
Abstract
Blastomyces dermatitidis is a dimorphic fungus that can range from mild to severe disease presentation, including the acute respiratory distress syndrome (ARDS) based on the individual’s immunity. Acute respiratory distress syndrome is an uncommon presentation having an incidence of about 10% to 15% but has a high mortality exceeding 90%. This is a case of a 50-year-old female with past medical history of asthma and type 2 diabetes mellitus who presented to the pulmonology clinic with worsening dyspnea for the last 2 months. She also had a lesion in the left lower back, which was draining purulent fluid. Chest radiographs showed bilateral infiltrates and was started empirically on vancomycin and piperacillin-tazobactam. Bronchoalveolar lavage was done and the cultures grew B dermatitidis. The patient was moved to a higher level of care and given amphotericin B. Unfortunately, the patient experienced septic shock, which later deteriorated into cardiac arrest, ultimately leading to their passing. The importance of early diagnosis of blastomycosis and timely treatment has been emphasized in this case report.
Introduction
Blastomycosis is a fungal infection caused by the fungus Blastomyces dermatitidis. It is a rare infection in the United States, but it is endemic in certain areas, such as the Ohio and Mississippi River Valleys, Great Lakes region, and the Southeastern United States. Unlike other deep fungal infections that occur primarily in immunocompromised patients, blastomycosis can occur in immunocompetent hosts as well. In many instances, patients do not exhibit symptoms, but they can also manifest acute respiratory distress syndrome (ARDS), which represents a severe manifestation of the condition, depending on the patient’s immune status. Acute respiratory distress syndrome is a life-threatening condition characterized by poor oxygenation secondary to capillary endothelial injury and diffuse alveolar damage. Acute respiratory distress syndrome carries a high mortality and few effective therapeutic modalities exist to mitigate this condition. Here, we present a case of pulmonary and cutaneous blastomycosis, which later developed into an ARDS.
Case Presentation
A 50-year-old African American female with a past medical history of asthma, hypertension, and type 2 diabetes mellitus presented to the pulmonary clinic with a 2-month history of progressive dyspnea, greenish-yellow sputum production, night sweats, and weight loss. She denied hemoptysis, fevers, or chills. She has no pertinent travel history. She also had a 1-week history of purulent discharge from a cutaneous lesion on her left lower back. Samples were taken for wound cultures on admission (Figure 1). She also had a recent emergency room visit 1 month ago for suspected community-acquired pneumonia.

Skin lesion on her left lower back (red arrow) draining purulent fluid taken on admission.
