
Abstract
There are few cases in the literature demonstrating vasculitis induced by tumor necrosis factor–α. There exist even fewer cases of systemic inflammation involving the skin, nerves, and kidneys. Here, we present a novel case of a 27-year-old man with Crohn disease refractory to multiple medications, most recently treated with infliximab. He presented with a 3-week history of non-blanching palpable petechial rash involving his bilateral extremities and right upper extremity as well as lesions with black eschar around his ankles. He was found to have refractory cutaneous small vessel vasculitis, nephrotic range proteinuria, and small fiber neuropathy. This case describes the evaluation and treatment of systemic small vessel vasculitis in the setting of infliximab therapy.
Introduction
Tumor necrosis factor (TNF)-α inhibitors are a rare cause of systemic vasculitis. There exists minimal literature that has quantified the occurrence of vasculitis following TNF-α therapy. We review the largest and how it relates to this case (Figure 1), 1 expanding on the literature and highlighting the rarity of this patient’s constellation of symptoms.
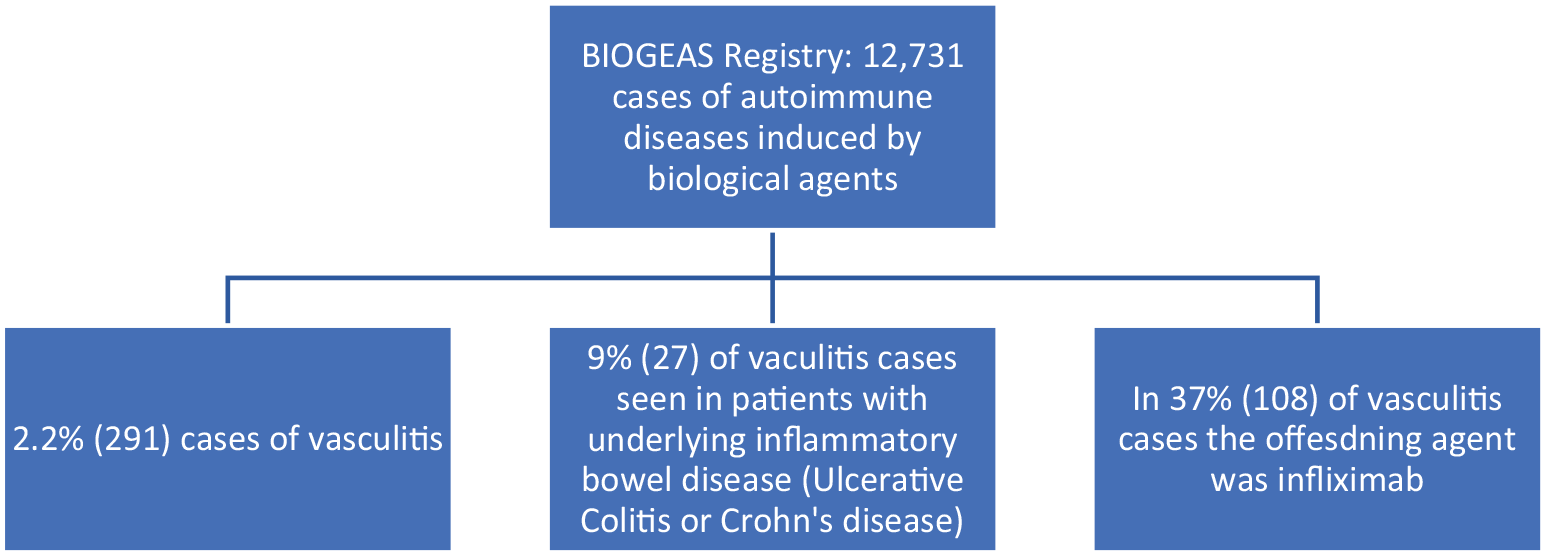
Occurrence of vasculitis in large case review, demonstrating the rarity of vasculitis seen in inflammatory bowel disease treated with infliximab. 2
Case Presentation
A 27-year-old man with a history of refractory Crohn controlled on infliximab presented endorsing 1 week of rash that started on ankles, spreading to the rest of legs accompanied by lower extremity swelling and pain. Inflammatory bowel disease (IBD) treatment history includes adalimumab, azathioprine, vedolizumab, and ustekinumab. Infliximab was started 7 months prior to presentation, and the last infusion was 6 weeks prior to presentation.
