
Abstract
Tumor lysis syndrome (TLS) occurs when large numbers of tumor cells lyse and release their contents, causing electrolyte derangements and renal injury. It is an uncommon complication of solid tumors and occurs most commonly after cytotoxic therapy rather than spontaneously. In this article, we describe a case of spontaneous TLS in a patient with squamous cell carcinoma of the lung. We also present a literature review of spontaneous TLS occurrence in solid tumors.
Introduction
Tumor lysis syndrome (TLS) occurs when lysed tumor cells release intracellular ions and uric acid into the bloodstream, causing electrolyte derangements and renal injury. 1 This effect requires lysis of significant quantities of tumor cells and most commonly occurs in high-grade cancers, especially hematologic malignancies with high tumor cell burden. It is most often precipitated by the initiation of cytotoxic therapy. Less commonly, TLS can occur spontaneously in hematologic tumors in the absence of cytotoxic therapy or in non-hematologic solid tumors after starting chemotherapy. It is even more uncommon for TLS to occur spontaneously in non-hematologic solid tumors.2-5 Here, we present a case of spontaneous TLS in metastatic squamous cell carcinoma of the lung.
Case
A 58-year-old male patient with an 80 pack-year smoking history was transferred to our hospital for acute on chronic right hip and thigh pain. Four days prior, he had presented to an outside hospital reporting a 4-month history of worsening right thigh and hip pain, described as a “tight band sensation” over the right thigh. Laboratory results at that time were unremarkable but magnetic resonance imaging (MRI) of the right hip showed an aggressive destructive bony lesion at the center of the proximal femoral neck with posterior exophytic component and cystic necrosis (Figure 1). He was discharged home, with plans to follow up with orthopedic surgery for likely metastatic malignancy versus less likely primary bone cancer.

Right hip magnetic resonance imaging (MRI) demonstrated an aggressive bony lesion at the center of the proximal femoral neck with posterior exophytic component and cystic necrosis.
On the day of his presentation to our facility, the patient developed acute onset severe right hip pain when getting out of bed. He again presented to the outside hospital and was diagnosed with a new pathologic intertrochanteric hip fracture for which he was transferred to our hospital. His physical examination was notable for cachexia and coarse pulmonary crackles and rhonchi throughout all lung fields. His laboratory results showed sodium 107 mmol/L, potassium 7.8 mmol/L, phosphorus 6.7 mg/dL, uric acid 10.6 mg/dL, lactate dehydrogenase 1233 U/L, and serum creatinine 6.15 mg/dL. The electrocardiogram (EKG; Figure 2) showed pronounced widening of the QRS and peaked T waves. Biopsy of the right thigh mass showed metastatic squamous cell carcinoma of the lung. A computed tomography scan of the lung (Figure 3) was performed, which showed an irregular, hypodense right hilar lesion measuring 6.2×2.1 cm and enlarged right supraclavicular and subcarinal lymph nodes. He was diagnosed with spontaneous TLS (sTLS) secondary to metastatic squamous cell lung cancer.

Electrocardiogram (EKG) showed pronounced widening of the QRS and peaked T waves consistent with sequelae of hyperkalemia.