On admission, she was tachycardic with heart rate 117/min, tachypneic with respiratory rate 22/min, normotensive with blood pressure 130/83 mm Hg, and was saturating 89% on 3 L/min nasal cannula. Initial chest x-ray showed bilateral infiltrates (Figure 2). A computed tomography (CT) was done with pulmonary embolism (PE) protocol for elevated D dimer level of 15.81 mg/L-FEU, which ruled out PE but it showed presence of patchy areas of consolidation bilaterally along with mass-like lesions, most pronounced in the left lung base (Figure 3). Cultures were taken from blood, sputum, and the cutaneous lesion. She was empirically started on broad-spectrum antibiotics vancomycin and piperacillin-tazobactam. As patient has a history of weight loss and mass-like lesions are seen in the CT chest, bronchoscopy was planned. After 36 hours, bronchoscopy and bronchoalveolar lavage (BAL) was acquired and sent to the lab for cytology, Gram’s stain, bacterial culture, and fungal cultures. Her bronchoscopy was complicated with right lower lobe pulmonary hemorrhage, secondary to the biopsy done during the procedure and she could not be extubated immediately after the procedure. She was successfully extubated on day 4 but was requiring a high-flow nasal oxygen at 50% fraction of inspired oxygen and 35 L/min. Chest x-ray revealed worsening infiltrates consistent with ARDS (Figure 4). Echocardiogram showed normal left ventricular systolic function with ejection fraction of 50% to 55%, and normal right ventricular systolic function with a right ventricular systolic pressure of 17 mm Hg. Preliminary cultures from the BAL showed yeast growth at this time. Secondary to her worsening hypoxemia, she was intubated after failed noninvasive oxygen supplementation and was transferred to a higher level care facility. Autoimmune workup with antinuclear antibody (ANA) test, antineutrophil cytoplasmic antibodies (ANCA) test, anti-glomerular basement membrane, rheumatoid factor, and cyclic citrullinated peptide (CCP) antibody tests were negative. Her serum Histoplasma galactomannan antigen was positive with 8.8 ng/mL (normal: <0.5 ng/mL) and urine Histoplasma galactomannan test was also positive with >15.0 ng/mL (normal: <0.5 ng/mL). Bronchoalveolar lavage sample was positive with Grocott methenamine silver stain which showed scattered fungal spores consistent with B dermatitidis. The cutaneous wound culture also showed growth of B dermatitidis. However, almost 3- to 4-week time was taken for the cultures to result. The blood culture and sputum culture resulted negative for any growth. The patient was started on amphotericin B 5 mg/kg q24 hours as soon as she reached the higher care facility. Unfortunately, her condition deteriorated, necessitating the use of vasopressors to manage worsening shock and resulting in kidney injury. Subsequently, she experienced a cardiac arrest and passed away shortly thereafter.
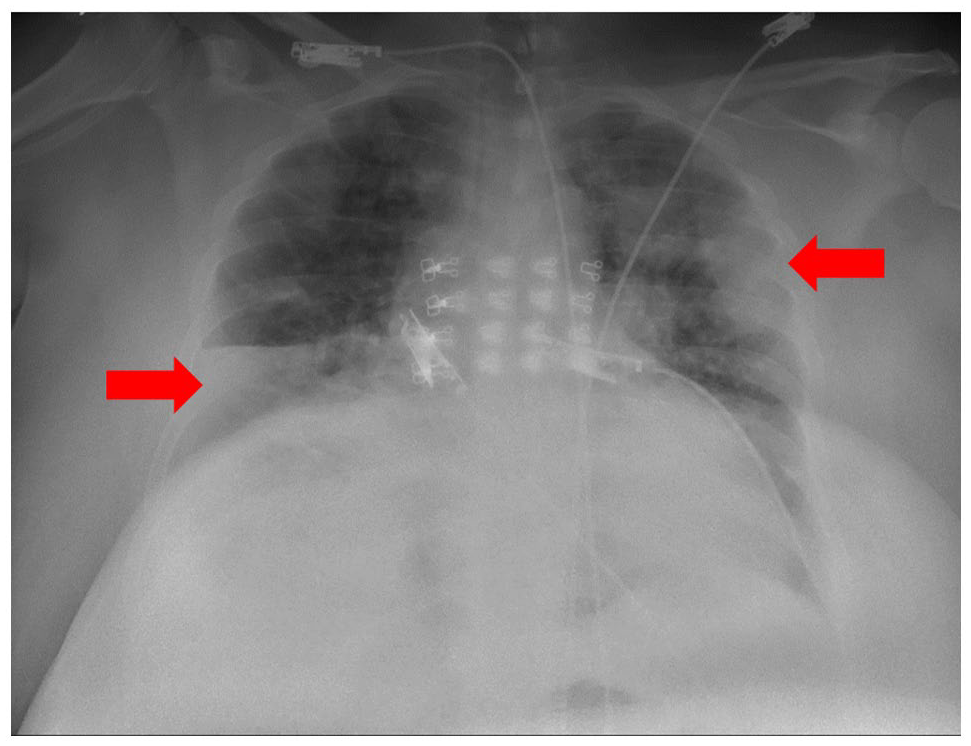
Bilateral infiltrates (red arrows) are seen in the posteroanterior view of the chest x-ray on admission.
