
Abstract
A 54-year-old man presented with significant ST-segment elevations noted on both channels displayed on the mobile cardiac outpatient telemetry (MCOT). Pertinent cardiac history was remarkable for syncope and episodes of atypical chest pain. The latter were described as infrequent and not associated with exercise intolerance. His syncopal episodes were described as occurring mostly in the mornings after the use of the restroom. Episodes happen 1 or 2 times a year since 2015. Patient had undergone thorough investigation with no significant findings. An MCOT was prescribed since frequency of symptoms has recently increased. Significant ST-segment elevations were noted. The patient described atypical chest pain and a sensation of presyncope during these recordings. He was urgently admitted, and a coronary angiogram revealed no epicardial luminal stenosis. However, the presence of sluggish coronary flow was suggestive of possible vasospastic angina. No ST-segment changes were noted during his coronary angiogram. The remarkable element portrayed by this case hinges in showing the unique utility of MCOT, as the most uncharacteristic diagnostic tool, in identifying transient ST-segment elevations that finally led to the diagnosis.
Introduction
In contrast to the standard electrocardiogram (ECG), which provides a brief summary of cardiac electrical activity over a period of 10 seconds, ambulatory ECG monitoring provides a view of ECG data over an extended period, thereby allowing us to evaluate the dynamic and transient cardiac electrical activity. The most common ambulatory ECG application is used in the diagnosis and assessment of potential cardiac arrhythmias (such as in patients with syncope or presyncope) or conduction abnormalities; however, this application extends beyond that to have a role in stratification of certain cardiomyopathies, in assessing the effectiveness of arrhythmia therapy, and in the evaluation of silent ischemia.
Ambulatory ECG monitoring has experienced significant improvements since its initial inception in 1961 by Norman G. Holter. 1 Overtime and with these changes in electrocardiographic ST-segment analysis, there has been a renewed interest in using Holter Monitoring, especially in multicenter clinical trials, to analyze ST-segment. 2 However, there has been no consensus on how to define an ischemic event. These assessments have been largely limited to ST-segment depressions. In contrast, the potential utility of ST-segment elevation during routine remote cardiac monitoring has been limited to patients with transient left ventricular apical ballooning. 3
Since there is paucity of data with regards to the potential assessment of ST-segment and unmet need to come to a consensus and revisiting current guidelines; we hope that our case report serves as evidence to galvanize efforts in reviving the utility of remote cardiac monitoring in ischemic disease assessment.
Case Presentation
A 54-year-old male patient with a past medical history significant for hypertension, dyslipidemia, and gout presented to the cardiology clinic for chief complaints of chest burning sensations and a syncopal episode that would occur mostly in the mornings before he uses the restroom. He has had an extensive cardiac work up since the evolution of his symptoms since 2015 to include a normal Holter, stress test, tilt table, and an echocardiogram. His symptoms were never exertional with reported good exercise tolerance as he claims to walk 10 miles daily to his work. Given the persistence of his symptoms with significant diaphoresis and bothersome palpitations, a mobile cardiac outpatient telemetry (MCOT) device was requested.
During his period of wearing the device, he had an episode of chest burning with profuse diaphoresis in which significant ST-segments elevations were recorded (Figures 1-4). Therefore, the patient was contacted and brought immediately to the hospital and a coronary angiogram was performed.