Computed tomography (CT) scan of the chest demonstrated a 6.2 × 2.1 cm irregular, hypodense right hilar lesion.
He received rasburicase and underwent renal replacement therapy in the intensive care unit for 2 days, with resolution of his electrolyte derangements, after which he was transferred to the general medicine floor and underwent a total right leg amputation for treatment of his pathologic fracture. He declined any medical treatment for his metastatic cancer, was ultimately discharged on hospice, and died within 6 months.
Discussion
Tumor lysis syndrome is an oncologic emergency that usually occurs following the induction of cytotoxic therapy. Published mortality rates vary from 7% to 33%.3,4,6 It is defined by the Cairo-Bishop criteria and has both clinical and laboratory criteria for diagnosis (Table 1).
Cairo-Bishop Criteria for Diagnosis of Tumor Lysis Syndrome. 7 .
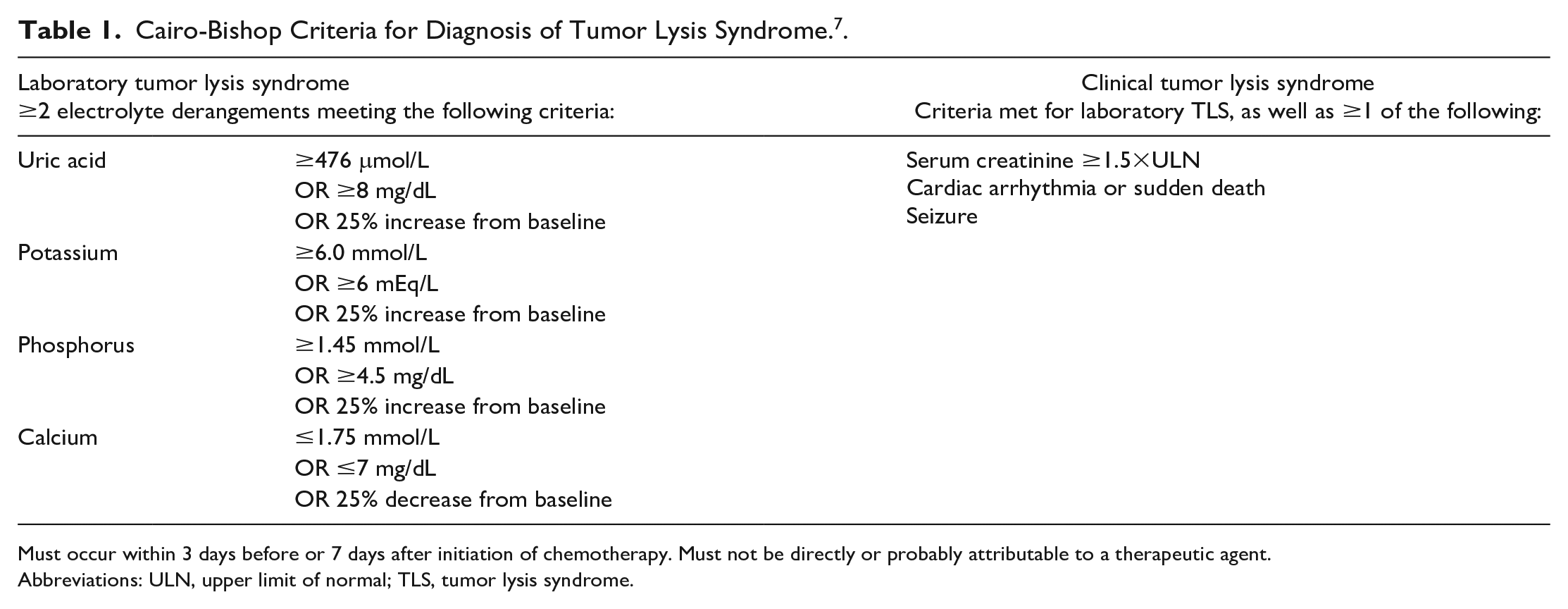
Must occur within 3 days before or 7 days after initiation of chemotherapy. Must not be directly or probably attributable to a therapeutic agent.
Abbreviations: ULN, upper limit of normal; TLS, tumor lysis syndrome.
It occurs most often in hematologic malignancies, but solid tumors represent about 20% of cases. 4 Less commonly, TLS can occur spontaneously in the absence of cytotoxic therapy. This phenomenon, known as sTLS, is most often seen in hematologic malignancies but is increasingly reported in solid tumors. 8 sTLS in solid tumors, which is more likely to occur with high tumor burden and metastatic disease, is associated with high morbidity and mortality. 9
Spontaneous TLS has been reported to occur in numerous types of solid cancers. Review of the literature shows a total of 83 published cases of sTLS in adult patients. Table 2 summarizes the reported cases of sTLS in the literature and denotes the specific tumor type and associated all-cause mortality (whether the patient was noted to have died at the time of the publication). We did not include cases in pediatric patients or cases in which the patient had recently received chemotherapy, radiation, or hormone therapy. Cases in which the patient received corticosteroids or had a remote history of chemotherapy were included. The majority of these cases involve small cell lung cancer and prostate cancer, which make up 16.9% and 14.5% of total cases, respectively. Our case represents the third case of spontaneous tumor lysis occurring in squamous cell lung cancer. All-cause mortality in these 83 cases of sTLS in solid tumors is 59%, but the small sample size limits our ability to draw conclusions from these data. In addition, it should be noted that not all deaths were directly due to the complications of sTLS. Many patients recovered from their electrolyte abnormalities but ultimately succumbed to their advanced cancer. Others declined treatment or were transitioned to hospice, and not all cases provide information about the patient’s long-term outcome. However, there is undoubtedly significant mortality associated both with complications of sTLS and with the malignancies that cause it, which are usually advanced with significant tumor burden.
Published Cases of Spontaneous Tumor Lysis Syndrome in Solid Tumors.

Although sTLS is defined as TLS that occurs in the absence of cytotoxic therapy, our case and several others in the literature suggest that there may be other factors that can increase the risk of TLS, especially in pediatric patients. Steroid therapy is known to be cytotoxic in hematologic malignancies, but has also preceded TLS in several cases of solid tumors in which it has no cytotoxic effect.54,72,85 There have also been a number of cases of sTLS occurring during manipulation of tumors. sTLS has been noted to directly follow intra-abdominal lymphoma debulking, 86 endoscopic retrograde cholangiopancreatography (ERCP) with gastric neuroendocrine tumor biopsy, 35 open cholecystectomy with wedge liver biopsy of metastatic neuroendocrine carcinoma, 21 resection of pediatric hepatoblastoma 87 and nephroblastoma, 88 and pediatric lymphoma staging laparotomy. 89 Hepatic transarterial embolization for hepatic metastases of a neuroendocrine tumor was also associated with TLS in 1 case, 76 and a temporal relationship has been observed between TLS and both sustained high fever 90 and anesthesia administration 91 in pediatric patients. In the case of our patient, sTLS occurred shortly after a pathologic fracture of tumor-containing bone. Given that sTLS has been known to occur with surgical manipulation of tumors, it is possible that disruption of the tumor due to the fracture could have contributed to our patient’s presentation.
It is also important to note that patients may present with sTLS without any known or prior suspicion for malignancy, which was the case for 15 of the patients in our literature review. This, along with the increasing number of reported cases of sTLS in both hematologic and solid cancers, highlights the importance of having a high index of suspicion for TLS in patients presenting with classic laboratory or clinical abnormalities, even without a cancer diagnosis. In patients presenting with such findings without a known malignancy, an underlying malignancy should be sought.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views presented above are those of the authors and do not necessarily represent the views of the DoD or its components.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for publication provided by Madigan Army Medical Center; the authors received no external financial support for the research, authorship, or publication of this article.
Prior Presentation of Abstract Statement
This case was presented as “A case of spontaneous tumor lysis in squamous cell lung cancer” at the 2022 Triservice ACP Chapters Annual Meeting in San Antonio, TX, September 7 to 10, 2022.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because our institution does not require informed consent for reporting individual cases if patient information is fully anonymized.