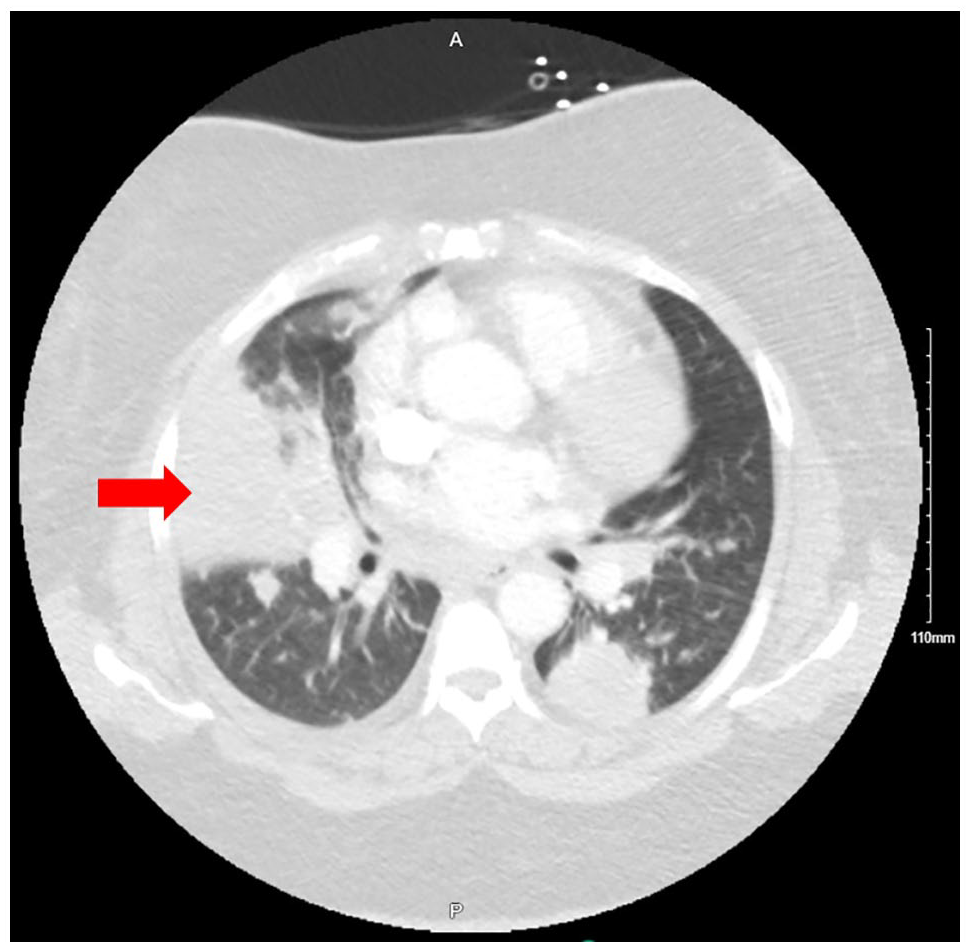
Bilateral patchy infiltrates are seen in the chest computed tomography more pronounced in the left lung base taken on admission. Red arrow shows patchy infiltrate in the right middle lobe.