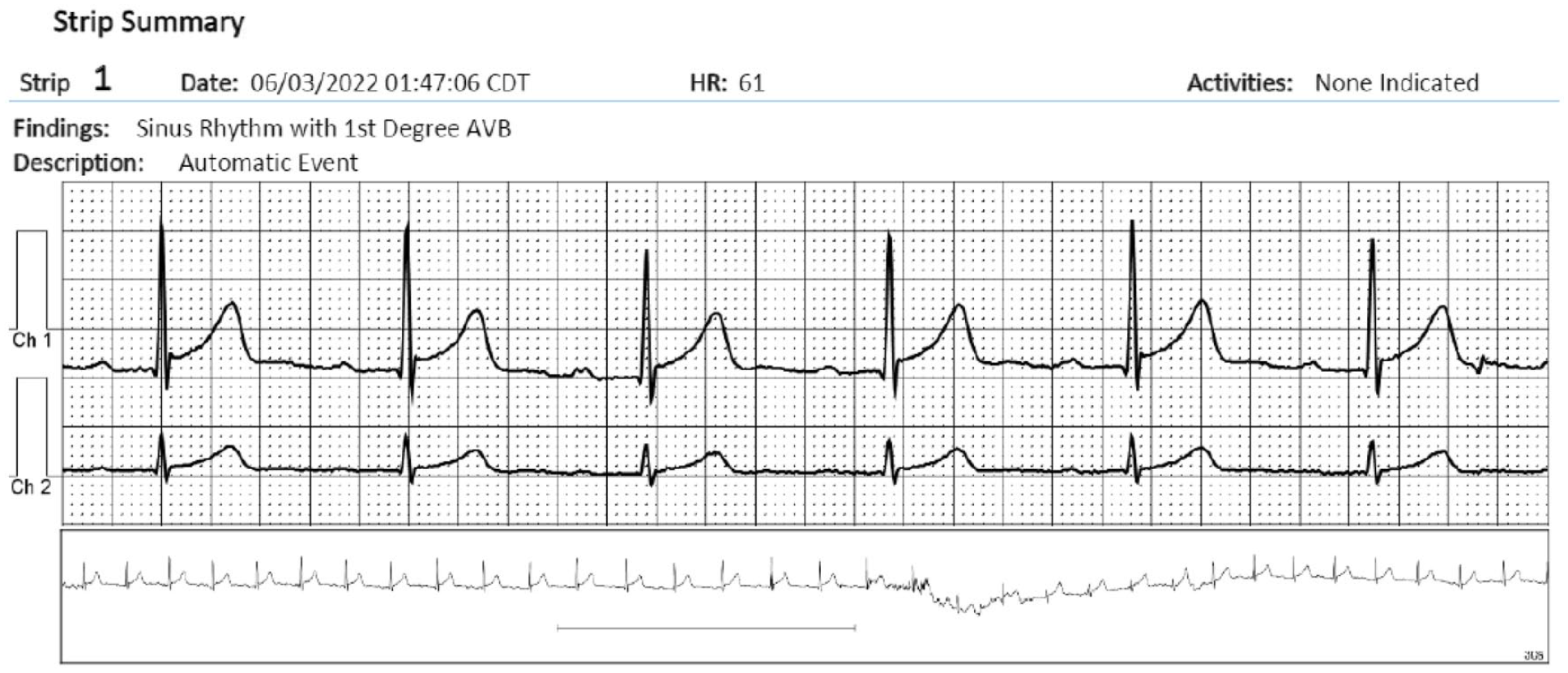
Random mobile cardiac outpatient telemetry recording showing normal sinus rhythm with a first-degree AV block and minor concave up ST-segment change, suggestive of early repolarization.

Random mobile cardiac outpatient telemetry recording showing normal sinus rhythm with a first-degree AV block and a normal ST-segment without early repolarization changes.

Normal sinus rhythm with first-degree AV block and marked (tombstone) ST-segment elevations.

Prolonged transmission showing normal sinus rhythm with transient third-degree AV block and persistent (tombstone) ST-segment elevations. Arrows indicating P-waves.
Upon admission, his ECG showed normal sinus rhythm without ST-segment deviation in terms of either depression or elevation. His high-sensitivity troponins were 3.5 pg/mL (0-14.4 pg/mL). An echocardiogram showed a normal ejection fraction with no wall motion abnormalities and no other structural abnormalities. Cardiac catheterization demonstrated no significant coronary artery disease but showed sluggish flow through the left anterior descending artery that could be indicative of vasospastic angina (Figures 5 and 6).

Representative coronary angiogram showing patent RCA taken at a left anterior oblique cranial 30° angulation, coronary artery LAD with the image acquired in the anteroposterior cranial 36° angulation and a small LXC at a right anterior oblique caudal 30° angulation.
