
Abstract
Follicular lymphoma (FL) usually has an indolent course and presents with painless, waxing and waning lymphadenopathy in the absence of systemic symptoms. It is uncommon for FL to present outside of lymph nodes, although it can develop in the gastrointestinal tract, skin, thyroid, and testes. Central nervous system (CNS) involvement in FL is rare. Most CNS lymphomas are diffuse large B-cell lymphoma, although Burkitt lymphoma, lymphoblastic lymphoma, and peripheral T-cell lymphoma are also observed. These tumors usually involve white matter but may also involve gray matter. Lymphomas of the dura are very uncommon and are usually mucosa-associated lymphoid tissue lymphomas. Here, we present a case of FL of the dura arising in a 62-year-old woman that was responsive to chemotherapy. According to a literature review, there have been 15 previously reported cases of FL of the dura. Dural FL has been most frequently treated with radiation and chemotherapy. Patients were still alive in all cases in which follow-up was reported. Although the sample size is small, these data suggest that dural FL, like other forms of FL, is an indolent disease that is associated with prolonged survival despite usually being incurable.
Case Presentation
A 62-year-old woman with a past medical history of coronary artery disease presented to her primary care physician with a 3-month history of worsening scalp pain and an enlarging, mildly tender palpable bump in the parietal area. She reported vision changes described as a darkening of her visual fields and severe, pressure-like headaches that occurred 3 to 4 times a week. She also reported worsening fatigue but denied fevers, chills, or night sweats. Magnetic resonance imaging demonstrated a 2.3 × 1.0 × 2.7 cm dural-based mass in the left frontoparietal region with extension into the gyri of the adjacent brain parenchyma (Figure 1). Notably, there were no abnormalities of the adjacent bone.
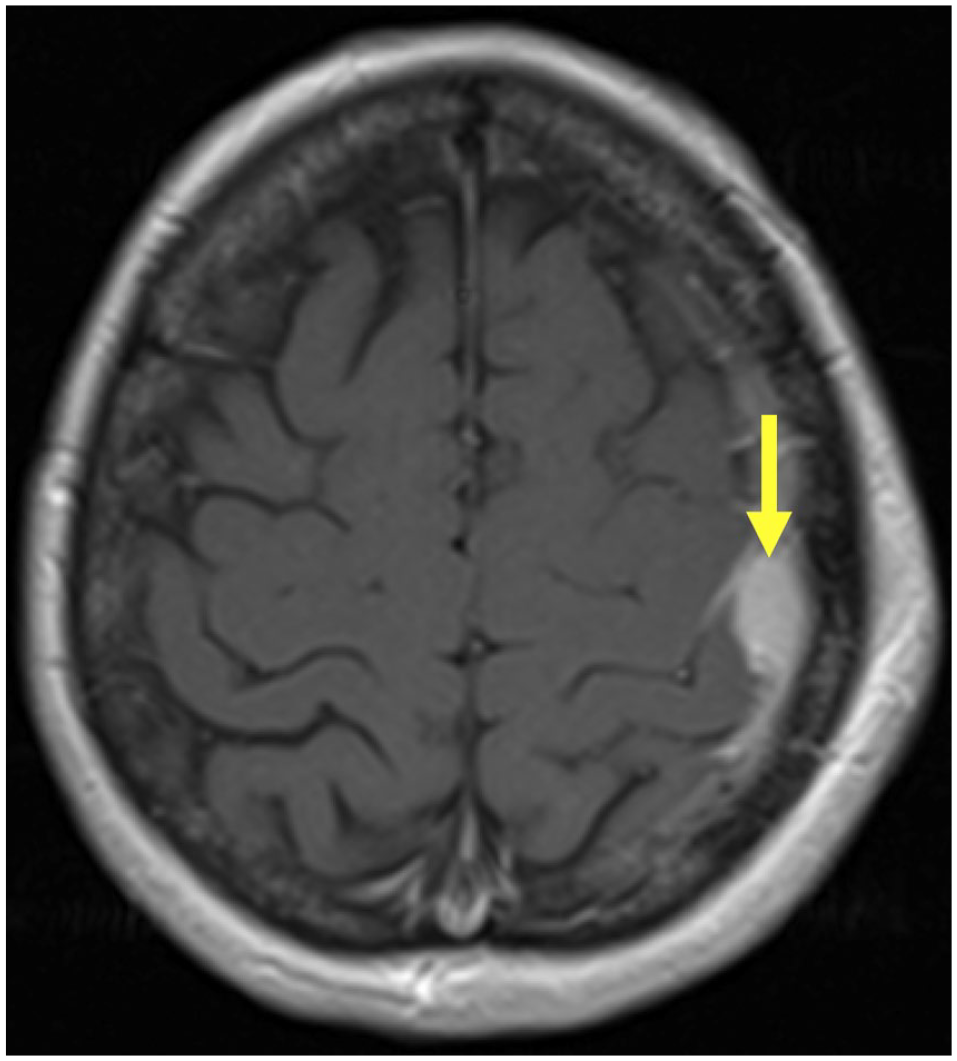
Coronal (left) and axial (right) magnetic resonance images demonstrating a 2.3 × 1.0 × 2.7 cm dural-based mass (yellow arrows) in the left frontoparietal region with associated thickening and enhancement of the adjacent dura. There is an extracranial component to the mass in the adjacent soft tissues without visible abnormalities of the bone. In addition, there are linear extension into the gyri of the adjacent brain parenchyma with an associated focal area of subcortical edema in the lateral aspect of the postcentral gyrus.