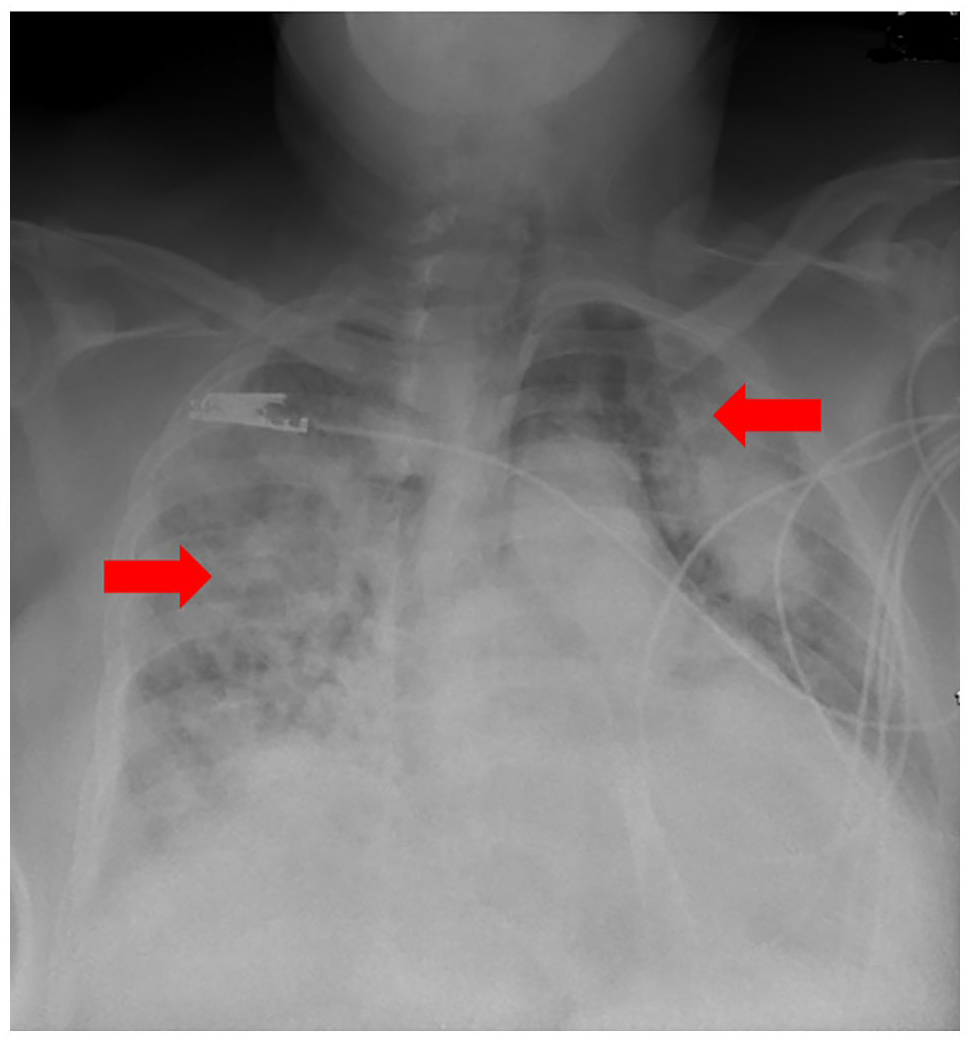
On day 4, new infiltrates (red arrows) developed compared with the initial chest x-ray.
Acute respiratory distress syndrome is a fatal complication of blastomycosis. This case report highlights the importance of early diagnosis and treatment of blastomycosis.
Discussion
B dermatitidis is a dimorphic fungus that is traditionally found in Mississippi and Ohio River Valley areas. It is an uncommon granulomatous disease. 1 Blastomyces spores inhabit the soil and infection occurs on inhalation of spores.
Risk factors for severe blastomycosis infection include pneumonia, obesity, diabetes mellitus, and immunosuppression. Immunocompromised patients required more frequent hospitalizations compared with immunocompetent patients. 2 Infection can be seen more commonly in young adults; more in men than in women. It can be seen in all races but seen more in African Americans. 3
The approximate incubation period for blastomycosis symptoms to develop is 30 to 105 days from inhalation of spores. The traditional progression of disease begins with pulmonary symptoms in 70% to 79%, with the next common site being skin, which is cutaneous mycosis. 1 Symptoms can range from self-limited to serious complications like ARDS 4 and cavitatory lesions. Gullapalli et.al presented a case of cavitation in the lung secondary to blastomycosis infection and was successfully treated with 1 year of itraconazole treatment. 5
The development of ARDS in blastomycosis is not completely understood, but is believed to result from a combination of factors, including direct lung tissue damage, immune response, and cytokine storm caused by blastomycosis. Apart from the factors mentioned, blastomycosis can contribute to ARDS by inducing additional complications, including pneumonia, acute lung injury, and sepsis which in turn can lead to ARDS. 1 Individuals at higher risk of developing ARDS from blastomycosis include those who are immunocompromised, older adults, and those with chronic lung conditions like asthma or chronic obstructive pulmonary disease. 1 A combination of abovementioned factors can be considered as the reasons for development of ARDS in our patient.
