-alpha (p-Ser118), which is a prognostic marker of response to tamoxifen. 25 Additionally, a link between breast cancer and lymphoma is possible through the viral oncogenesis via the Mouse Mammary Tumor Virus, which has demonstrated both diseases in both mice and humans.26-27
Conclusion
We described a patient with an exceedingly rare PBL, classic follicular lymphoma, emphasizing the role of thorough histopathologic evaluation and imaging in establishing the diagnosis. The indolent nature of this lymphoma highlights the importance of personalized management, with surveillance being a viable approach in asymptomatic, low-burden cases. Continued reporting and study of PBL are crucial for enhancing the understanding of this rare malignancy.
Footnotes
Acknowledgements
Special thanks to the Department of Pathology for providing images in support of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case reports.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Prior Presentation of Abstract Statement
This work has not previously been presented at any conference of submitted to another journal for consideration