A left craniotomy was performed and biopsies were taken of the mass. Flow cytometry analysis detected a population of abnormal CD19(+)/CD20(+) B cells with dim, lambda light chain restriction and homogenous expression of CD10. Microscopic analysis demonstrated a nodular lymphocytic infiltrate consisting of centrocytes with many centroblasts (greater than 15 per high power field), diagnostic of follicular lymphoma (FL), grade IIIA (Figure 2). Immunohistochemical stains showed predominantly CD20(+)/Pax-5(+) B cells that were reactive for both Bcl-2 and Bcl-6 (Figure 3). The Ki-67 proliferation index was as high as 70% in some nodules. Cytogenetic testing revealed an abnormal female karyotype (46,XX,add(1)(p34.1),t(2;6)(q31;q21),del(6)(q21),t(14;18)(q32.3;q21.3)[10]/46,XX[10]) with fluorescent in situ hybridization confirming the presence of IGH/BCL2 gene fusion rearrangement. Cells were negative for MYC gene locus rearrangement. Next-generation sequencing analysis was notable for loss of function mutations of the CREBBP and KMT2D genes. Computed tomography (CT) scans of the chest, abdomen, and pelvis were notable for bilateral hilar adenopathy with nodes up to 12 mm in size, suggestive of disease spread.

(A) The dura demonstrates infiltration of fibrous tissue by a vaguely nodular lymphocytic infiltrate (hematoxylin and eosin, 40× magnification). (B) Closer inspection of 1 of the nodular areas reveals the infiltrate to consist of a mixture of small lymphocytes with cleaved nuclei (centrocytes) and large lymphocytes with multiple nucleoli (centroblasts) (hematoxylin and eosin, 400× magnification).

(A) Lymphocytes express CD20, consistent with B cells (CD20 immunohistochemical stain, 200× magnification). (B) CD21 highlights retained follicular dendritic cell meshworks (CD21 immunohistochemical stain, 200× magnification). B cells show aberrant co-expression of (C) Bcl-2 and (D) Bcl-6 (Bcl-2 and Bcl-6 immunohistochemical stains, 200× magnification). The overall morphological and immunophenotypic findings support the diagnosis of follicular lymphoma.