Although ARDS is a rare complication in blastomycosis, it carries high mortality rates ranging from 50% to 90%. 6 Sometimes the consolidation on chest x-ray from blastomycosis is misdiagnosed as consolidation from community-acquired pneumonia that will result in delayed diagnosis and delayed treatment. Sputum and BAL are helpful in diagnosing pulmonary blastomycosis. 7 Some of the common radiological findings like consolidation, nodules, cavitation, lymphadenopathy, and cavitary lesions can be seen. 5 Antigen detection can be done but has low specificity due to cross-reactivity with Histoplasma like in our patient. 8 Hence, although serum antigen is positive, bronchoscopy with BAL cultures was done to confirm the diagnosis. 8
Cutaneous blastomycosis usually occurs secondary to hematogenous spread and resembles verrucous skin lesions. 3 Occurrence of central nervous system (CNS) involvement is seen in 5% to 10% of patients with systemic blastomycosis. Brain magnetic resonance imaging and lumbar puncture can be done to diagnose CNS blastomycosis. 9 However, blastomycosis can involve almost all organs in the body. A thorough history including the patient’s occupation and physical examination is important in suspicion of blastomycosis to prevent delay in diagnosis and management. 7
In the Cooperative Mycoses Study of the National Communicable Disease Center, a greater relapse rate was seen in patients who received less than a total of 1.5 g of amphotericin B. Outcomes of blastomycosis are determined by several factors like dosage of medication and cellular immunity. 10 For a moderately severe to severe presentation of either pulmonary or disseminated extra pulmonary blastomycosis, treatment is initiated with lipid formulation of amphotericin B 3 to 5 mg/kg daily for 1 to 2 weeks or until improvement is noted. 11 Amphotericin B is associated with nephrotoxicity and may limit the duration of treatment. Monitoring of electrolytes and creatinine is essential to monitor nephrotoxicity. 11
From March 2020, retrospective cohort study published by Rush et al included 1848 patients who were diagnosed with blastomycosis; 11.9% patients required mechanical ventilation, with approximately 40% risk of mortality. 12
Recently, extracorporeal membrane oxygenation (ECMO) has become a rescue tool in treating refractory blastomycosis-associated ARDS. Early appropriate antimicrobial therapy and transfer to a facility with ECMO plays a key role in treatment of rapidly deteriorating patients. 13
Conclusion
This case report highlights the importance of early diagnosis and treatment of blastomycosis for a favorable outcome. Acute respiratory distress syndrome is a serious complication of blastomycosis, and it can be fatal. It also draws light on the fact that fungal infections like blastomycosis can also be seen in immunocompetent people. The patient in this case had a number of risk factors for blastomycosis, including her asthma and diabetes mellitus. She also had a delayed diagnosis, which may have contributed to her poor outcome. Acute respiratory distress syndrome secondary to blastomycosis is seldom seen but has a very high mortality rate, as high as 90%. Acute respiratory distress syndrome is a difficult condition to treat, with very few effective therapeutic modalities, which can improve patient’s survival.
Footnotes
Authors’ Note
The case was presented as a poster at ATS 2023 conference on May 23, 2023, at Washington, DC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because the patient has expired, which is consistent with the local governing institutional review board.