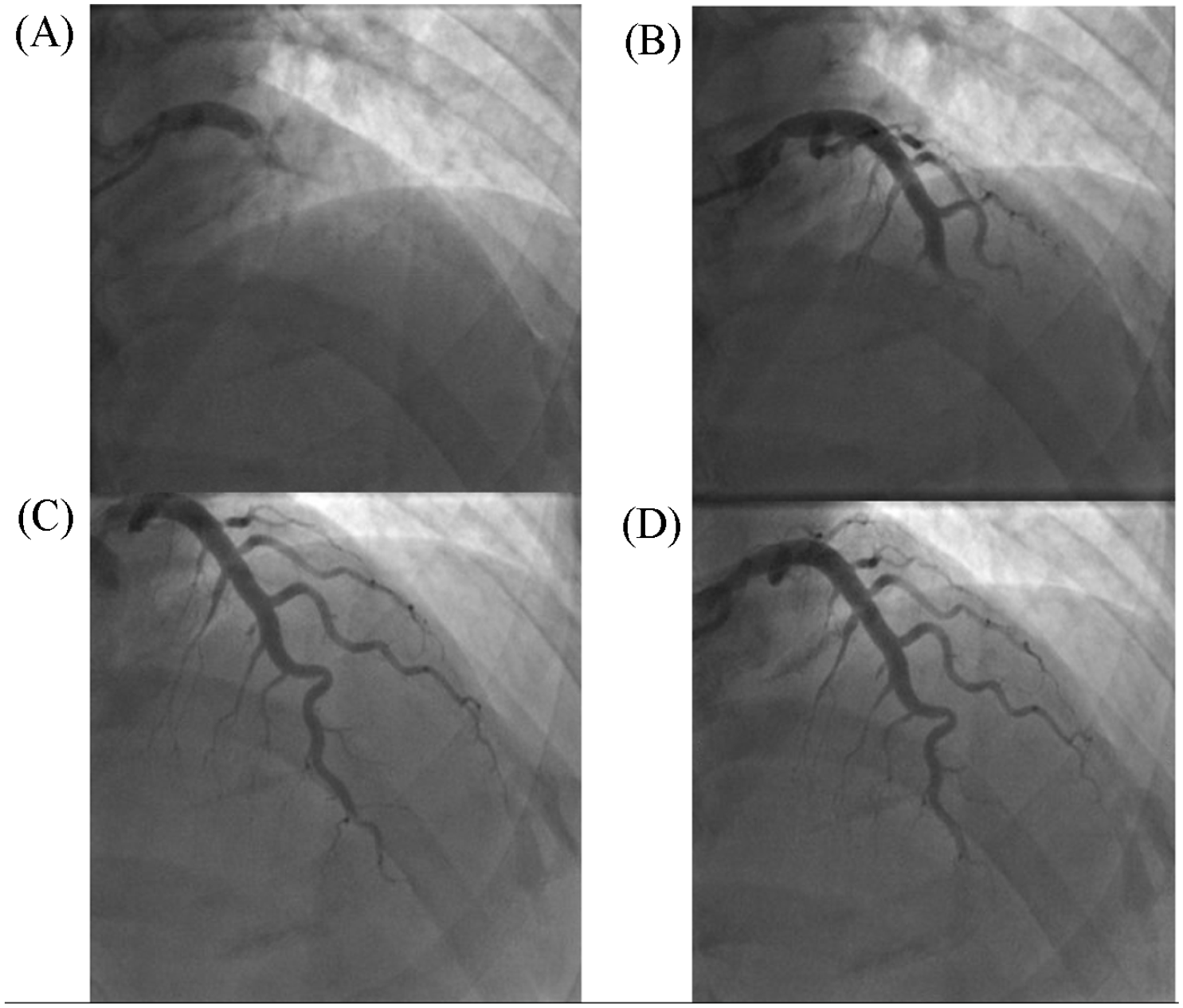
Temporal shots of the coronary artery LAD all obtained in the right anterior oblique caudal 30° angulation. Frames were taken at 8 frames per second. (A) Taken at 1 second; (B) Taken at 2 seconds; (C) Taken at 4 seconds, and (D) Taken at 5 seconds. These images represent the sluggish flow seen in the LAD coronary artery.
The initial differential diagnosis for patients presenting with acute ST-segment elevations must include the most serious conditions such as acute myocardial infarction, acute pericarditis, hyperkalemia, acute pulmonary embolism, and coronary artery spasm (CAS) and promptly evaluated. 4
In contrast, there are patients that can present with persistent ST-segment elevations in which the differential diagnosis would include a long-term transmural infarction with aneurysmal formation, repolarization abnormalities such as bundle-branch blocks or early repolarization, Brugada syndrome, left ventricular hypertrophy, massive hiatal hernias, and in cases of malignancies such as infiltration of the heart, breast cancer, lung cancer, and cases of pleural mesothelioma and melanoma.4,5
In this case, the occurrence of transient ST-segment elevation associated with symptoms was most likely due to coronary vasospasm, given the sequence of temporal events and findings of coronary angiography.