The patient was treated for grade IV stage IIIA FL with methotrexate, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (MR-CHOP), which was generally well tolerated. The CT scan after cycle 3 showed good disease response with reduced mediastinal lymphadenopathy and no residual brain lesion. Follow-up scan after cycle 6 showed slightly reduced hilar lymphadenopathy.
Discussion
Follicular lymphoma is the second most common type of non-Hodgkin lymphoma after diffuse large B-cell lymphoma (DLBCL). 1 There are about 15 000 cases of FL in the United States and Europe per year. 2 Median age of diagnosis is 65 years. 3 Pathogenesis normally involves overexpression a translocation between chromosomes 14 and 18. This translocation leads to overexpression of the leukemia/lymphoma 2 (BCL2) oncogene. 4
FL usually presents with painless, waxing and waning lymphadenopathy in the absence of systemic symptoms despite widespread disease; basic labs are often normal, and just a fifth of patients report weight loss or B symptoms. 5 It is uncommon for FL to present outside of the lymph nodes. 6 The most common sites of primary extranodal FL are the gastrointestinal tract (often the second portion of the duodenum), skin, thyroid, and testes. Central system involvement (CNS) involvement in FL is rare. 7 Meanwhile, the vast majority of CNS lymphomas are DLBCL, although Burkitt lymphoma, lymphoblastic lymphoma, and peripheral T-cell lymphoma not otherwise specified are also observed. 8 These tumors usually involve white matter but may also involve gray matter. 9 Lymphomas of the dura are very rare and are usually mucosa-associated lymphoid tissue (MALT) lymphomas. 10
Dura mater is a dense layer of irregular connective tissue that serves as the outermost layer of the meninges, sitting atop arachnoid and pia mater. Meningiomas are by far the most common dural tumor. Other dural tumors include solitary fibrous tumors, sarcomas, and metastases, as well as less common tumors such as Ewing sarcoma, gliosarcomas, and xanthoastrocytomas. 11 There have been at least 105 cases of dural MALT lymphoma described in the literature. 12 The FL of the dura is less common still; in our literature review, we identified 15 such cases with convincing pathological date consistent with a diagnosis of dural FL (Table 1).
Case Reports of Follicular Lymphoma of the Dura With Associated Size, Histology, Treatment, and Outcome.

Abbreviations: FL, follicular lymphoma; CAP, cisplatin, adriamycin, prednisone; CHOP, cyclophosphamide, hydroxydaunomycin (doxorubicin), oncovin (vincristine), prednisone; NED, no evidence of disease; LAD, lymphadenitis; MR-CHOP, methotrexate, rituximab, cyclophosphamide, hydroxydaunomycin (doxorubicin), oncovin (vincristine), prednisone; IV, intravenous; R-CHVP, rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone; IT, intrathecal; R-CHOP, rituximab, cyclophosphamide, hydroxydaunomycin (doxorubicin), oncovin (vincristine), prednisone.
Conclusion
Median age of patients with dural lymphoma was 56.7, close to the median age of 65 in all patients with FL. 25 Common anatomical locations included dura overlying the frontal area (6) spinal column (4), and cavernous sinus (2). Systemic involvement was reported in 8 cases; these included lymph nodes in 7 cases, bony metastases in 2, and bone marrow in 1. Of the 14 cases (including our patient) in which the grade of the lymphoma was reported, 10 were low grade (I or II), 2 were IIIA, 1 was IIIB, and 1 was IV. Of the 14 cases (including ours) in which treatment was reported, 3 patients received radiation only, 10 received radiation and chemotherapy, and 1 patient received chemotherapy only. Eleven cases reported outcomes at least 6 months after diagnosis and, in all cases, patients were alive. Patients were still alive in all cases in which follow-up was reported. Although the sample size is small, these data suggest that dural FL, like other forms of FL, is an indolent disease that is associated with prolonged survival despite being incurable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.