Work-up showed negative antinuclear antibody (ANA), antineutrophilic cytoplasmic antibody (ANCA), COVID/respiratory viral panel, tuberculosis, connective tissue panel, cryoglobulin, rheumatoid factor, serum protein electrophoresis, borrelia, and gonorrhea/chlamydia; nonreactive HIV and hepatitis panel; normal C3, C4, thyroid stimulating hormone, and creatine kinase; and mildly elevated C-reactive protein (CRP)/erythrocyte sedimentation rate (ESR). Skin biopsy showed leukocytoclastic vasculitis. The patient was treated with intravenous (IV) dexamethasone and 40 mg prednisone. The patient reported worsening swelling and arthralgias, was transitioned to IV Solu-Medrol 125 mg q6h with improvement of symptoms, and was discharged after 5 days with oral steroids.
Three weeks after discharge, the patient re-presented with gradual worsening skin manifestations and pain. Work-up showed negative blood cultures, IgA of 377 (60-400 mg/dL), and urinalysis with red blood cells and protein. Prednisone was increased from 40 to 60 mg daily. The patient transferred to our hospital for access to subspecialty care.
On admission, physical examination revealed bilateral lower extremity, forearm, and abdominal petechial rash with healing ulcers (Images 1-3); profound allodynia and neuralgias in bilateral lower extremities; and decreased range of motion in right hand and movement of feet limited by pain.

Black eschar posterior left ankle; Edematous foot with petechial rash; Demonstrates the diffuse nature of cutaneous vasculitis.
Labs showed IgA of 334, ANA <1:80, unremarkable ESR/CRP, negative ANCA/proteinase 3 (PR3)/myeloperoxidase, 24-hour urine protein with 5 g protein and 2 g albumin, and nephrotic range proteinuria without overt nephrotic syndrome. Skin biopsy showed granular IgA staining of superficial dermal blood vessels. Kidney biopsy showed IgA nephropathy with mild activity and no significant evidence of chronicity. The glomeruli showed focal, mild mesangial expansion, and increased cellularity. The tubular structures showed patchy tubular simplifications consistent with mild tubular injury. The glomerulus showed granular mesangial staining for IgA (3+) and C3 (2+). Electromyography was deferred. The patient was treated with intravenous immunoglobulin, followed by 40 mg IV methylprednisolone BID. With improvement of symptoms, the patient was transitioned to and discharged on prednisone 50 mg BID.
Discussion
TNF-α inhibitor–induced vasculitis is challenging to diagnose due to the difficulty of distinguishing between vasculitis caused by an offending drug and underlying disease. A way to elucidate the diagnosis is mapping the temporality of medication and the onset of symptoms. Another indication of the etiology is determining the activity of the underlying disease.
The etiology of TNF-α inhibitor–induced vasculitis is not completely understood. Two main mechanisms are prevalent in the literature. We will first discuss immune complex–mediated type 3 hypersensitivity reaction. Induction of ANA occurs in 23% to 57% of patients, induction of anti-ds DNA antibodies occurs in 9% to 33%, the association is unknown between vasculitis and these antibodies, and it is posited that the development of antibodies against anti-TNF-α agents and TNF-α inhibitor immunocomplexes leads to this reaction and complement activation. 3 These immune complexes precipitate on small vessels inducing a local reaction.2,4 Support for this hypothesis comes from the fact that discontinuation of biologics with the addition of immunosuppressants leads to recovery. 2
Another prevalent hypothesis is cytokine imbalance. TNF-α inhibitor induces a cytokine imbalance due to the suppression of TNF, resulting in preferential expression of Th2 cells over Th1 cells inducing an inflammatory state leading to autoimmune disease. 3 A less popular hypothesis is drug toxicity causing direct insult.
The leading treatment is discontinuation of the offending therapy. Corticosteroids are used in severe, refractory cases. Additional immunosuppressant agents are less frequently utilized.
The US Food and Drug Administration database showed relapses occurred in 67% of patients who restarted the offending agent. A study showed relapse occurred in 33% of patients who were started on a different anti-TNF-α. 5 In another study, 41 patients had their medication stopped, and 4 were able to maintain therapy. In about half of the 41 patients who stopped medication, they resumed therapy with a different biological with only 4 recurrences. There was 71% reactivation with reintroduction of the same agent. 4 It is difficult to draw conclusions due to the small sample; however, we do not recommend reintroducing the same agent and, if possible, avoiding the drug class.
Conclusion
Small vessel vasculitis is a rare but known side effect of TNF-α inhibitors. This must be shared with the patient as a risk-benefit analysis before commencing treatment. Other important information includes the length of treatment and prognosis. Many patients need immunosuppression for months which comes with risk. Fortunately, of 72 cases described in a systematic review, 75% of patients had complete remission. 4 Future areas of study include genetic susceptibility and prediction of adverse drug response. Other areas include the safety of reintroduction of biologics in patients with a history of adverse reaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.