Management of CAS has been largely based on identifying and avoiding precipitating factors. These factors can include cigarette smoking and cocaine use, sympathomimetic agents that is used to augment our catecholamines and nonselective beta-blockers. 6 Other risk factor that has been associated with CAS is magnesium deficiency. 6 The mainstays of treatment for CAS besides avoiding and correcting precipitating factors are Calcium-channel blockers and nitrates. 6 Recent off-label use of riociguat was used to treat refractory CAS. 7
Patient has done well on follow-up with resolution of symptoms on diltiazem, a calcium channel blocker.
Discussion
Vasospastic angina previously known as Prinzmetal angina is characterized by episodes of rest angina attributable mainly to coronary artery vasospasm that promptly responds to short-acting nitrates. 8 Recently, CAS has been associated with either ST-segments elevations or depressions; hence, the term vasospastic angina is more commonly used. Vasospastic angina can also present in patient with coronary stenosis (>70%) that resolve after administration of intracoronary nitroglycerin as well as in patients who had prior coronary artery bypass grafting for left main stenosis that on follow-up angiography might not had further evidence of left main disease.6,9
The prevalence of vasospastic angina is difficult to assess since provocative spasm testing with intracoronary acetylcholine is not widely performed in contemporary cardiology practice. Consequently, prevalence estimates are subject to patient selection bias for identifying vasospastic angina. Considering this limitation, in a recent meta-analysis of 24 studies in more than 6500 patients with suspected coronary disease and no epicardial obstructive coronary lesions, the prevalence of epicardial artery vasospastic angina was 40% (95% CI: [33%, 47%]). 10
Some studies suggest that the prevalence of vasospastic angina is similar between men and women; 11 however, in certain populations, the prevalence was shown to be higher in males taking into consideration the confounding factor of higher smoking rates in males.12,13 Vasospastic angina can be caused by either a focal or diffuse spasm of the smooth muscle in the arterial wall resulting in high-grade obstruction of the epicardial coronary artery.14,15 This can possibly happen either due to, autonomic nervous system dysfunction, endothelial dysfunction, vascular smooth muscle hyperactivity, microvascular spasm, allergy or smooth muscle dysfunction, often coexisting with coronary spasm.16-23
Diagnostic criteria for vasospastic angina include: (1) nitrate-responsive angina that typically occurs at rest or at night and associated with transient ischemic ST-segments changes, (b) CAS on angiography (more than 90% blood flow limitation). Of course, obstructive coronary disease must be excluded first through ECG and angiography.
When a diagnosis is established, an initial therapy of sublingual nitroglycerin should be considered along with smoking cessation if that was the case. The mainstay therapy for vasospastic angina is calcium channel blockers. If symptoms persist, the use of nicorandil, ranolazine, and enhanced external counter pulsation (EECP) can be considered.24-26 Recent off-label use of riociguat was used to treat refractory cases. 7
In our case, we sought not to seek additional measures as angiographically there were no evidence of epicardial luminal plaques, but the flow to the left anterior descending artery was sluggish to strongly suggest the diagnosis.
To the best of our knowledge, this is the first case to be reported of transient ST-segment elevations identified during routine MCOT monitoring resembling the tombstone changes seen in acute myocardial infarction. Traditionally, most ST-segment deviations seen on remote cardiac monitoring is reported as ST-segment depressions, indicating episodes of transient ischemia.27-30 These early studies hinted at the value of identifying transient ST-segment changes as valuable, particularly, as it identified patients at higher risk. 29
Aside from improvement in the quality of tracings, MCOT devices also offer the availability of continuous listening; recording every heartbeat for up to 30 days with the flexibility of storing data locally or when needed, data can be transmitted in real time for immediate assessment as seen in our case. 31
Therefore, this new technology might offer us the opportunity of revisiting the potential value of analyzing ST-segment changes during routine activities, as this was seen as a maker of underlying silent coronary disease, particularly among diabetics. 32 Obviously, this opens new doors that can further improve cardiac risk assessment in this technologically savvy world that hopes to improve the use of remote technology to improve cardiovascular disease management. 33
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient for their anonymized information to be published in this article.